
伤口世界
电子邮件地址: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。

- 星期一, 15 12月 2025
The role of anti-aging approaches in managing hypogonadism in sedentary older males



This article is excerpted from the 《Frontiers in Aging》 by Wound World

- 星期五, 12 12月 2025
Prediction of Subtle Cognitive Decline in Normal Aging: Added Value of Quantitative MRI and PET Imaging


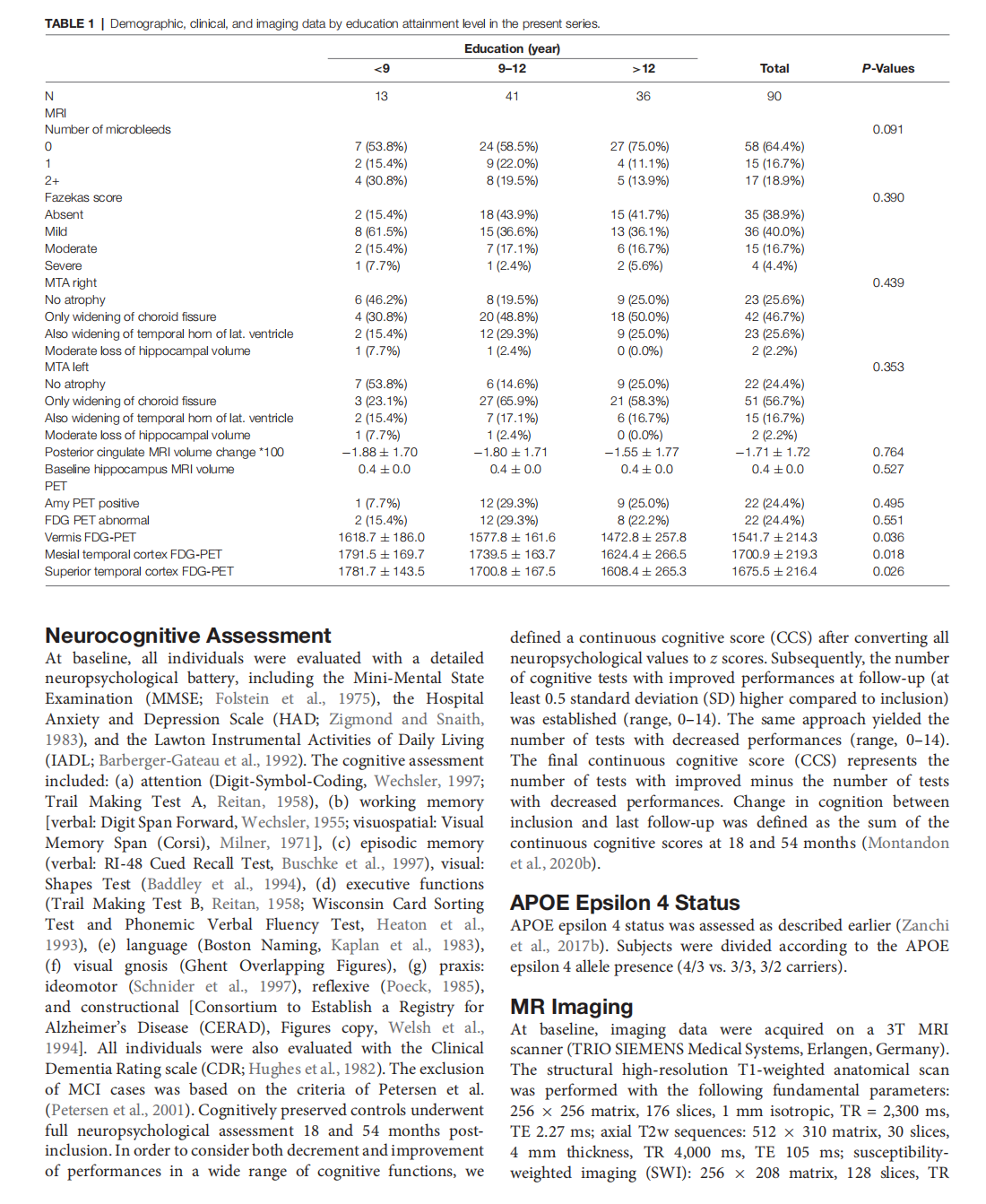




