
伤口世界
电子邮件地址: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。
- 星期三, 29 10月 2025
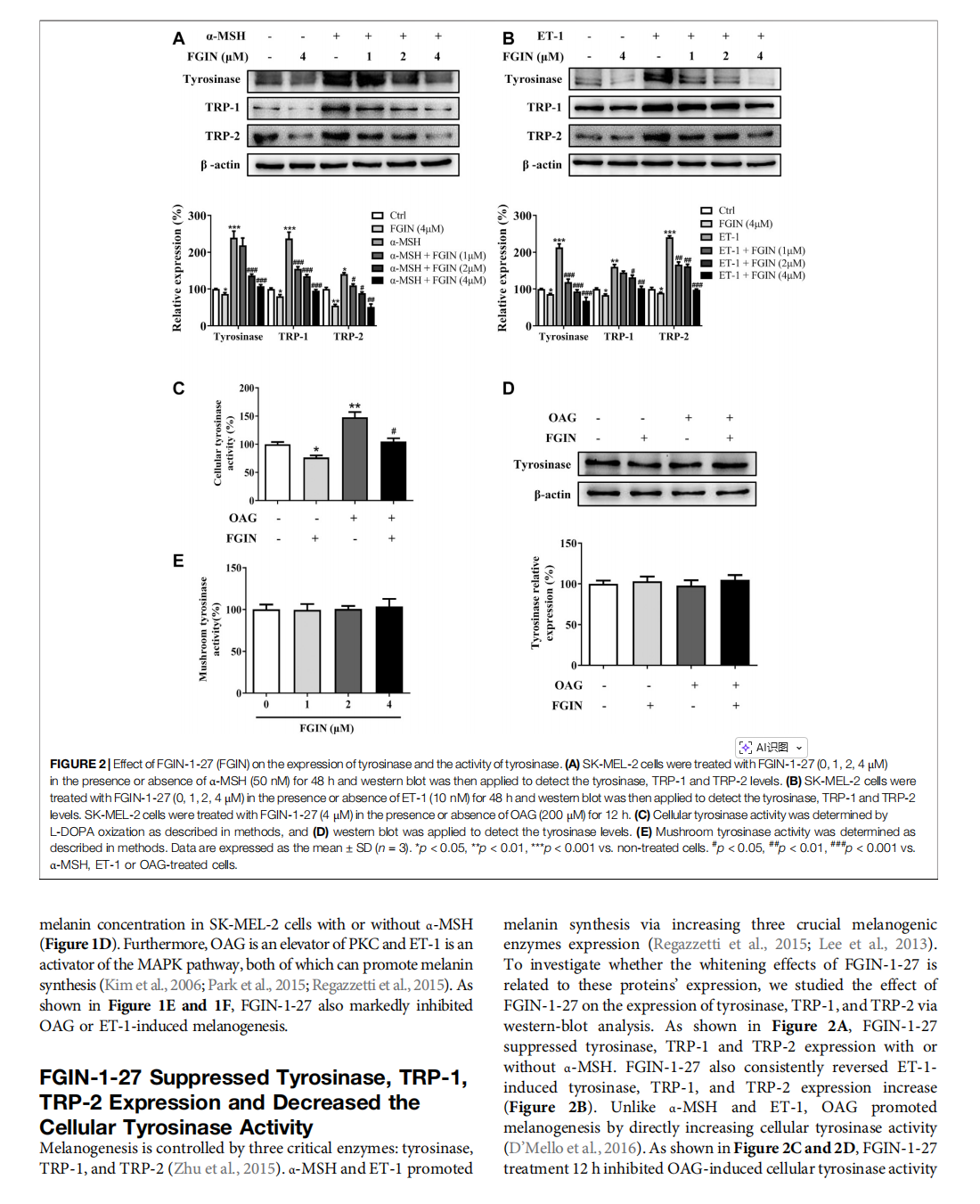
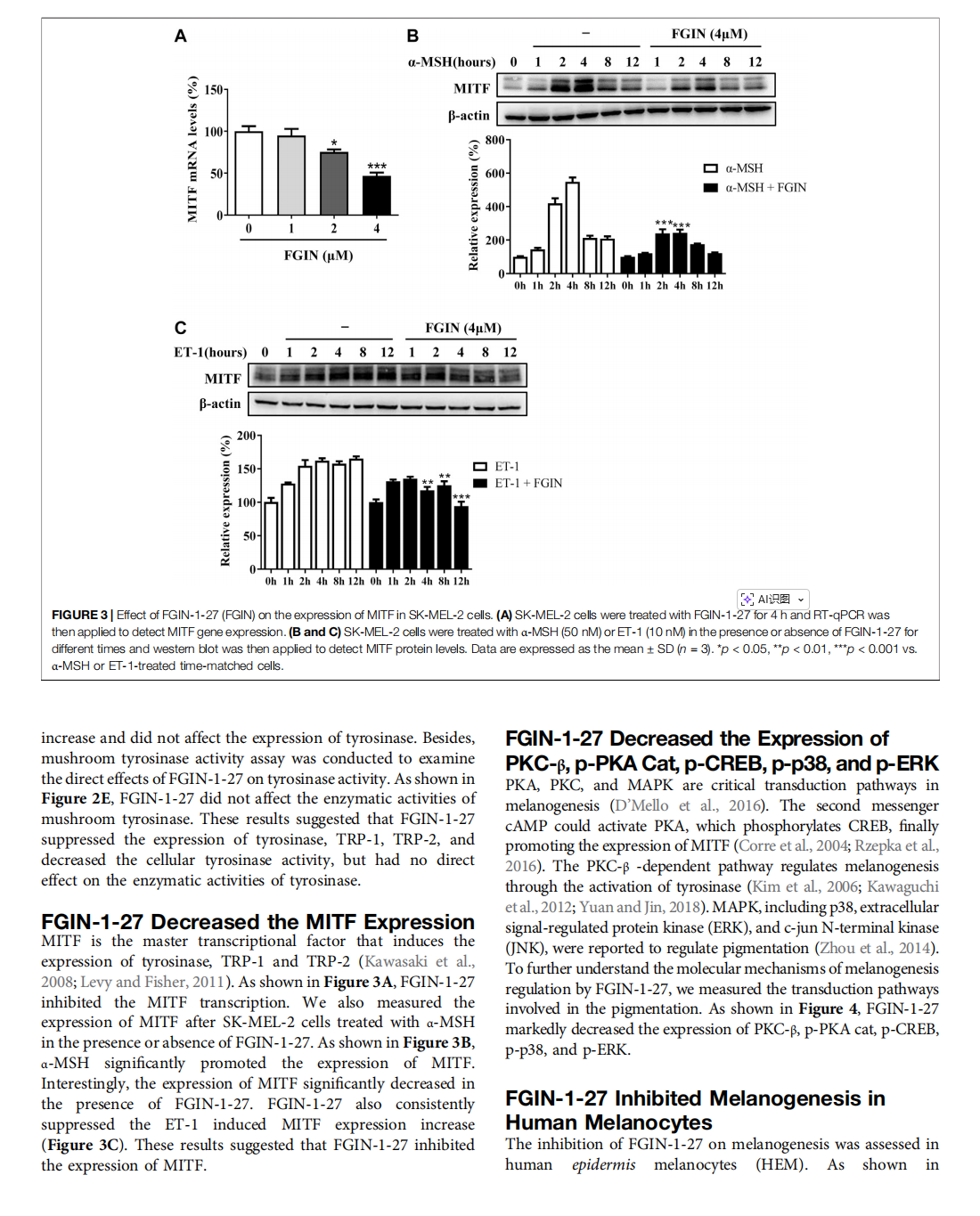
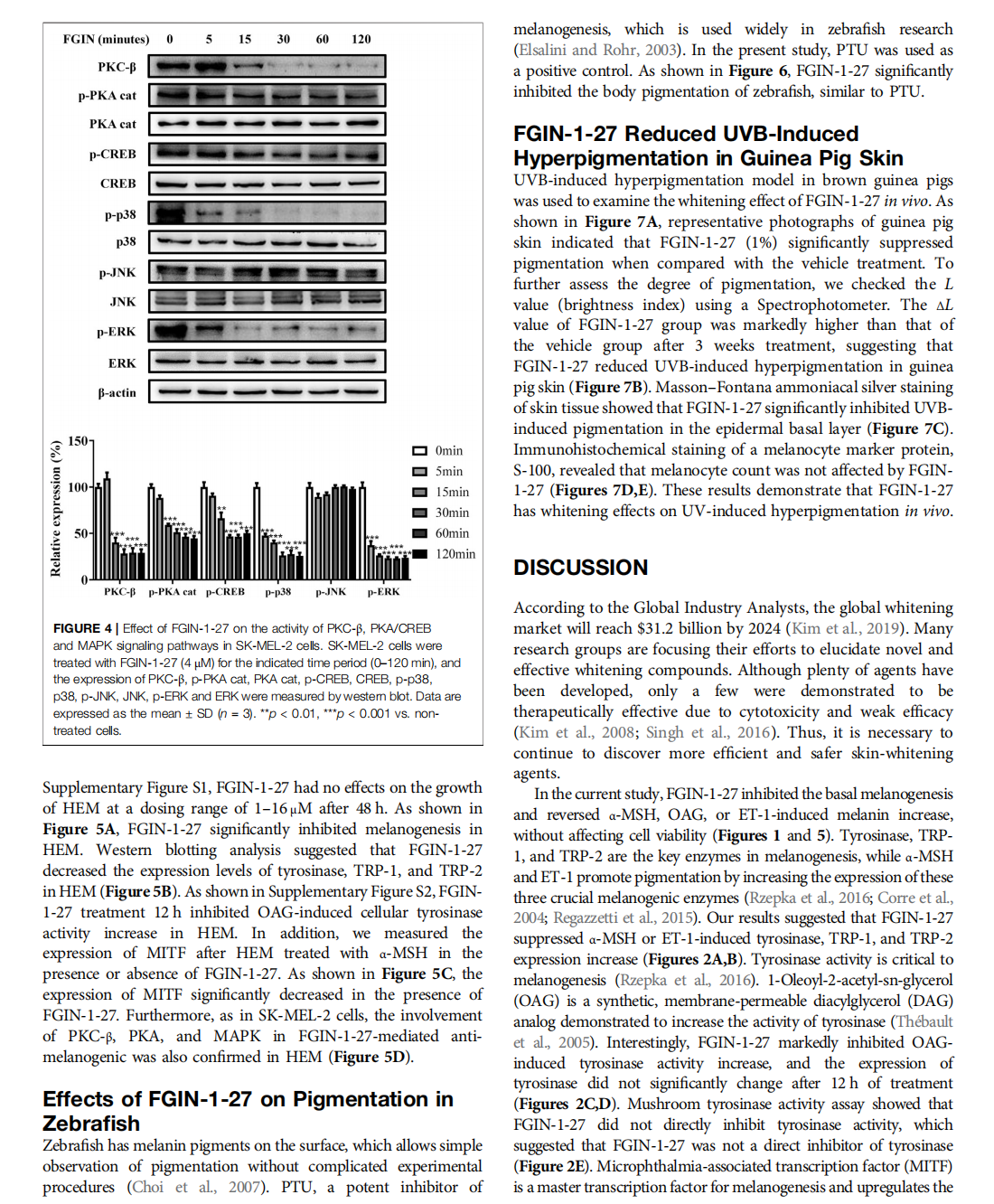
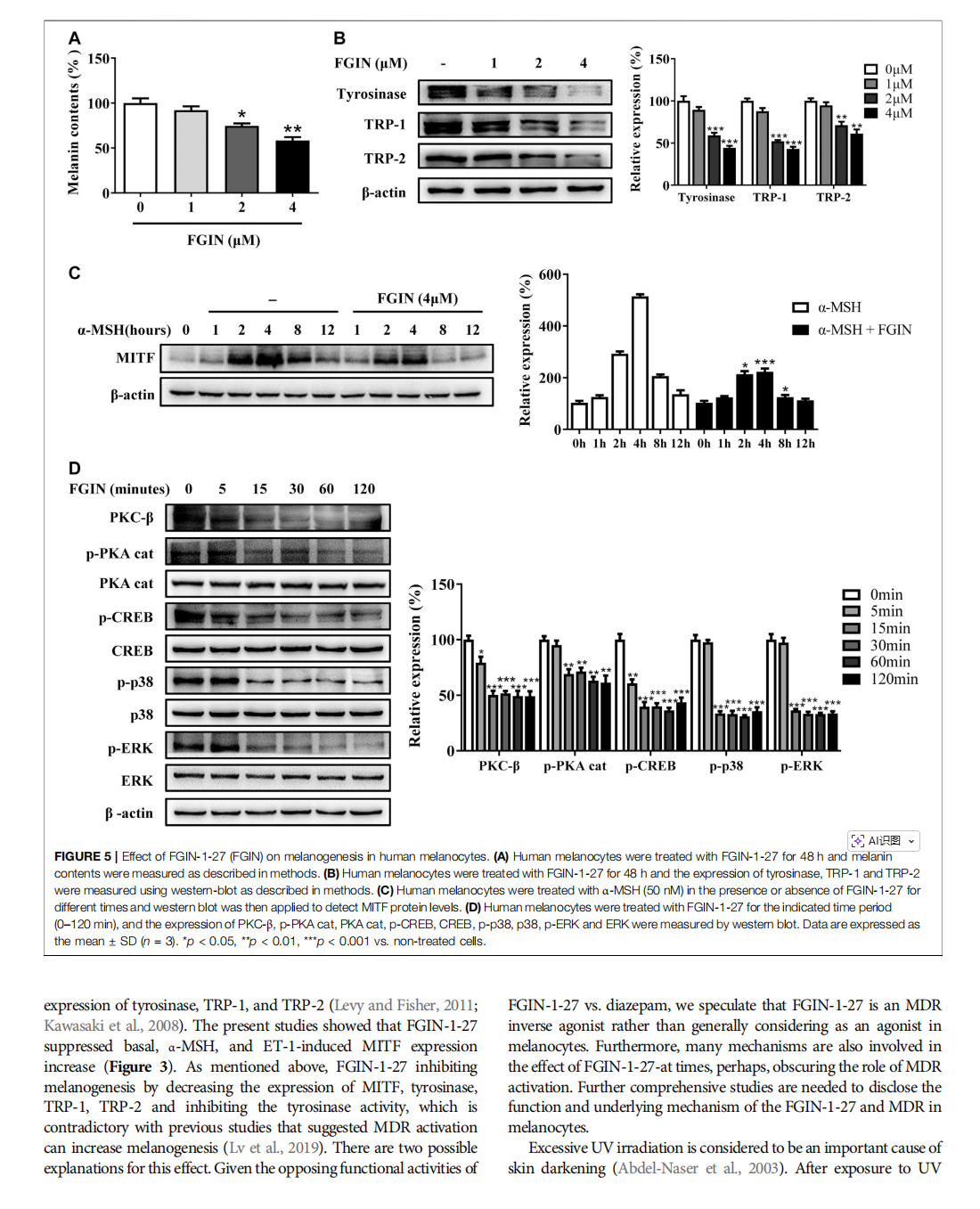
FGIN-1-27 Inhibits Melanogenesis by Regulating Protein Kinase A/cAMP-Responsive Element-Binding, Protein Kinase C-β, and Mitogen-Activated Protein Kinase Pathways

