文献精选
袁 悦1 ,纪晓晖1 ,顾敬喜2 ,陈官芝1*
1 青岛大学附属医院皮肤科,山东 青岛
2 山东省郯城县皮肤病防治站,山东 临沂
收稿日期:2024年2月27日;录用日期:2024年3月21日;发布日期:2024年3月29日
摘 要
目的:点阵CO2激光疗法在改善皮肤老化方面已经得到了广泛的应用,由于眶周皮肤的脆弱、易造成瘢痕的特性,目前针对眶周皮肤年轻化的激光治疗开展较少。本研究旨在确定点阵CO2激光联合疗法在眶周皮肤再生表面修复中的有效性和安全性。方法:截至2023年12月01号,在3个主要数据库中进行了系统搜索。纳入的研究包括点阵CO2激光或联合其他疗法来改善眼周老化的有效性及并发症,并报告了治疗的有效性和安全性;多篇文章报道同一组患者时,选择最近的报道完整数据的文章。排除标准包括体外研究、动物研究、未使用点阵CO2激光、专家述评、书信、会议摘要、数据不完整或不能获取、CO2点阵激光治疗但未声明关于眶周皱纹或年轻化的研究。结果:筛选后纳入7项临床试验,共纳入166例患者。研究汇总发现眶周皮肤老化及皱纹深度绝大部分都得到了改善,大多数患者都对这项技术感到满意。研究中发现患者在CO2激光术后耐受性良好,主要产生的并发症有包括红斑(n = 8)、色素沉着过度(n = 8)、渗出、渗血、局部水肿、结痂、疼痛、灼热、瘙痒、水疱等。随访时均再未观察到疱疹感染等其他不良反应。术后7天无瘢痕及表皮萎缩再形成。大多数并发症轻微且短暂。治疗后红斑发生率为0.10 (95% CI:0.03~0.18, p < 0.01),色素沉着发生率为0.08 (95% CI: 0.03~0.16, p < 0.01)。结论:研究发现,点阵CO2激光治疗眶周皮肤年轻化是有效且安全的。由于缺乏高质量的报告,有必要进行更多的试验来证实这些结果。
关键词 年轻化,点阵CO2 激光,眶周,Meta分析
A Systematic Review and Meta-Analysis of Efficacy, Safety, and Satisfaction Rates of Fractional CO2 Laser in Periocular Skin Rejuvenation
Yue Yuan1, Xiaohui Ji1, Jingxi Gu2, Guanzhi Chen1*
1 Dermatology Department, The Affiliated Hospital of Qingdao University, Qingdao Shandong
2 Skin Disease Prevention Station of Tancheng County, Shandong Province, Linyi Shandong Received: Feb. 27th, 2024; accepted: Mar. 21st , 2024; published: Mar. 29th, 2024
Abstract
Objective: Fractional CO2 laser therapy has been widely used in improving skin aging. Due to the fragile and scarring properties of periorbital skin, laser therapy for periorbital skin rejuvenation is rarely carried out now. The aim of this study was to determine the efficacy and safety of fractional CO2 laser combined therapy in periorbital skin regeneration surface repair. Methods: As of December 01, 2023, a systematic search was conducted in three major databases. Included studies included the efficacy and complications of fractional CO2 laser or combined with other therapies to improve periocular aging, and reported the efficacy and safety of the treatment. When multiple articles report on the same group of patients, select the most recent article reporting completedata. Exclusion criteria included in vitro studies, animal studies, no use of a fractional CO2 laser, expert reviews, letters, conference abstracts, incomplete or unavailable data, and studies on periorbital wrinkles or rejuvenation that did not claim fractional CO2 laser treatment. Results: After screening, 7 clinical trials were included, involving a total of 166 patients. The study summary found that periorbital skin aging and wrinkle depth were largely improved, and most patients were satisfied with this treatment. The study found that patients were well tolerated after fractional CO2 laser surgery, and the main complications included erythematosis (n = 8), hyper pigmentation (n = 8), exudation, bleeding, local edema, scab, pain, burning, pruritus, blisters, etc. No other adverse reactions such as herpes infection were observed during follow-up. No scar or epidermal atrophy was found 7 days after surgery. Most complications were mild and short-lived. The incidence of erythema after treatment was 0.10 (95% CI: 0.03~0.18, p < 0.01), and the incidence of hyper pigmentation was 0.08 (95% CI: 0.03~0.16, p < 0.01). Conclusion: It is found that fractional CO2 laser is effective and safe in the treatment of periorbital skin rejuvenation. Due to paucity of high-quality reportings, additional trials are warranted to corroborate these results.
Keywords Rejuvenation, Fractional CO2 Laser, Periorbital, Meta-Analysis
Copyright © 2024 by author(s) and Hans Publishers Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY 4.0).