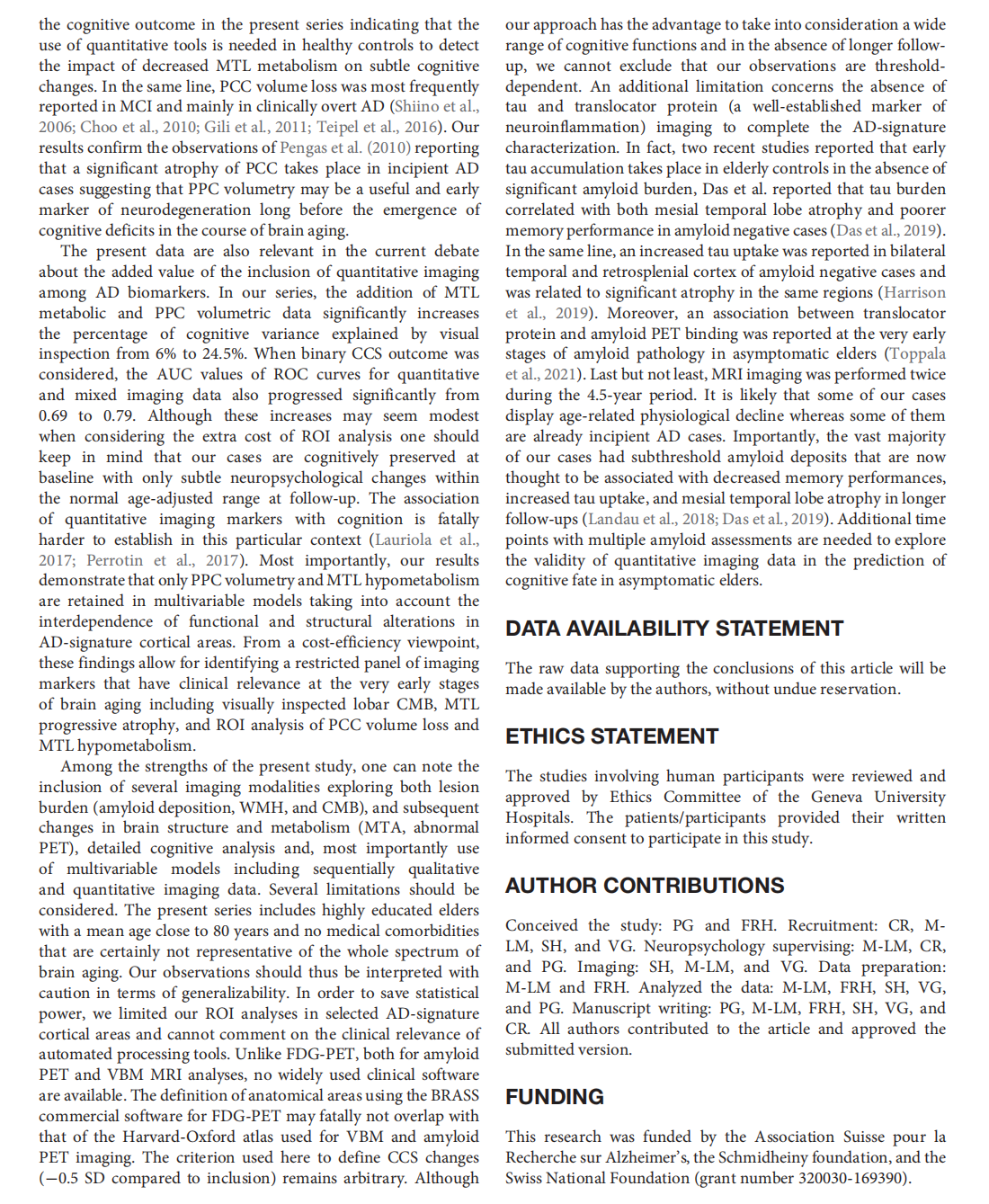


This article is excerpted from the 《Frontiers in Aging Neuroscience》 by Wound World