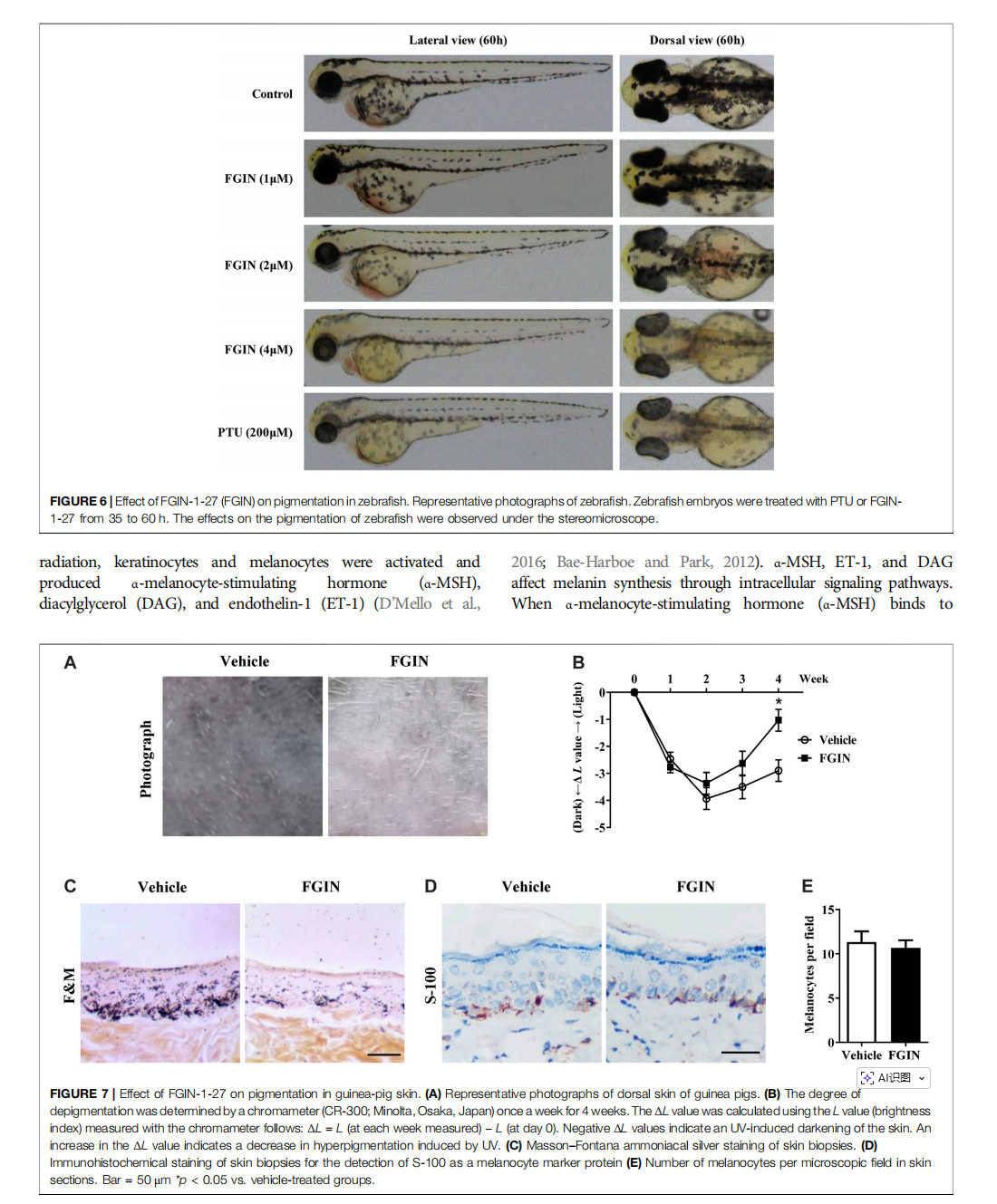
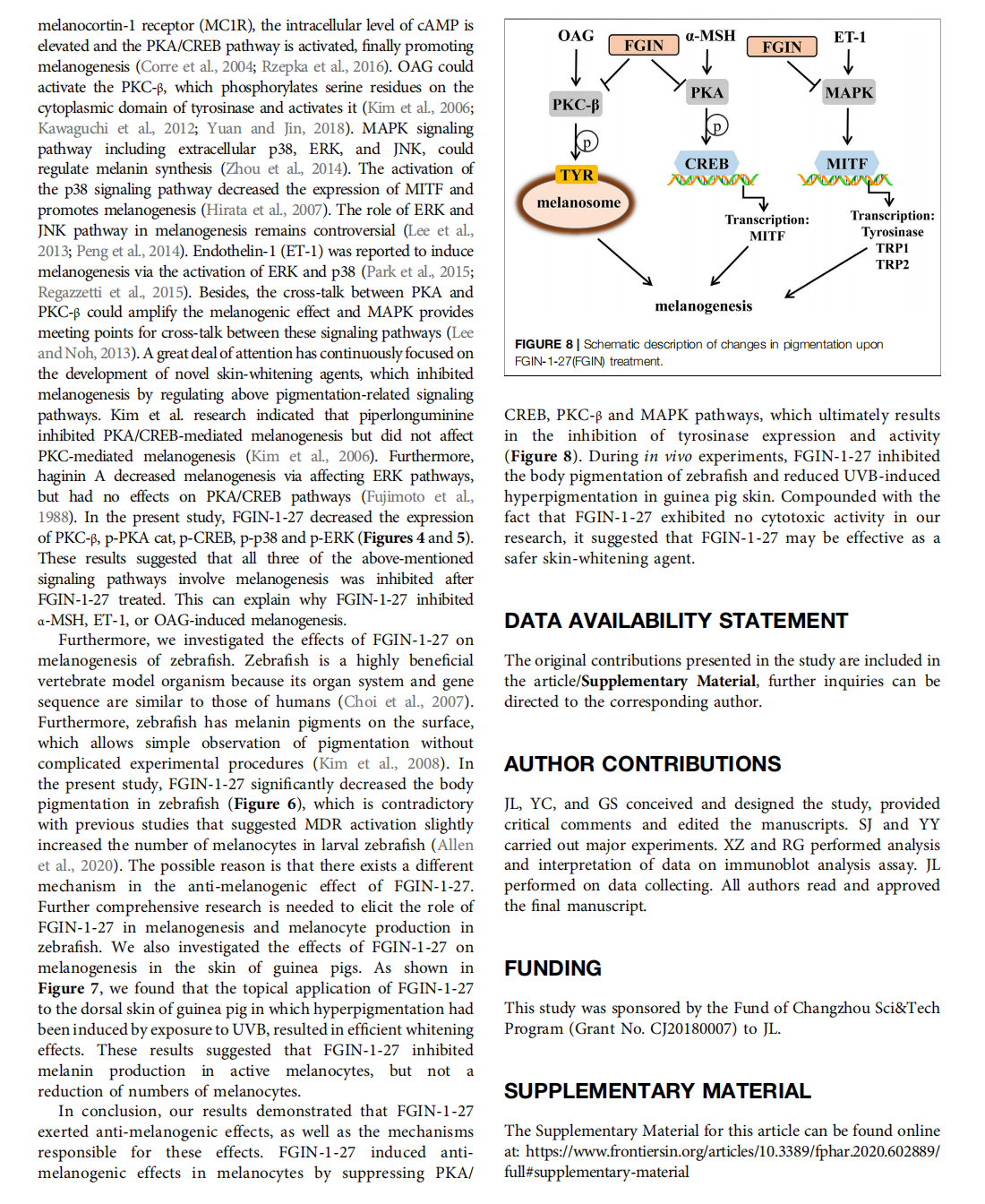