http://creativecommons.org/licenses/by/4.0/






Carlos Lo´ pez-Otı´n,1,2,3,* Maria A. Blasco,4 Linda Partridge,5,6 Manuel Serrano,7,8,9 and Guido Kroemer10,11,12,*
1 Departamento de Bioquı´mica y Biologı´a Molecular, Instituto Universitario de Oncologı´a (IUOPA), Universidad de Oviedo, Oviedo, Spain
2 Instituto de Investigacio´ n Sanitaria del Principado de Asturias (ISPA), Oviedo, Spain
3 Centro de Investigacio´ n Biome´ dica en Red de Ca´ ncer (CIBERONC), Madrid, Spain
4 Telomeres and Telomerase Group, Molecular Oncology Program, Spanish National Cancer Centre (CNIO), Madrid, Spain
5 Department of Genetics, Evolution and Environment, Institute of Healthy Ageing, University College London, London, UK
6 Max Planck Institute for Biology of Ageing, Cologne, Germany
7 Institute for Research in Biomedicine (IRB Barcelona), Barcelona Institute of Science and Technology (BIST), Barcelona, Spain
8 Catalan Institution for Research and Advanced Studies (ICREA), Barcelona, Spain
9 Altos Labs, Cambridge, UK
10 Centre de Recherche des Cordeliers, Equipe labellise´ e par la Ligue contre le cancer, Universite´ de Paris, Sorbonne Universite´ , INSERM U1138, Institut Universitaire de France, Paris, France
11 Metabolomics and Cell Biology Platforms, Gustave Roussy, Villejuif, France
12 Institut du Cancer Paris CARPEM, Department of Biology, Hoˆ pital Europe´ en Georges Pompidou, AP-HP, Paris, France
*Correspondence: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。 (C.L.-O.), 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。 (G.K.)
https://doi.org/10.1016/j.cell.2022.11.001
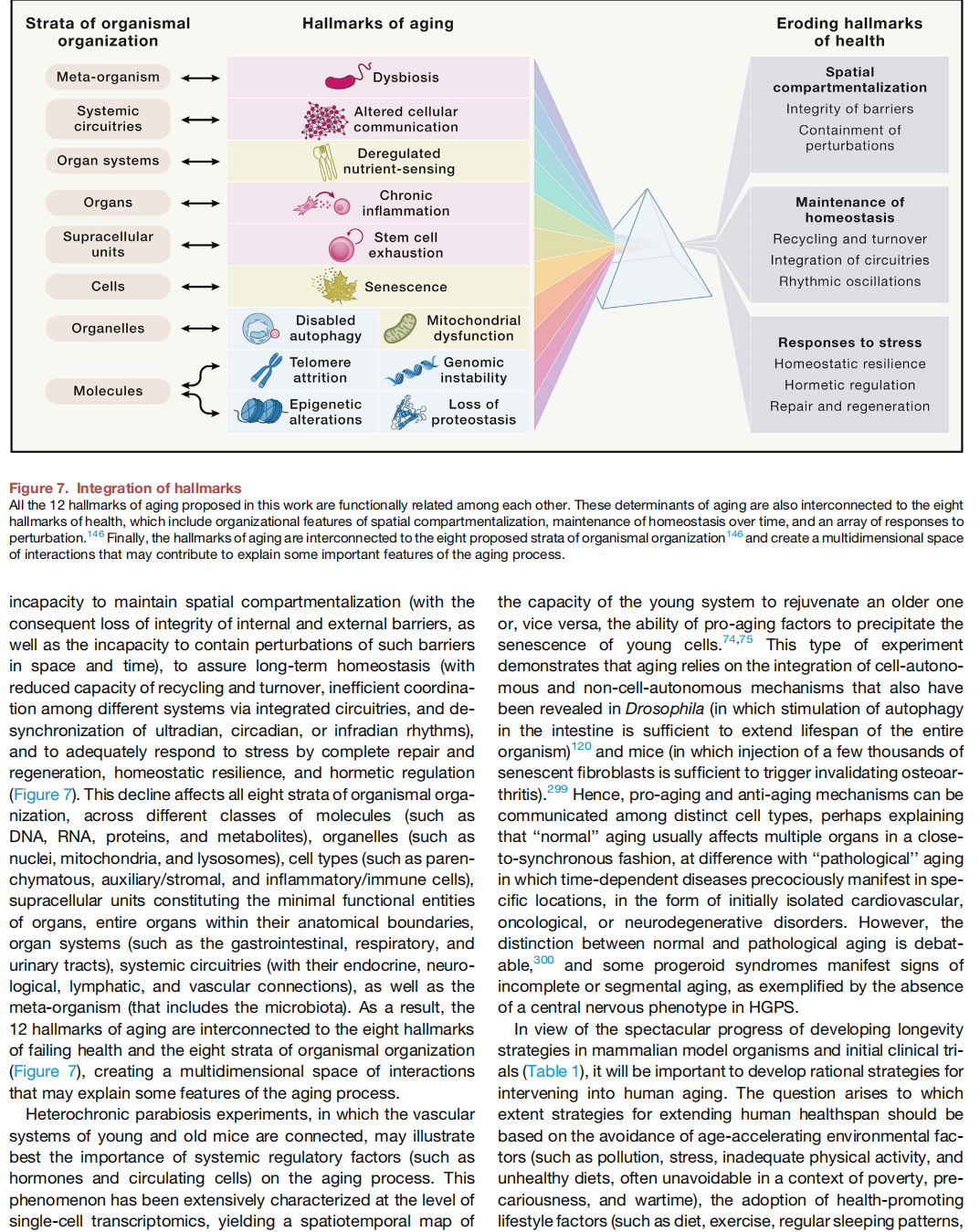
SUMMARY
Aging is driven by hallmarks fulfilling the following three premises: (1) their age-associated manifestation, (2) the acceleration of aging by experimentally accentuating them, and (3) the opportunity to decelerate, stop, or reverse aging by therapeutic interventions on them. We propose the following twelve hallmarks of aging: genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, disabled macroautophagy, deregulated nutrient-sensing, mitochondrial dysfunction, cellular senescence, stem cell exhaustion, altered intercellular communication, chronic inflammation, and dysbiosis. These hallmarks are interconnected among each other, as well as to the recently proposed hallmarks of health, which include organizational features of spatial compartmentalization, maintenance of homeostasis, and adequate responses to strees.