- 星期四, 11 12月 2025
Repeatability of Quantitative Imaging Features in Prostate Magnetic Resonance Imaging
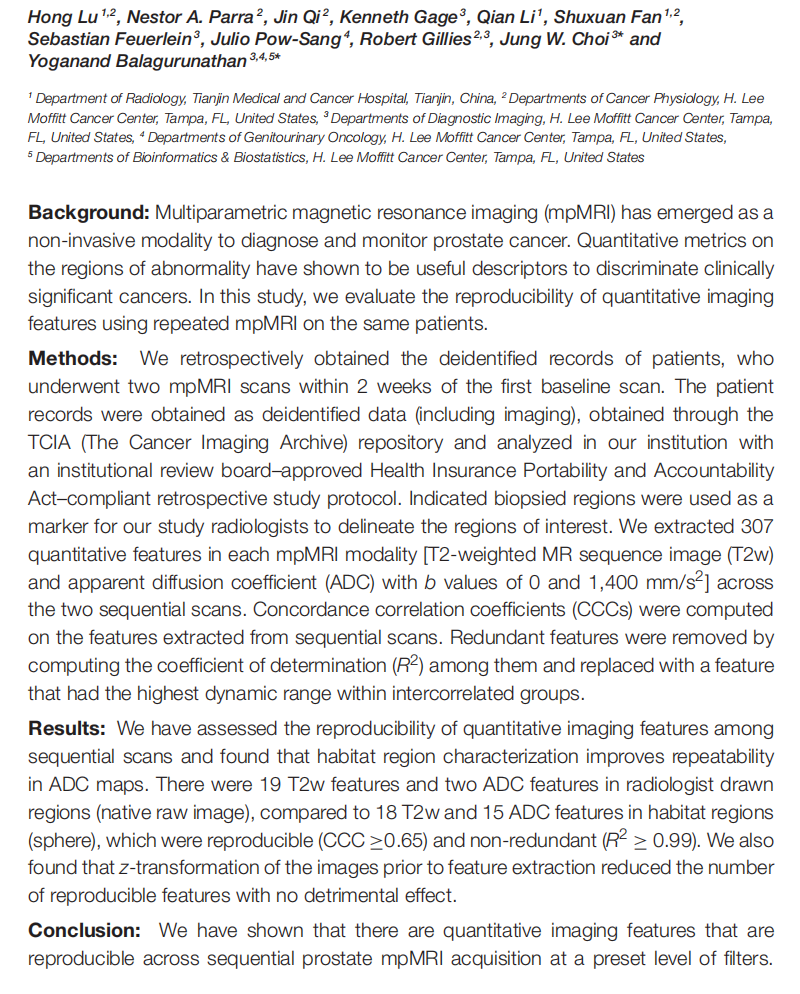