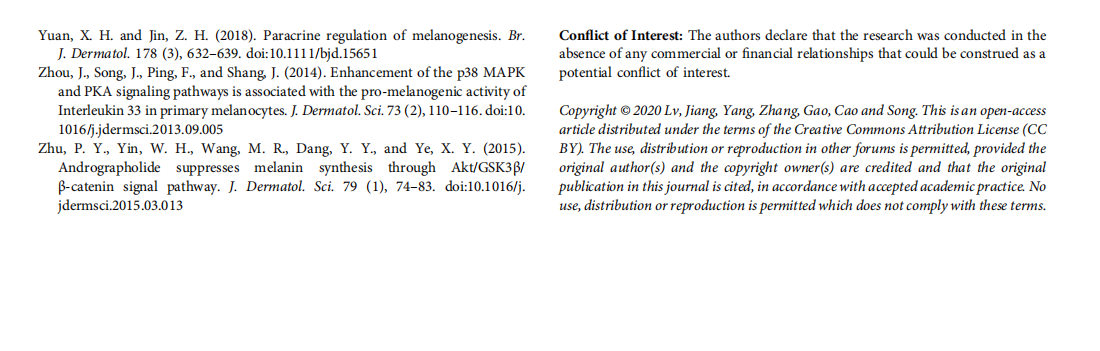
This article is excerpted from the 《Frontiers in Pharmacology》 by Wound World

- 星期二, 28 10月 2025
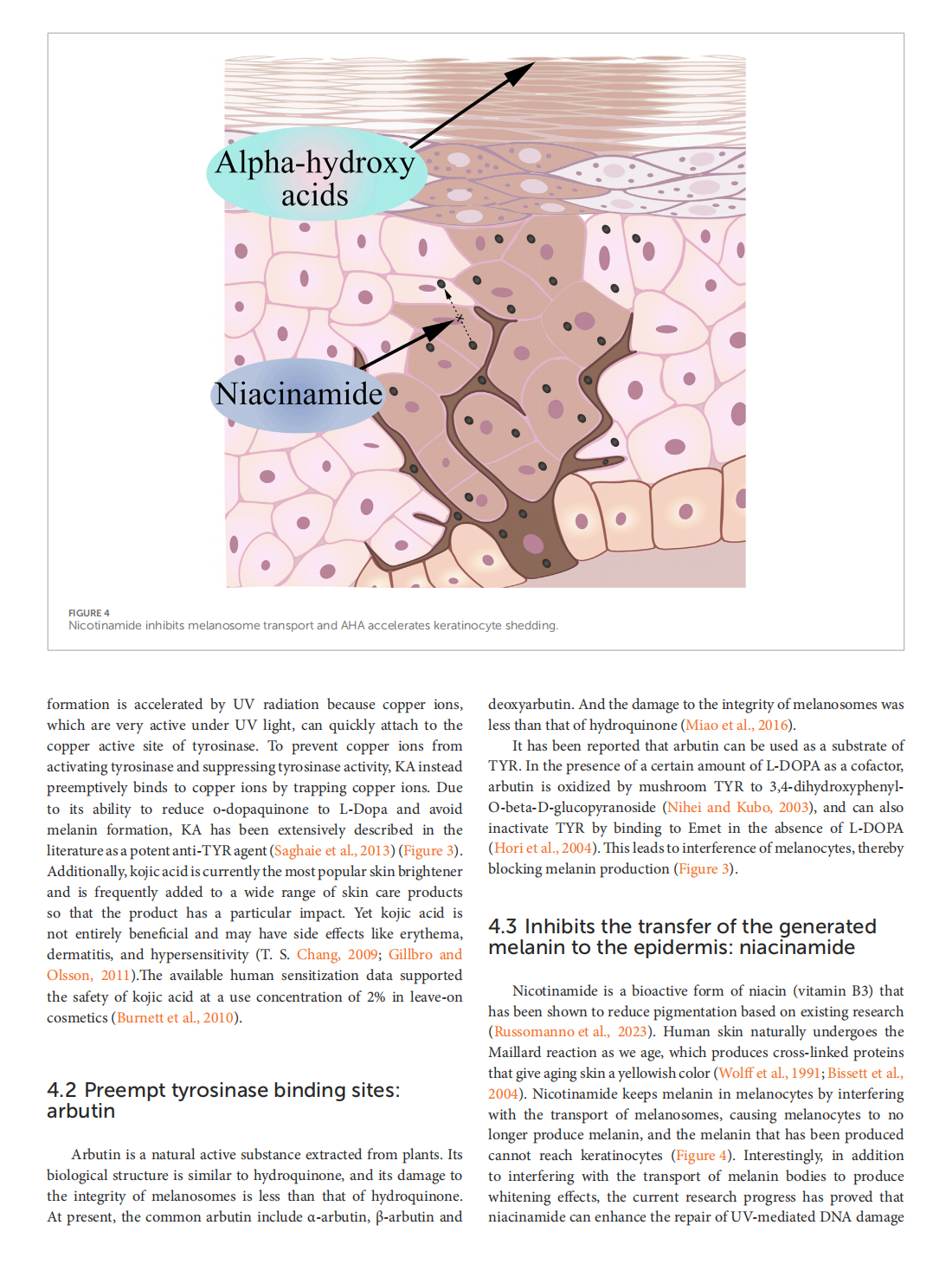
The biochemistry of melanogenesis: an insight into the function and mechanism of melanogenesis-related proteins






This article is excerpted from the 《Frontiers in Molecular Biosciences》 by Wound World

- 星期一, 27 10月 2025
The Whitening, Moisturizing, Anti-aging Activities, and Skincare Evaluation of Selenium-Enriched Mung Bean Fermentation Broth




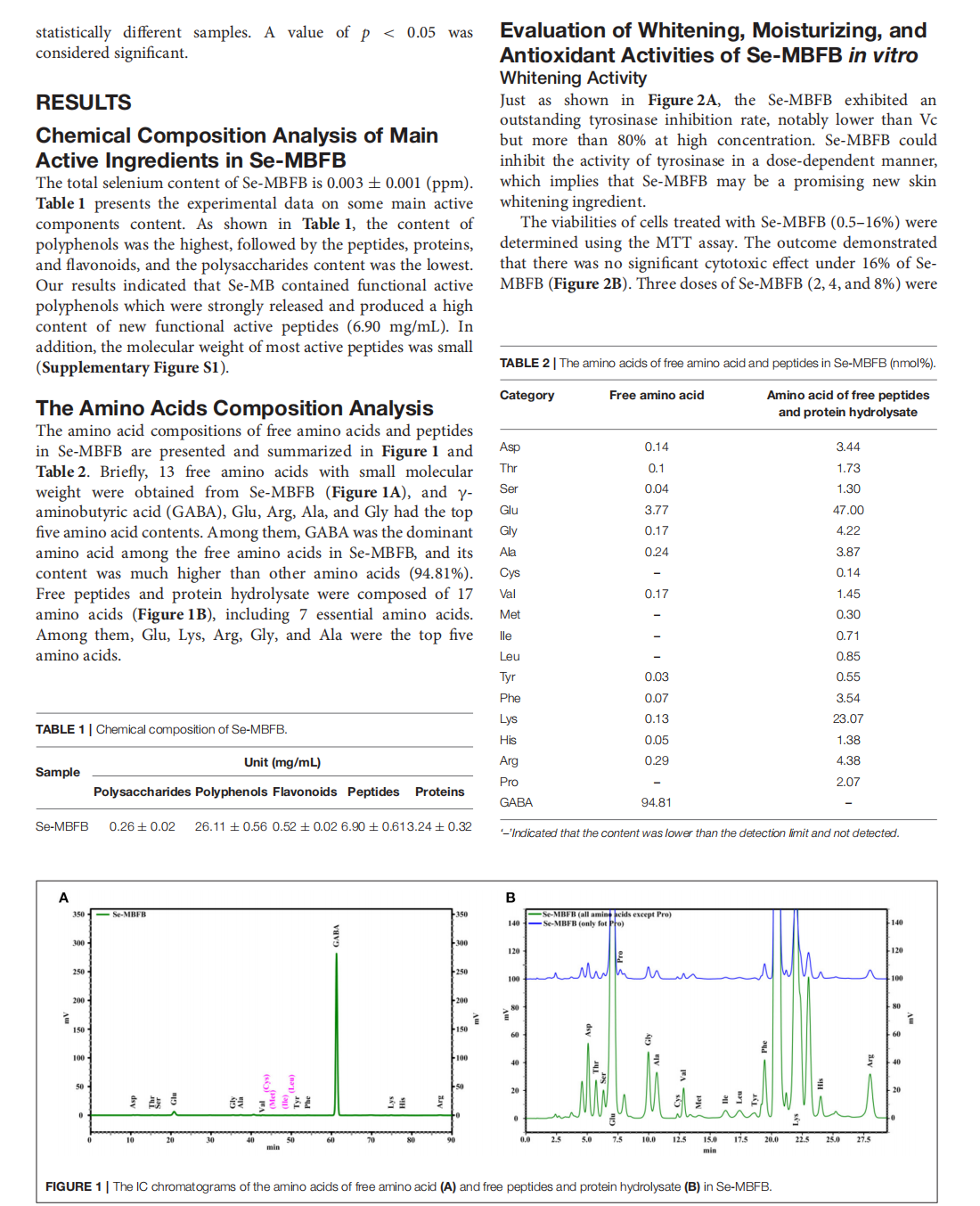
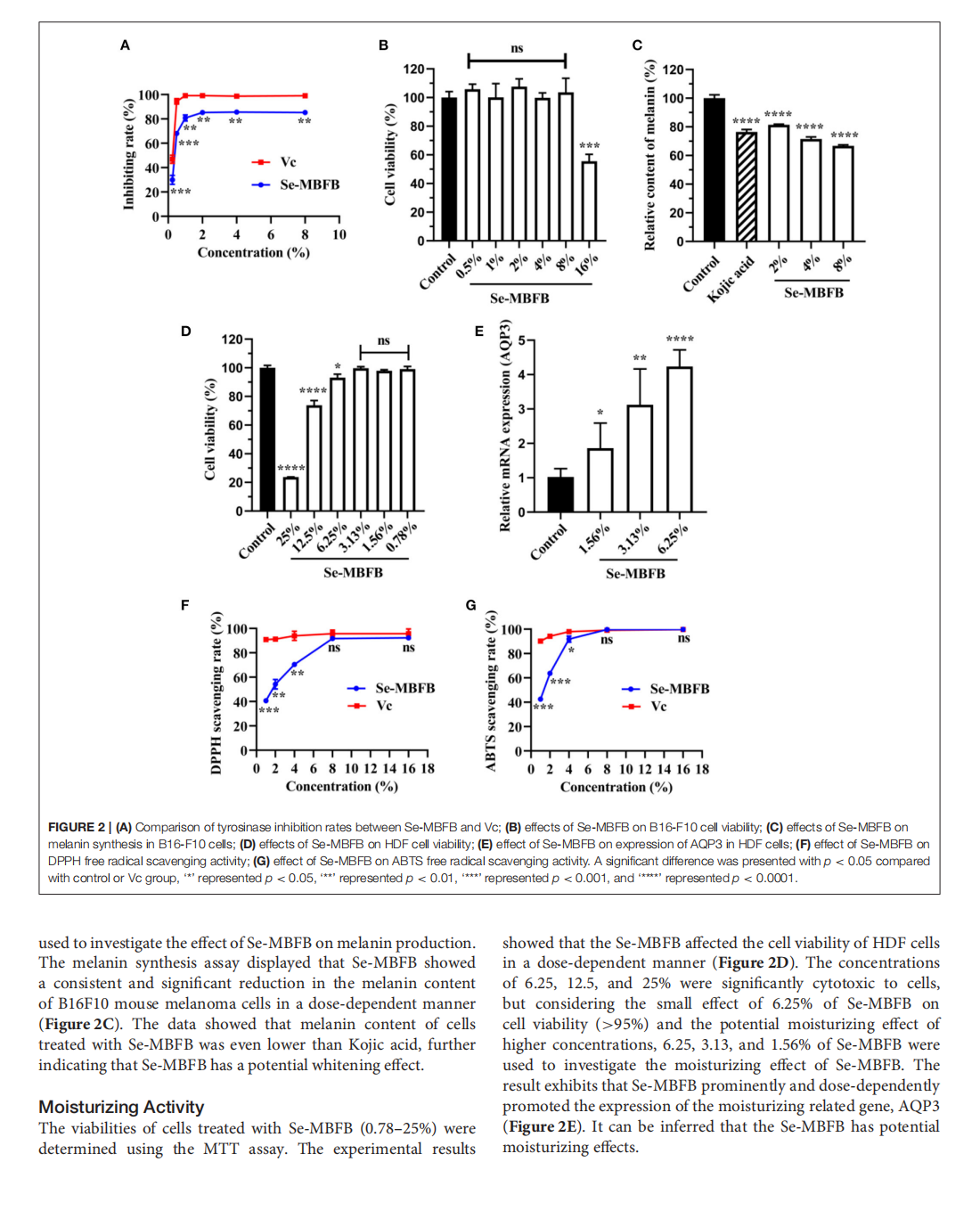

