文献精选
Antoine E. Roux,1 Chunlian Zhang,1 Jonathan Paw,1 Jose´ Zavala-Solorio,1 Evangelia Malahias,1 Twaritha Vijay,1 Ganesh Kolumam,1 Cynthia Kenyon,1 and Jacob C. Kimmel1,2,3, * 1Calico Life Sciences, LLC, 1170 Veterans Blvd, South San Francisco, CA 94080, USA
2Present Address: NewLimit, Inc., 901 Gateway Blvd, South San Francisco, CA 94080, USA
3Lead contact
*Correspondence: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。 https://doi.org/10.1016/j.cels.2022.05.002
SUMMARY
Partial pluripotent reprogramming can reverse features of aging in mammalian cells, but the impact on somatic identity and the necessity of individual reprogramming factors remain unknown. Here, we used single-cell genomics to map the identity trajectory induced by partial reprogramming in multiple murine cell types and dissected the influence of each factor by screening all Yamanaka Factor subsets with pooled single-cell screens. We found that partial reprogramming restored youthful expression in adipogenic and mesenchymal stem cells but also temporarily suppressed somatic identity programs. Our pooled screens revealed that many subsets of the Yamanaka Factors both restore youthful expression and suppress somatic identity, but these effects were not tightly entangled. We also found that a multipotent reprogramming strategy inspired by amphibian regeneration restored youthful expression in myogenic cells. Our results suggest that various sets of reprogramming factors can restore youthful expression with varying degrees of somatic identity suppression. A record of this paper’s Transparent Peer Review process is included in the supplemental information.
Helen C. Fraser1 | Valerie Kuan2,3,4 | Ronja Johnen5 | Magdalena Zwierzyna6 | Aroon D. Hingorani3,4,6 | Andreas Beyer5,7 | Linda Partridge1,8
1 Department of Genetics, Evolution and Environment, Institute of Healthy Ageing, University College London, London, UK
2 Institute of Health Informatics, University College London, London, UK
3 Health Data Research UK London, University College London, London, UK
4 University College London British Heart Foundation Research Accelerator, London, UK
5 Cologne Excellence Cluster on Cellular Stress Responses in Aging-Associated Diseases (CECAD), Medical Faculty & Faculty of Mathematics and Natural
Sciences, University of Cologne, Cologne, Germany
6 Institute of Cardiovascular Science, University College London, UK
7 Centre for Molecular Medicine, University of Cologne, Cologne, Germany
8 Max Planck Institute for Biology of Ageing, Cologne, Germany
Correspondence
Andreas Beyer, Cologne Excellence Cluster on Cellular Stress Responses in Aging-Associated Diseases (CECAD), Medical Faculty & Faculty of Mathematics and Natural Sciences, University of Cologne, Cologne, Germany.
Email: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。
Linda Partridge, Institute of Healthy Ageing, Department of Genetics, Evolution and Environment, University College London, London, UK.
Email: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。
Funding information
Bundesministerium für Bildung und Forschung, Grant/Award Number: HiGHmed 01ZZ1802U; UK Medical Research Council, Grant/Award Number: MR/N013867/1; Dunhill Medical Trust, Grant/Award Number: RPGF1806/67; BenevolentAI; Max- Planck-Gesellschaft; Wellcome Trust, Grant/Award Number: WT 110284/Z/15/Z; Deutsche Forschungsgemeinschaft, Grant/Award Number: CRC1310 and 325931972; British Heart Foundation, Grant/Award Number: AA/18/6/34223; European Research Council (ERC)
Abbreviations: AH, Aging hallmark; ARD, Age-related disease; EBI, European Bioinformatics Institute; ERK, Extracellular signal regulated kinase; GO, Gene Ontology; GSEA, Gene set
enrichment analysis; GWA, Genome-wide association; IFNg, Interferon gamma; MeSH, Medical Subject Headings; NCBI, National Centre for Biotechnology Information; NHGRI, National Human Genome Research Institute; PMID, PubMed unique Identifier; SNP, Single-nucleotide Polymorphism.
This is an open access article under the terms of the Creative Commons Attribution License, which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
© 2022 The Authors. Aging Cell published by Anatomical Society and John Wiley & Sons Ltd.
Abstract
Genetic, environmental, and pharmacological interventions into the aging process can confer resistance to multiple age-related diseases in laboratory animals, including rhesus monkeys. These findings imply that individual mechanisms of aging might contribute to the co-occurrence of age-related diseases in humans and could be targeted to prevent these conditions simultaneously. To address this question, we text mined 917,645 literature abstracts followed by manual curation and found strong, nonrandom associations between age-related diseases and aging mechanisms in humans, confirmed by gene set enrichment analysis of GWAS data. Integration of these associations with clinical data from 3.01 million patients showed that age-related diseases associated with each of five aging mechanisms were more likely than chance to be present together in patients. Genetic evidence revealed that innate and adaptive immunity, the intrinsic apoptotic signaling pathway and activity of the ERK1/2 pathway were associated with multiple aging mechanisms and diverse age-related diseases. Mechanisms of aging hence contribute both together and individually to age-related disease co-occurrence in humans and could potentially be targeted accordingly to prevent multimorbidity.