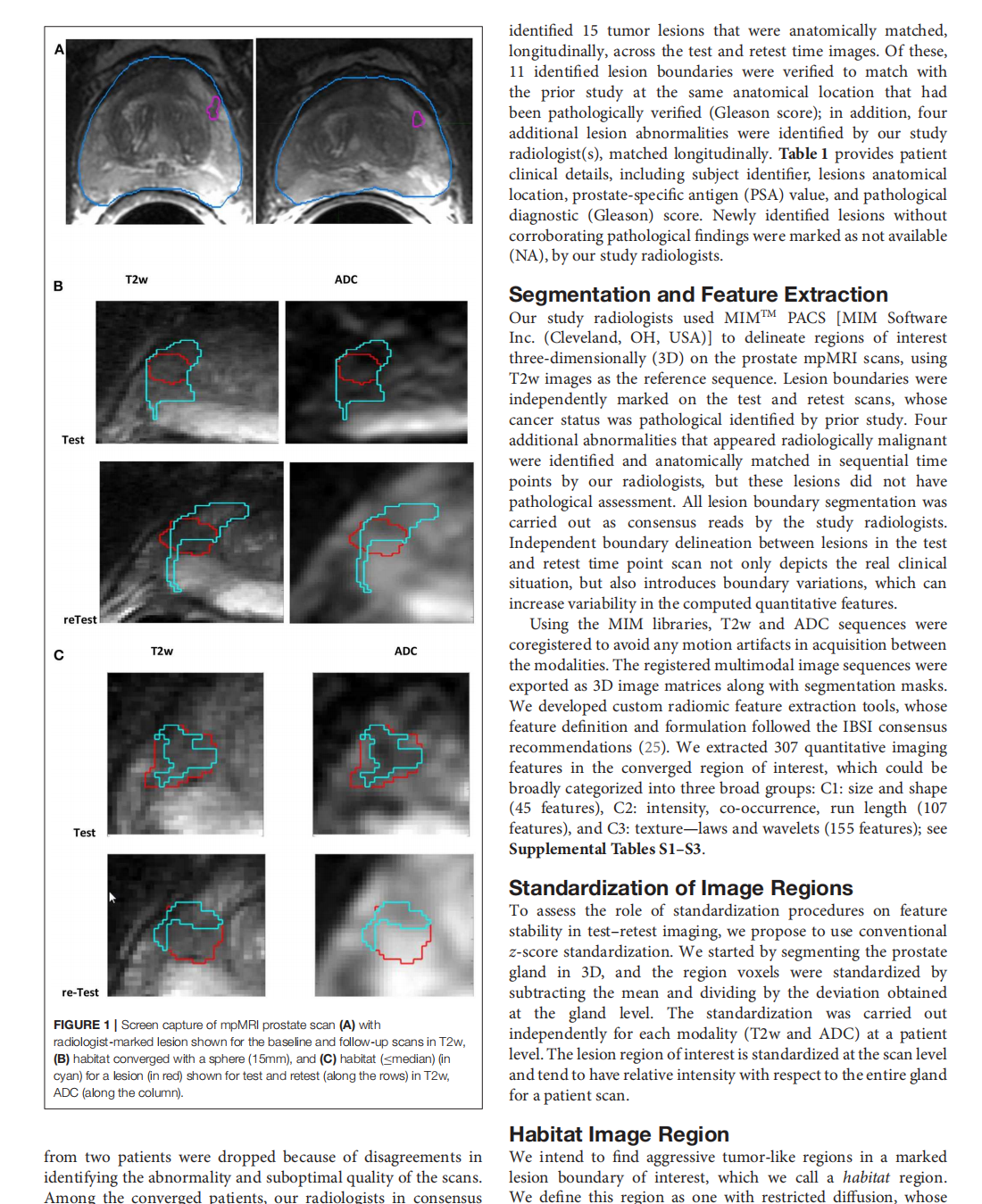
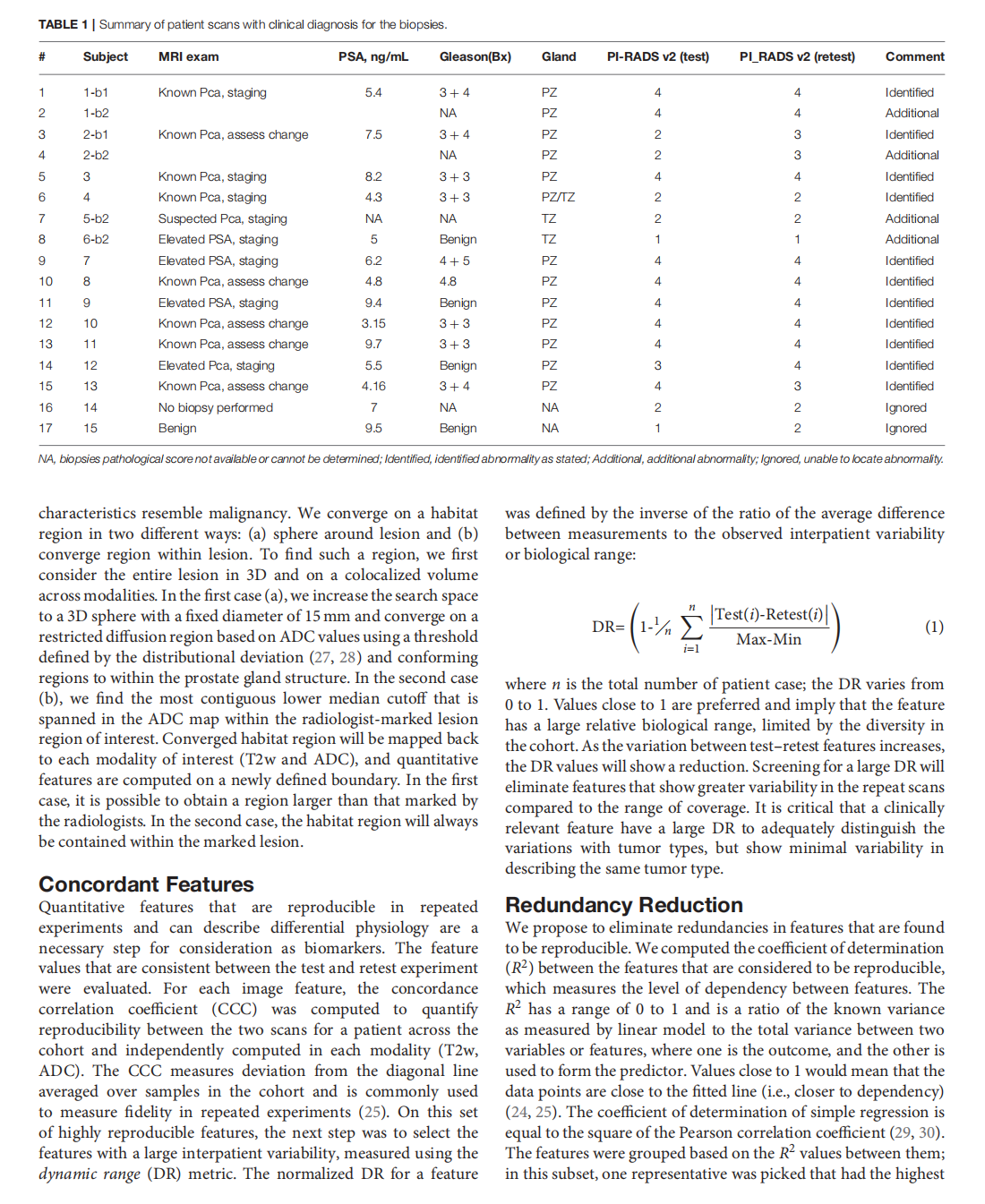
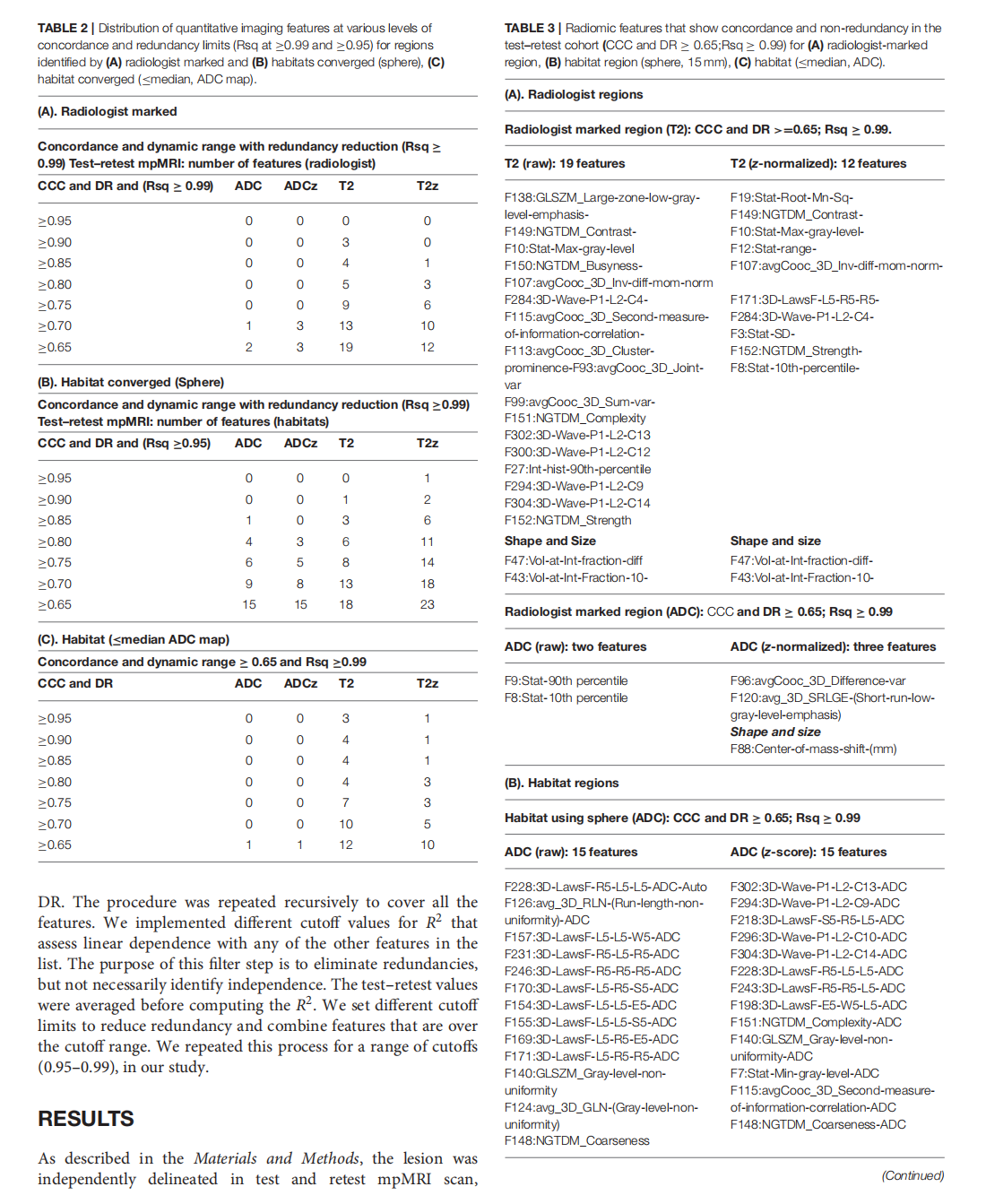