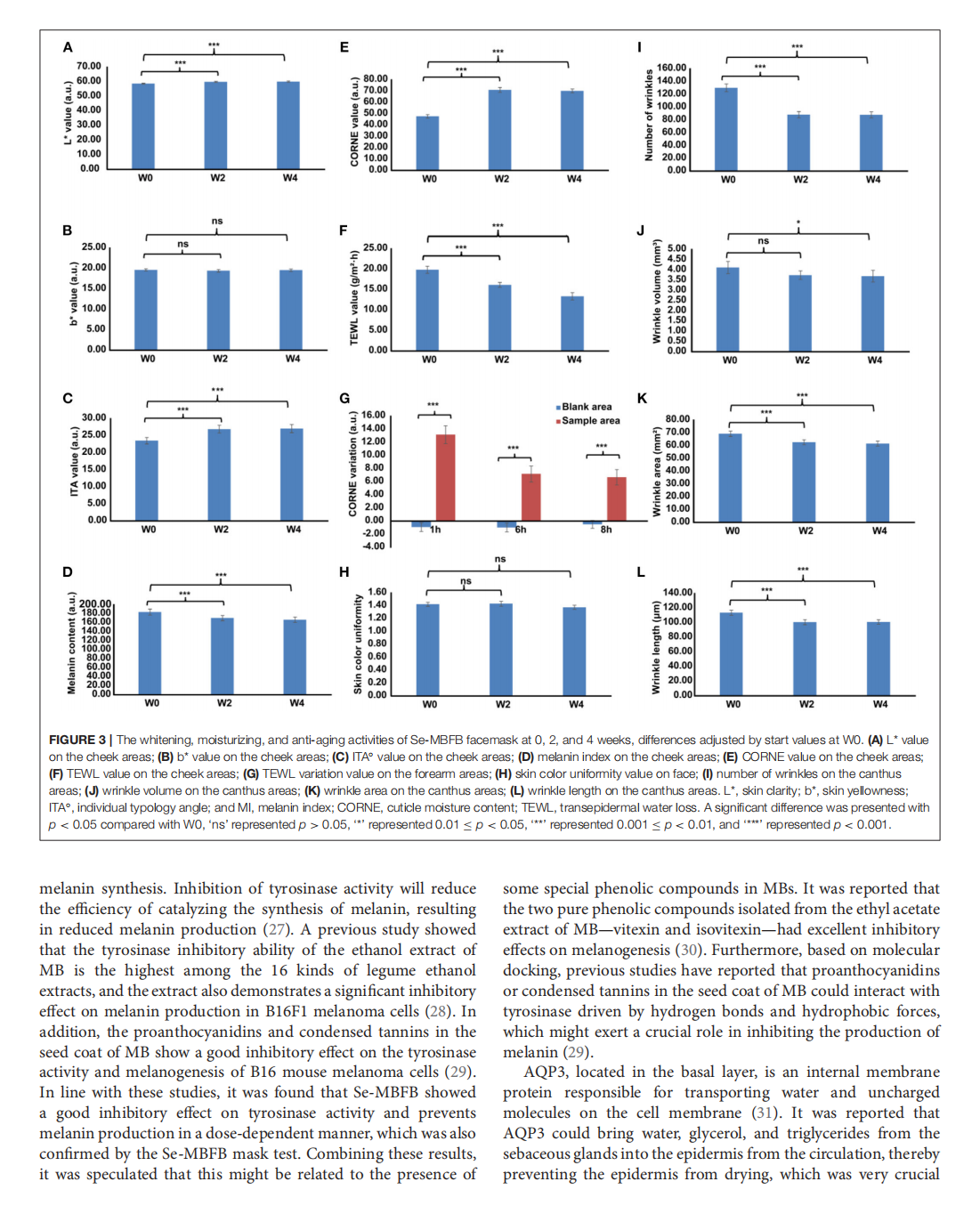
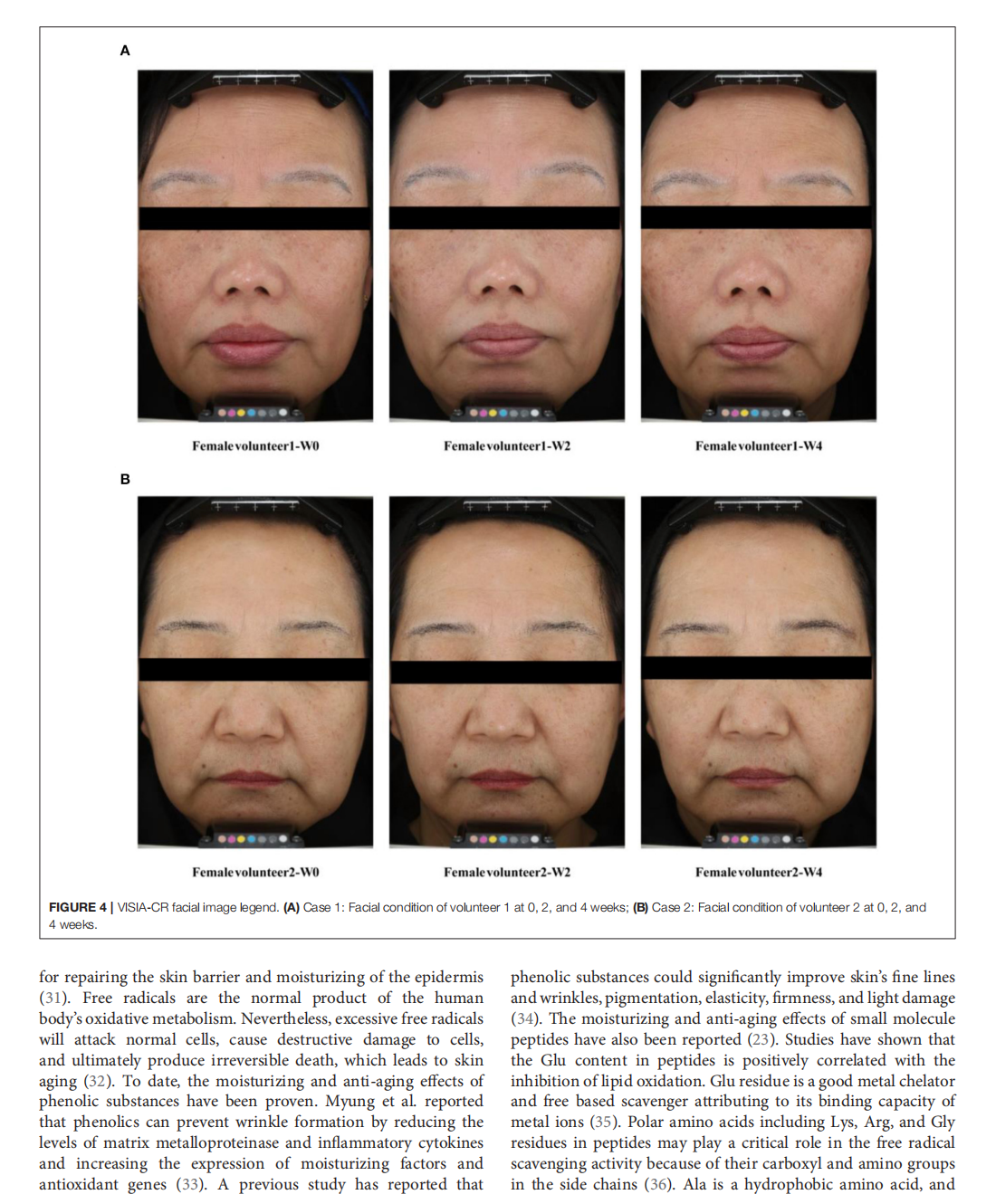
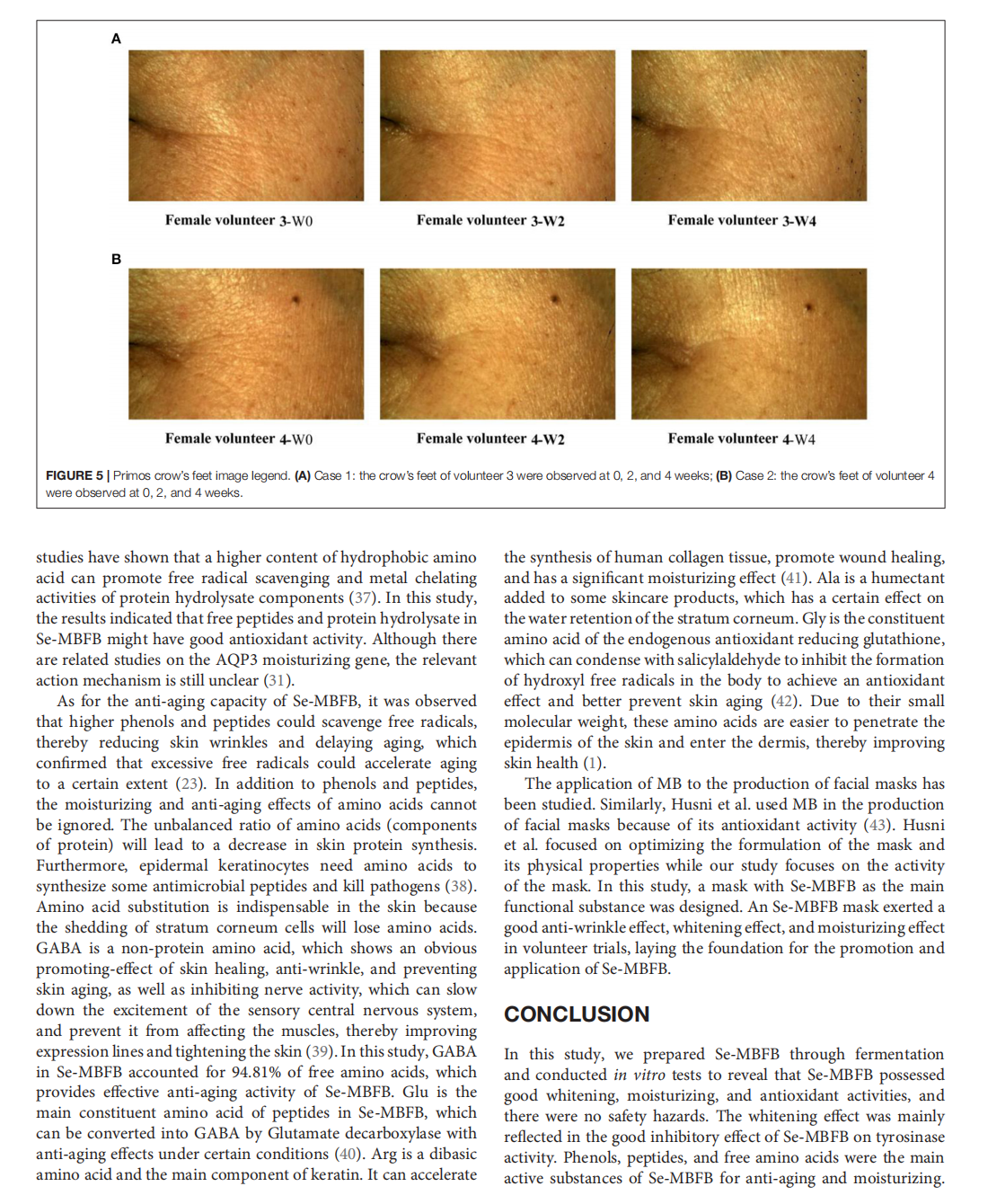
This article is excerpted from the《Frontiers in Nutrition》 by Wound World