KEYWORDS
age-related disease, aging, aging hallmarks, genetics, multimorbidity
Aging is characterized by a progressive loss of physiological integrity, leading to impaired function and increased vulnerability to death. This deterioration is the primary risk factor for major human pathologies, including cancer, diabetes, cardiovascular disorders, and neurodegenerative diseases. Aging research has experienced an unprecedented advance over recent years, particularly with the discovery that the rate of aging is controlled, at least to some extent, by genetic pathways and biochemical processes conserved in evolution. This Review enumerates nine tentative hallmarks that represent common denominators of aging in different organisms, with special emphasis on mammalian aging. These hallmarks are: genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, deregulated nutrient sensing, mitochondrial dysfunction, cellular senescence, stem cell exhaustion, and altered intercellular communication. A major challenge is to dissect the interconnectedness between the candidate hallmarks and their relative contributions to aging, with the final goal of identifying pharmaceutical targets to improve human health during aging, with minimal side effects.

Authors
Matthew Simon, Michael Van Meter, Julia Ablaeva, ..., John M. Sedivy, Andrei Seluanov, Vera Gorbunova
Correspondence
该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。 (A.S.), 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。 (V.G.)
In Brief
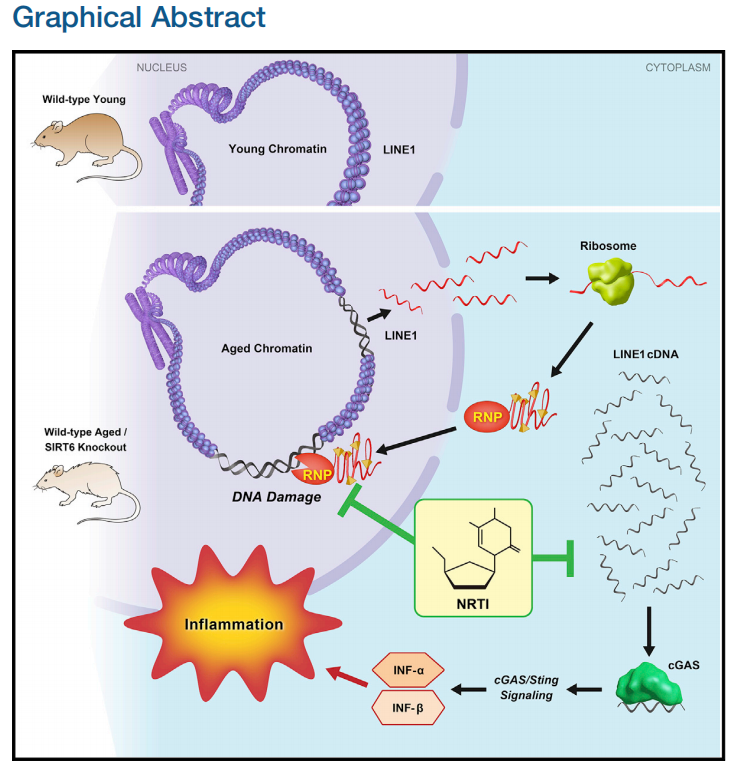
Simon et al. show that LINE1 retrotransposon elements are derepressed in aged and progeroid mice. Cytoplasmic accumulation of LINE1 cDNA copies induced a type I interferon response, through the cGAS DNA sensing pathway, resulting in pathological inflammation. Inhibiting L1 replication significantly improved the health and lifespan of aged mice.
Highlights
● SIRT6 KO mice accumulate L1 cDNA, triggering interferon response via cGAS pathway
● Wild-type aged mice accumulate L1 cDNA and display type I interferon response
● Reverse-transcriptase inhibitors rescue type I interferon response and DNA damage
● Reverse-transcriptase inhibitors extend lifespan and improve health of SIRT6 KO mice
SUMMARY
Mice deficient for SIRT6 exhibit a severely shortened lifespan, growth retardation, and highly elevated LINE1 (L1) activity. Here we report that SIRT6-deficient cells and tissues accumulate abundant cytoplasmic L1 cDNA, which triggers strong type I interferon response via activation of cGAS. Remarkably, nucleoside reverse-transcriptase inhibitors (NRTIs), which inhibit L1 retrotransposition, significantly improved health and lifespan of SIRT6 knockout mice and completely rescued type I interferon response. In tissue culture, inhibition of L1 with siRNA or NRTIs abrogated type I interferon response, in addition to a significant reduction of DNA damage markers. These results indicate that L1 activation contributes to the pathologies of SIRT6 knockout mice. Similarly, L1 transcription, cytoplasmic cDNA copy number, and type I interferons were elevated in the wild-type aged mice. As sterile inflammation is a hallmark of aging, we propose that modulating L1 activity may be an important strategy for attenuating age-related pathologies.
Context and Significance
Mammalian aging is complex and likely reflects accumulated damage to our genes/DNA. Retrotransposons are a special class of parasitic genetic elements that can replicate their DNA within our genes, at times amounting to up to 20% of human DNA. Retrotransposons, such as the commonly occurring L1, have been associated with aging, neurodegeneration, and cancer. University of Rochester scientists uncovered L1 retrotransposons as the culprit in many aspects of accelerated aging in mice, a model for human aging. They also linked these special gene elements to inflammation. Experimentally blocking retrotransposon amplification improved the health and lifespan of mice. Although there is a long road ahead, inhibiting retrotransposon activity, and the related inflammation, could eventually be a therapy for age-related diseases.