- 星期五, 24 10月 2025
Chinese Consumers’ Herd Consumption Behavior Related to Korean Luxury Cosmetics: The Mediating Role of Fear of Missing Out

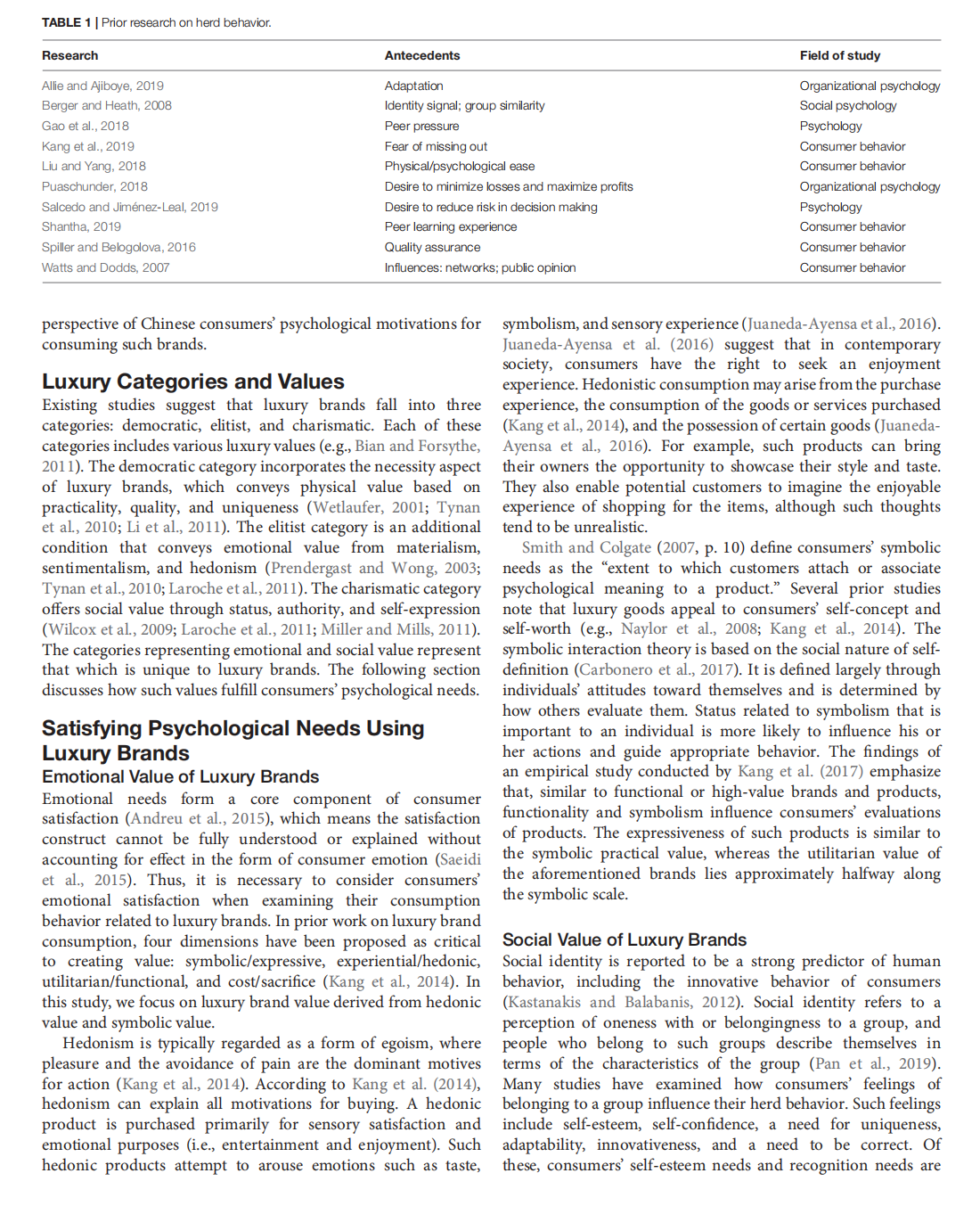


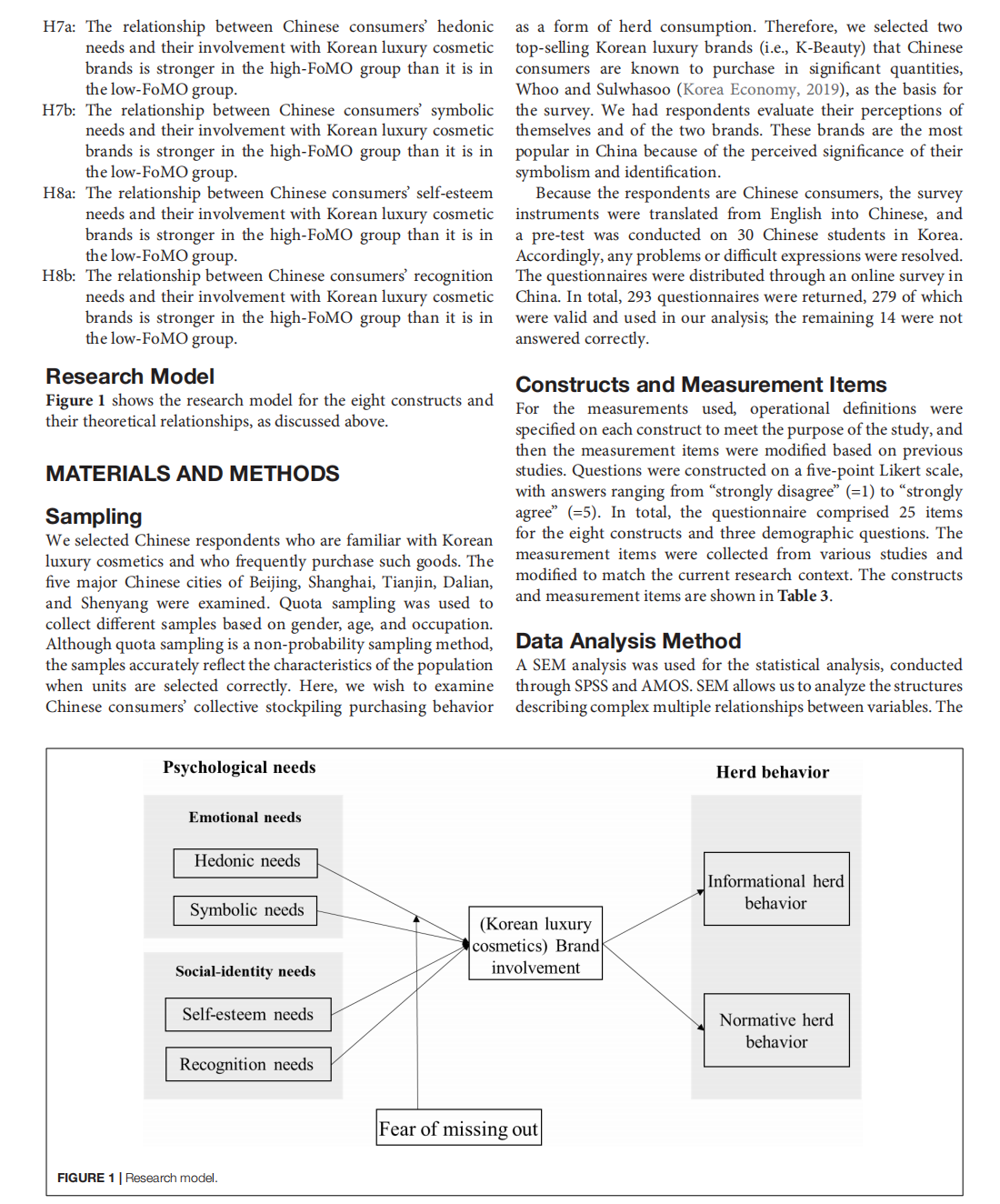
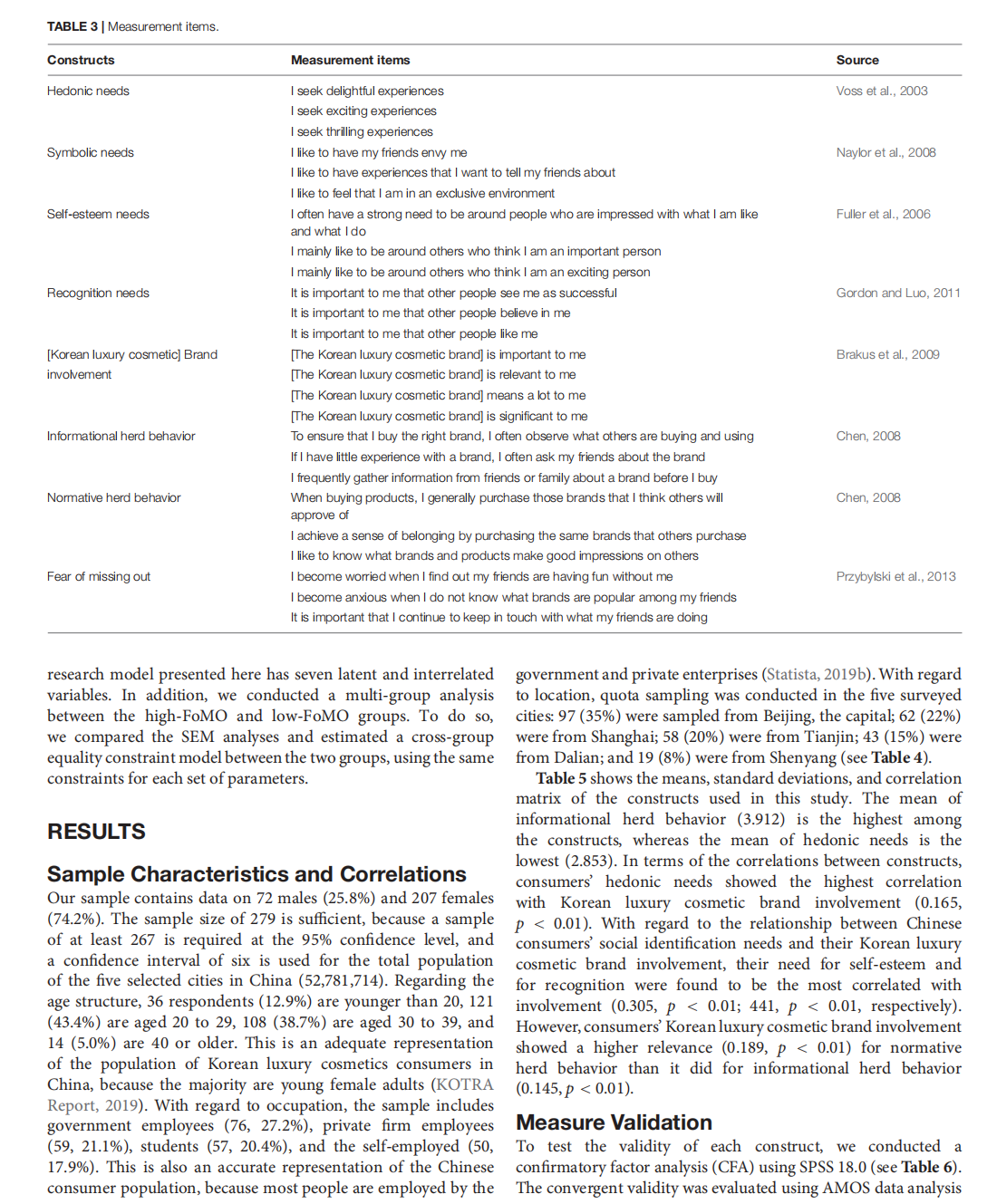
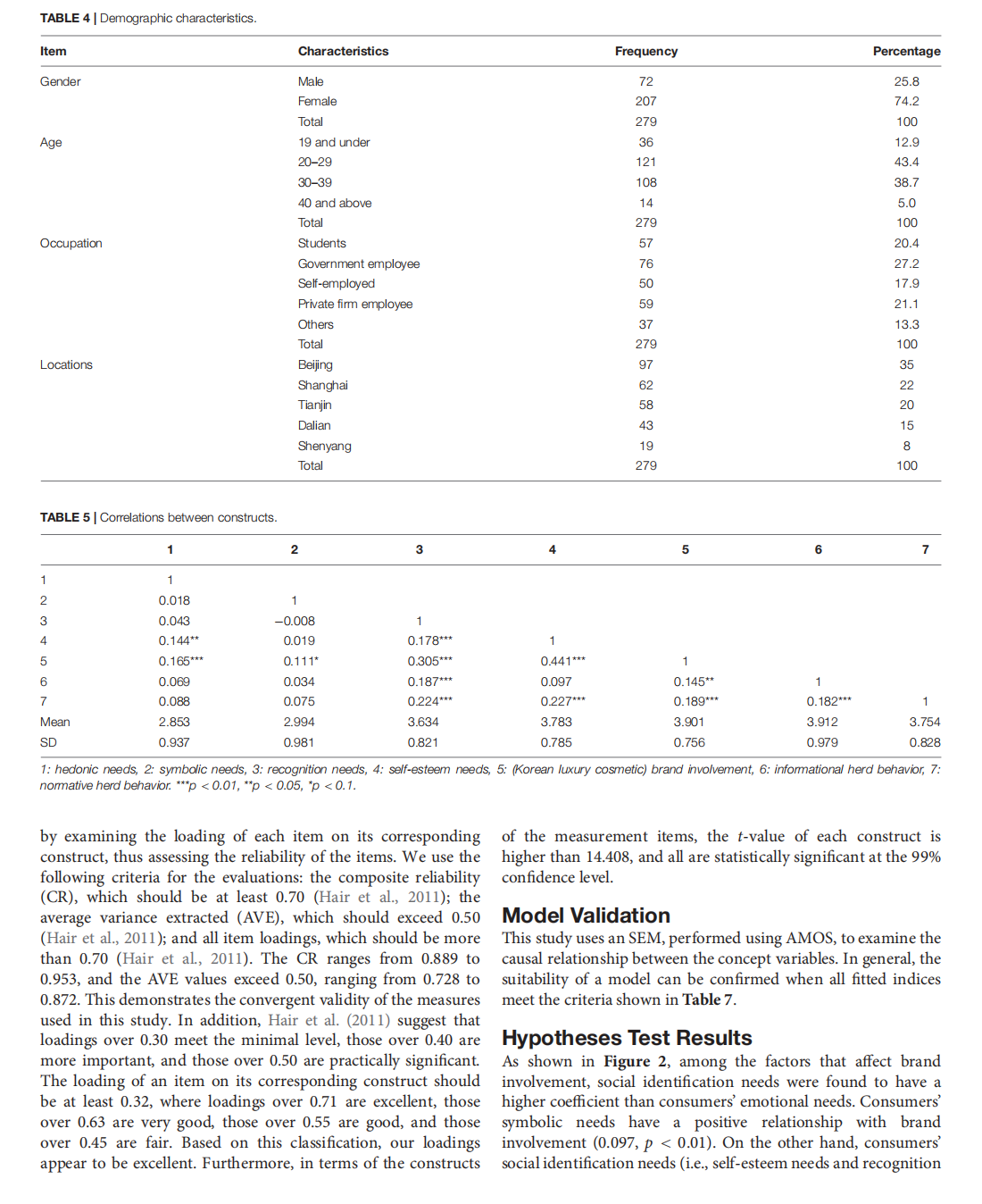
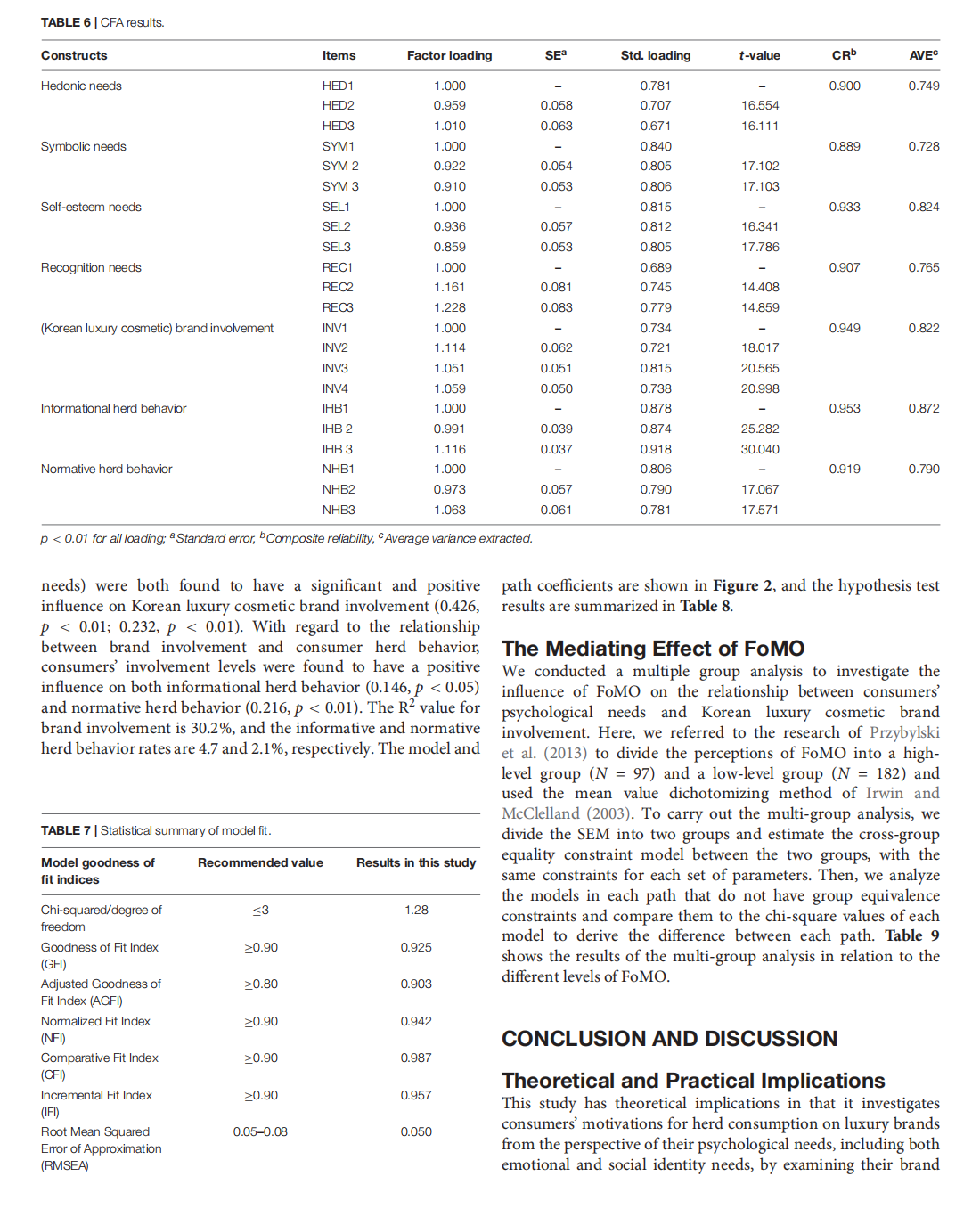
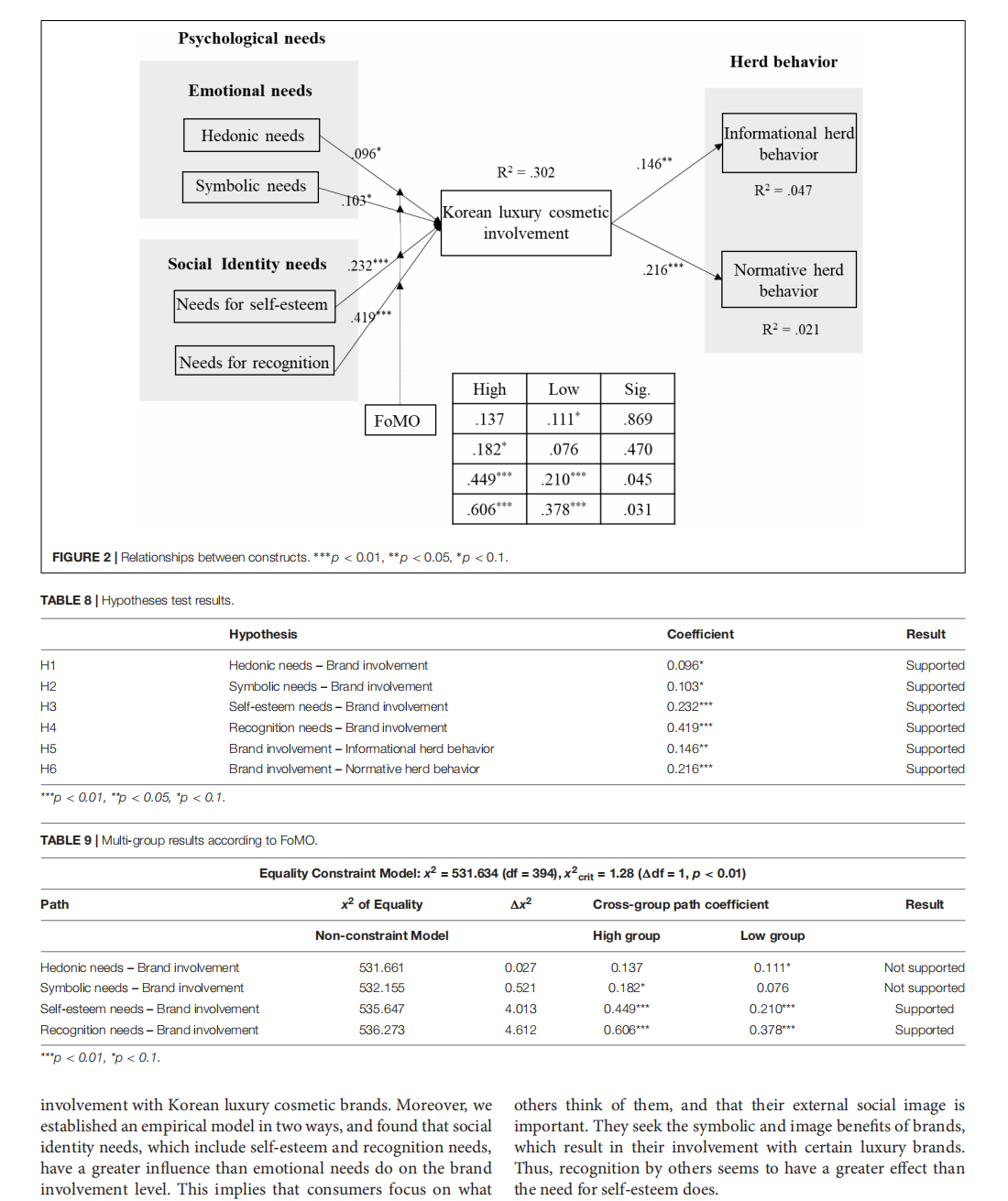


This article is excerpted from the 《Frontiers in Psychology》 by Wound World
- 星期四, 23 10月 2025
Safety Profile of Caesalpinia spinosa Aqueous Extract Tested in Oreochromis niloticus Toward Its Application in Dermocosmetics

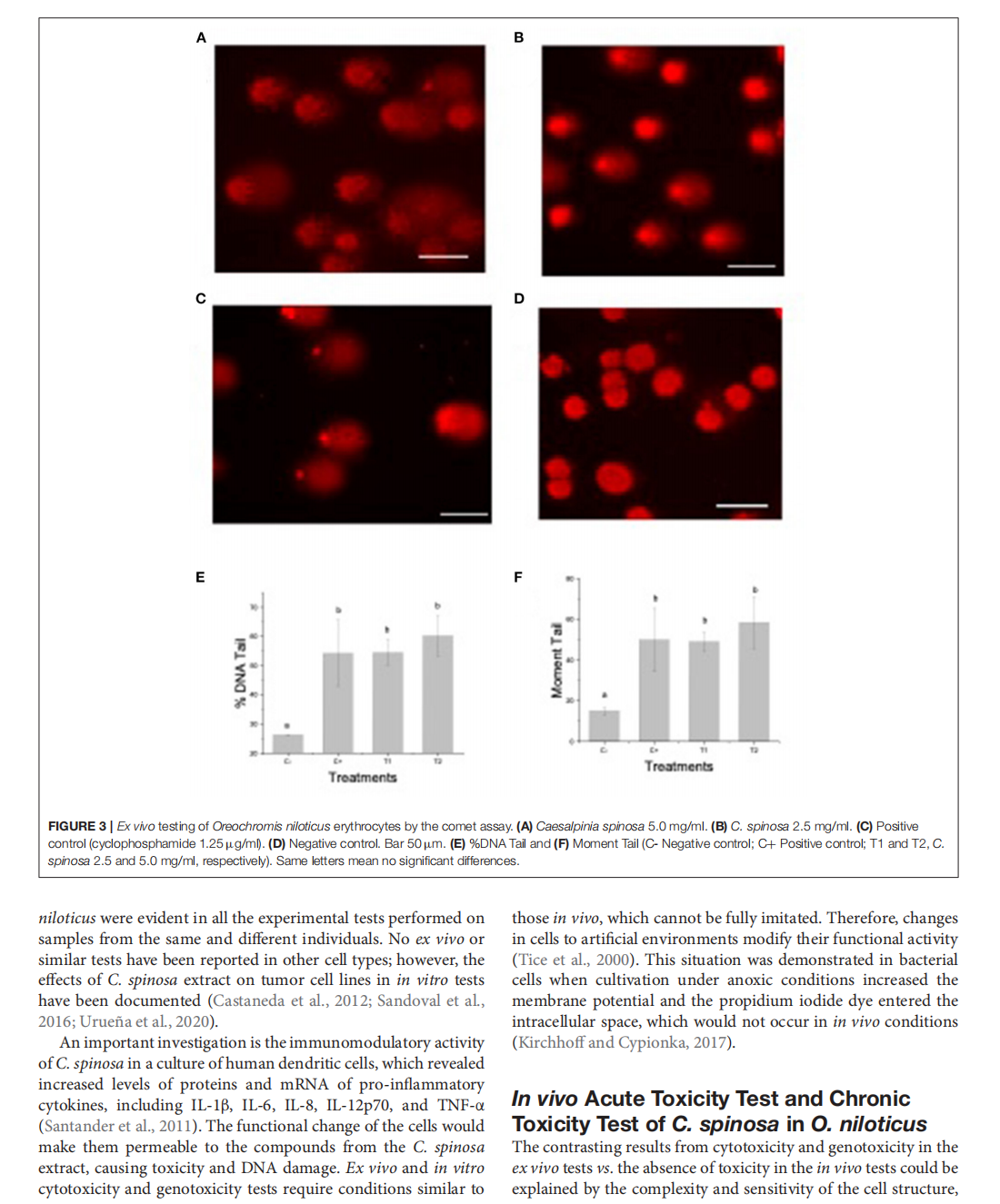
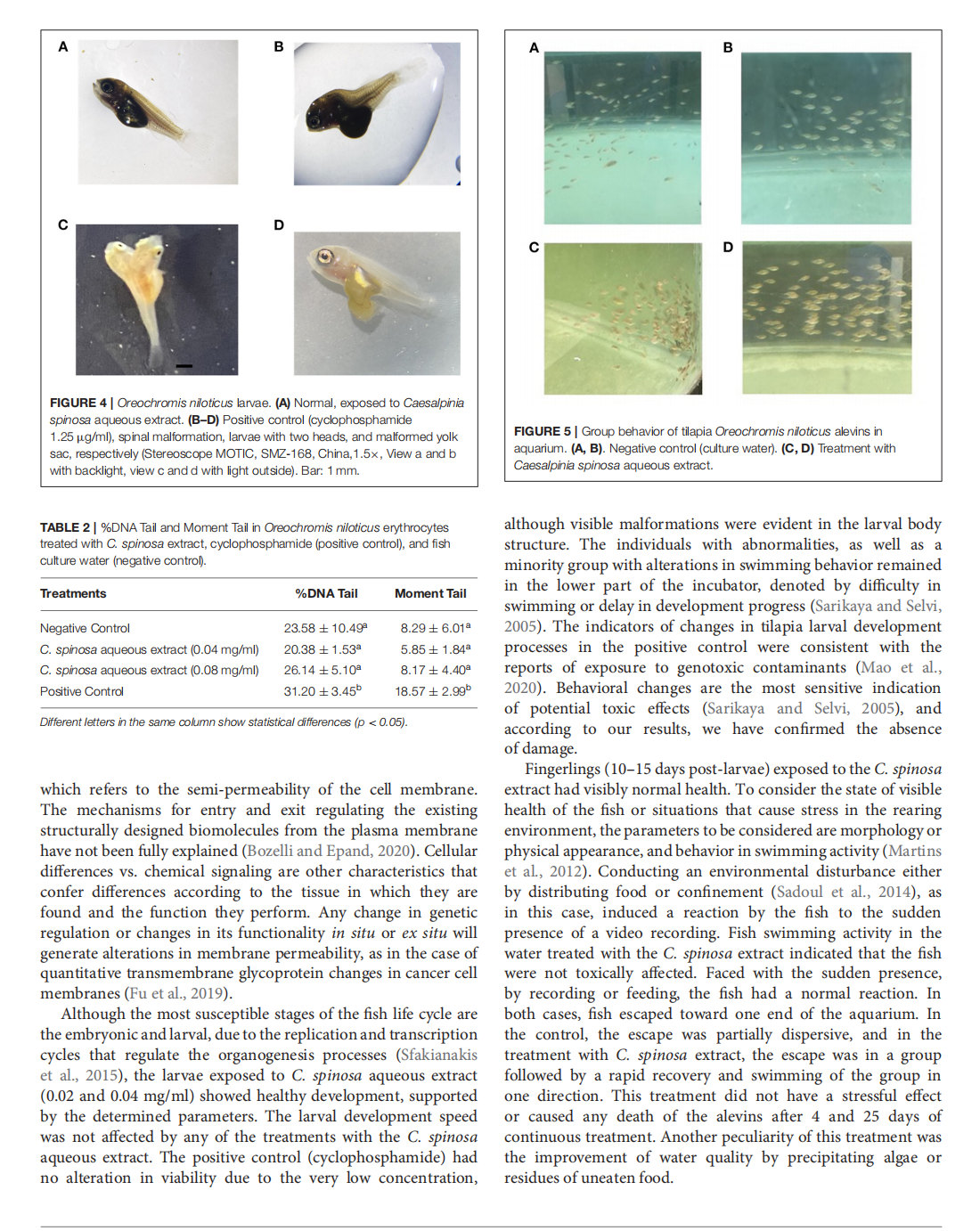
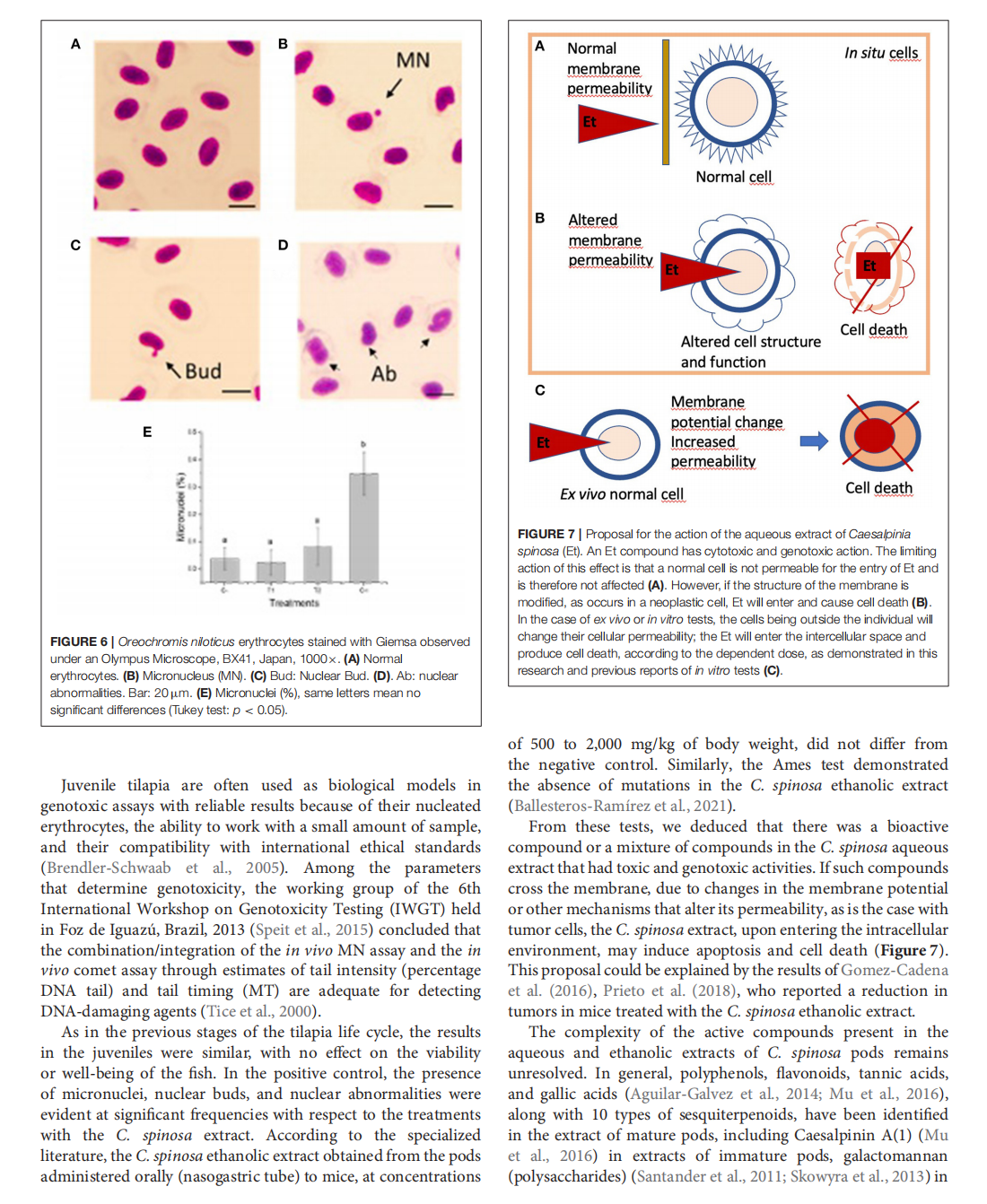


This article is excerpted from the 《Frontiers in Sustainability》by Wound World

- 星期三, 22 10月 2025
Prediction of Skin Sensitization Potential of Silver and Zinc Oxide Nanoparticles Through the Human Cell Line Activation Test


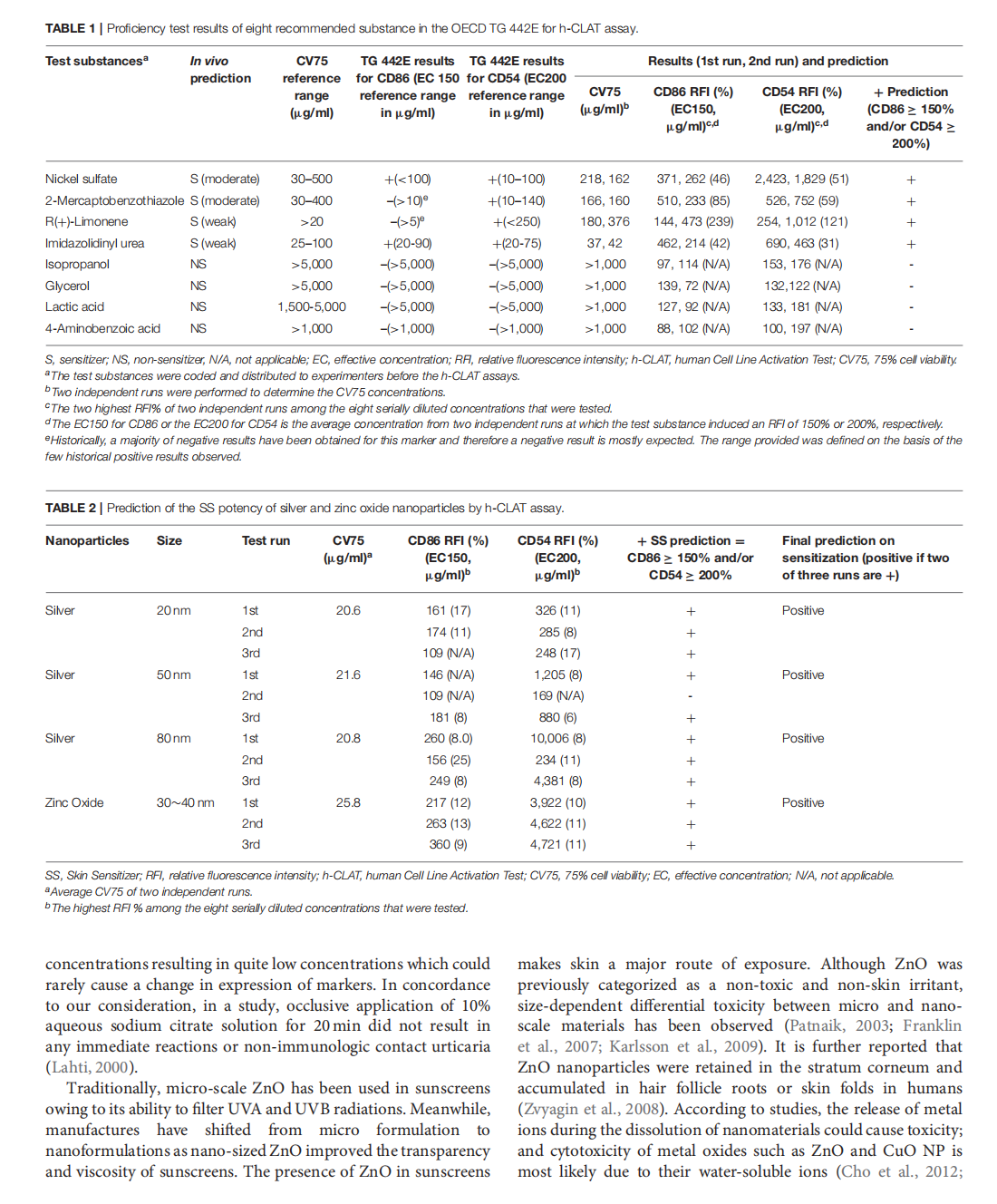
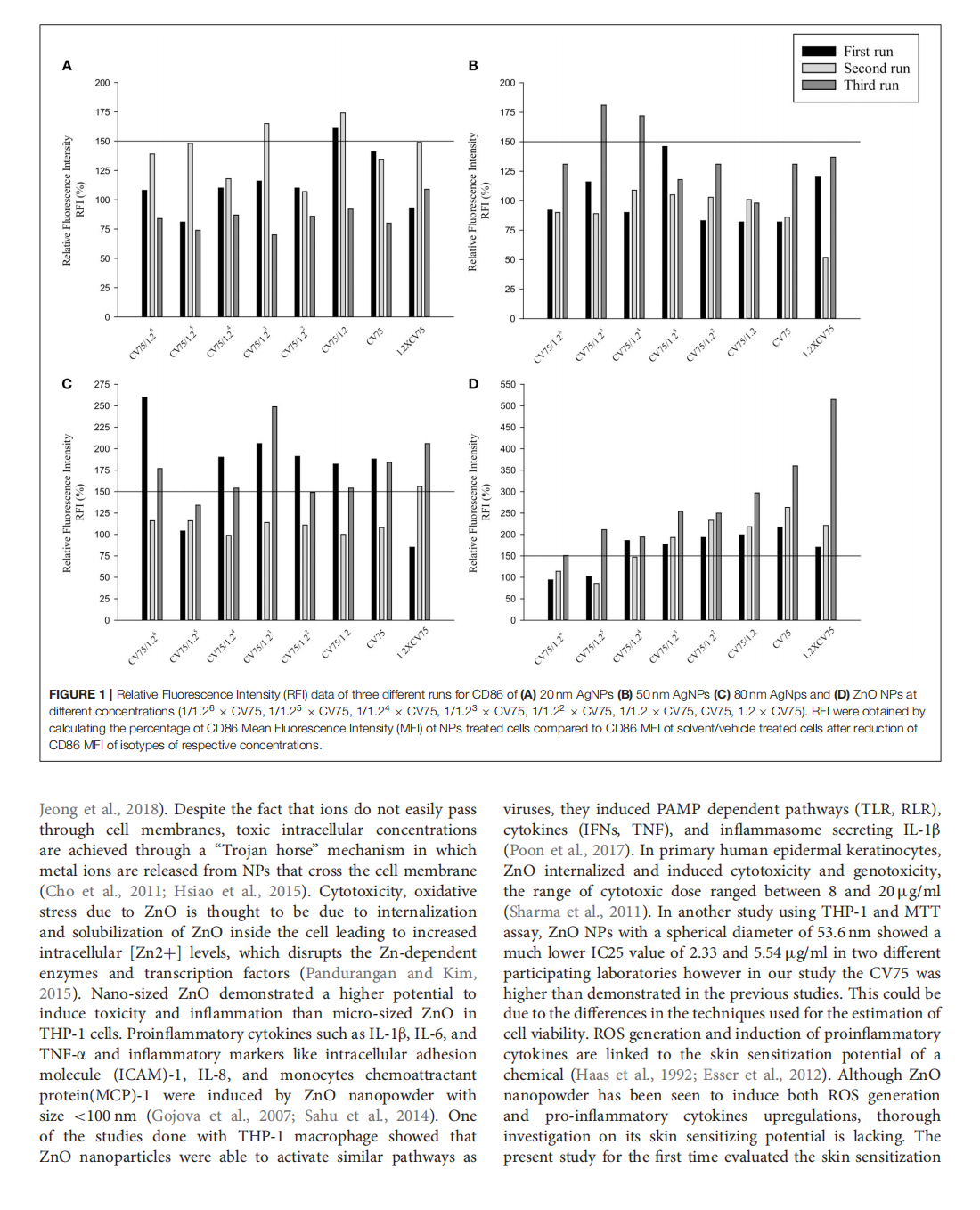
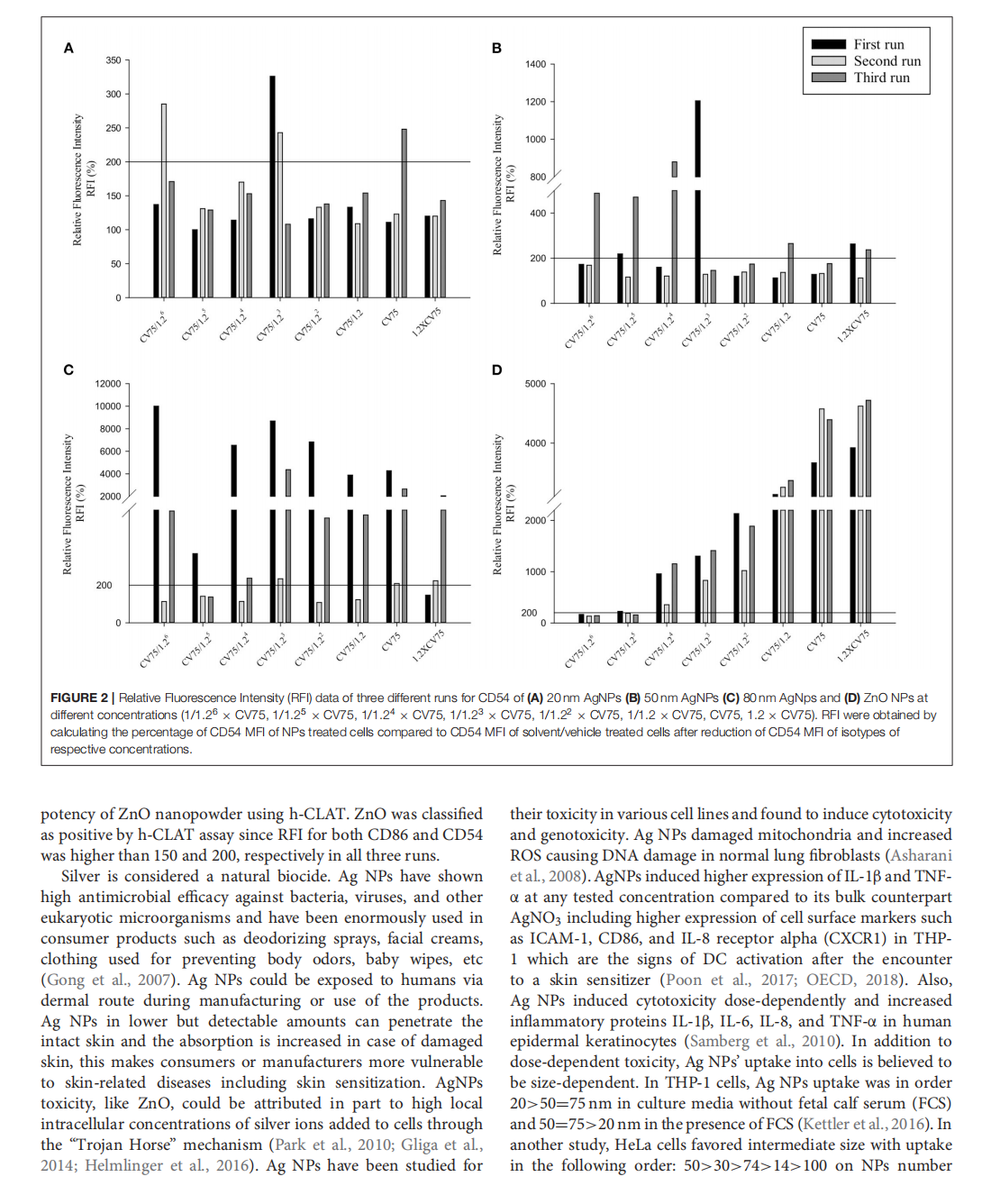



This article is excerpted from the 《Frontiers in Toxicology》 by Wound World

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}