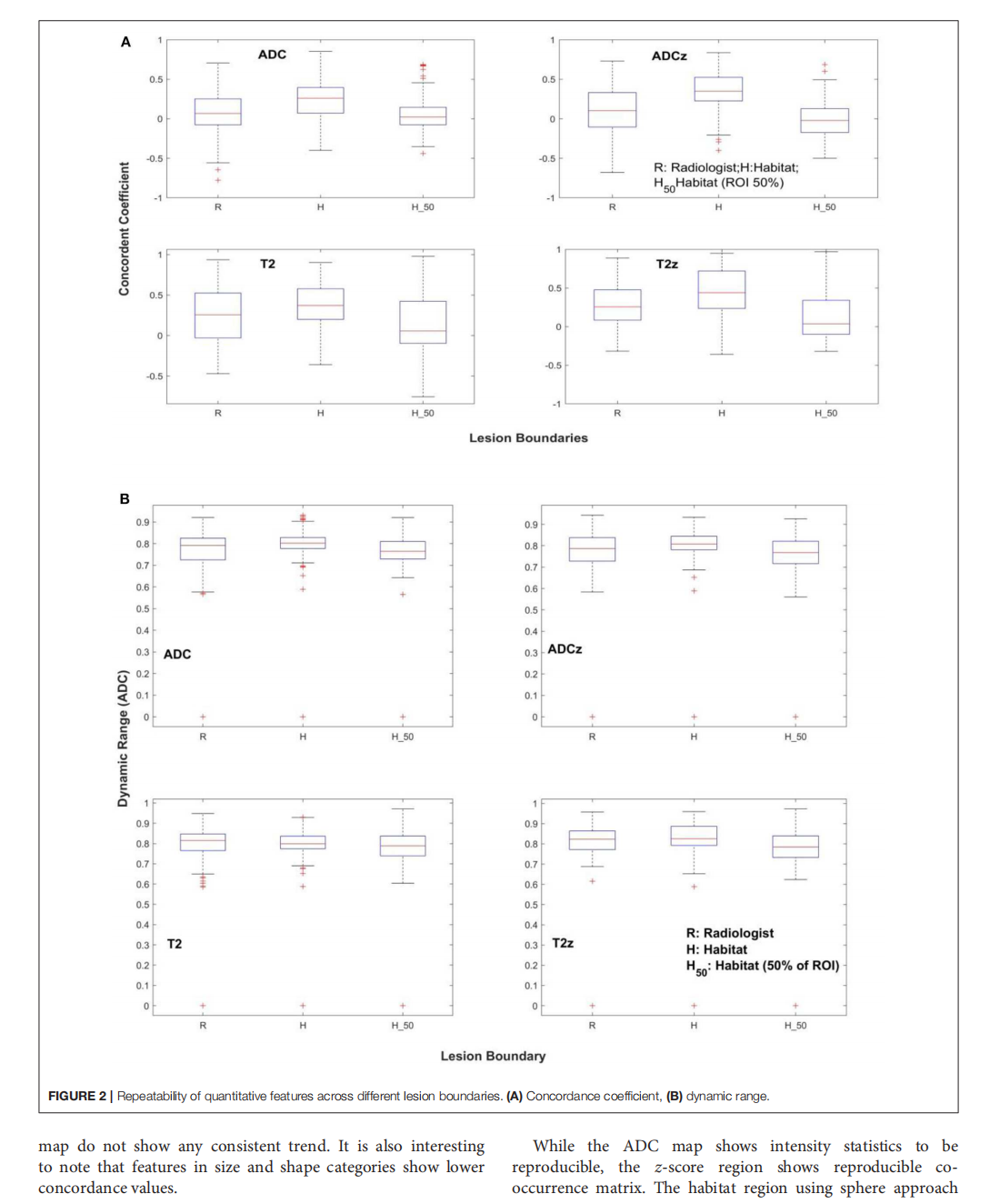
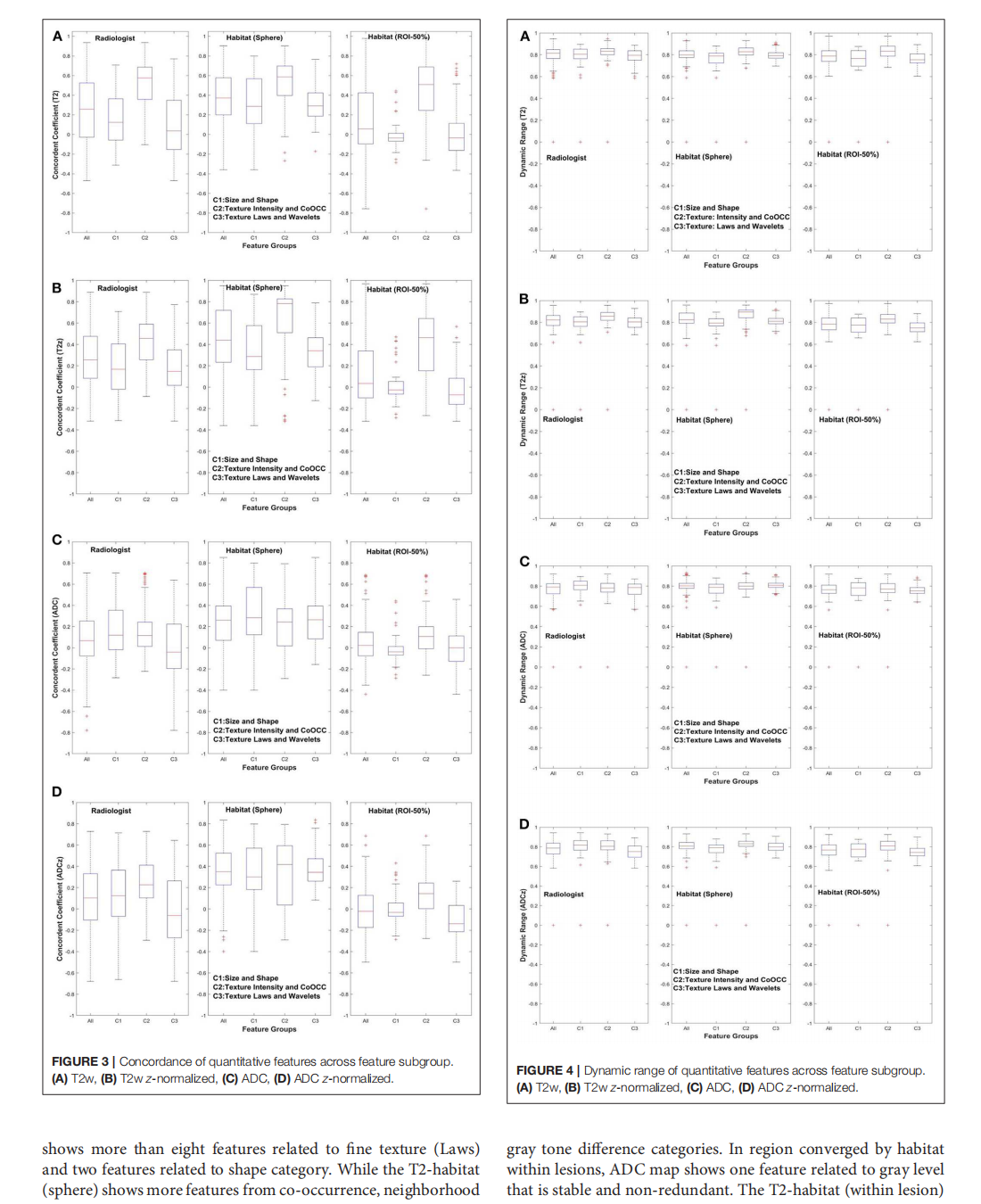

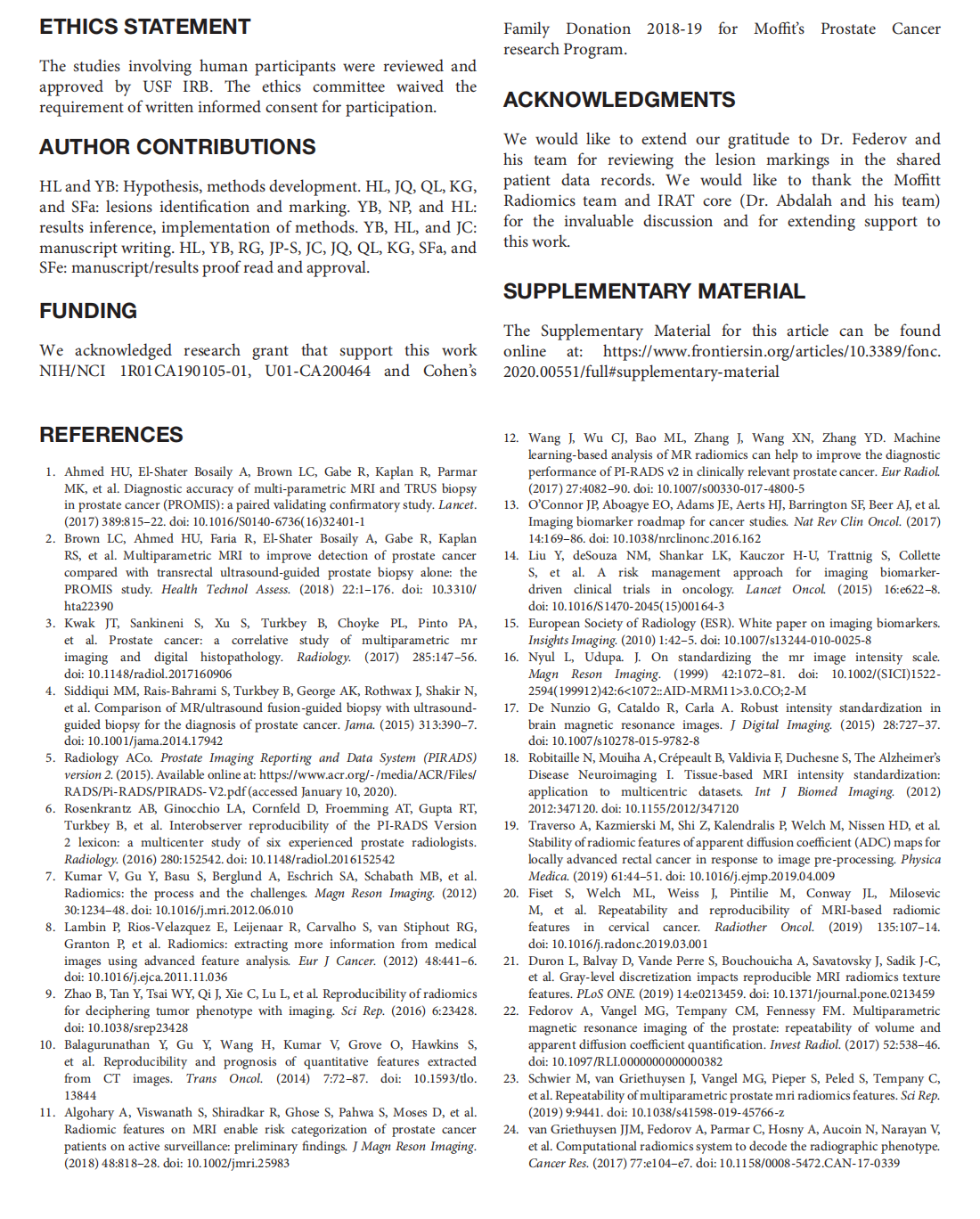
This article is excerpted from the 《Frontiers in Oncology》by Wound World
- 星期三, 10 12月 2025
Still Wanting to Win: Reward System Stability in Healthy Aging



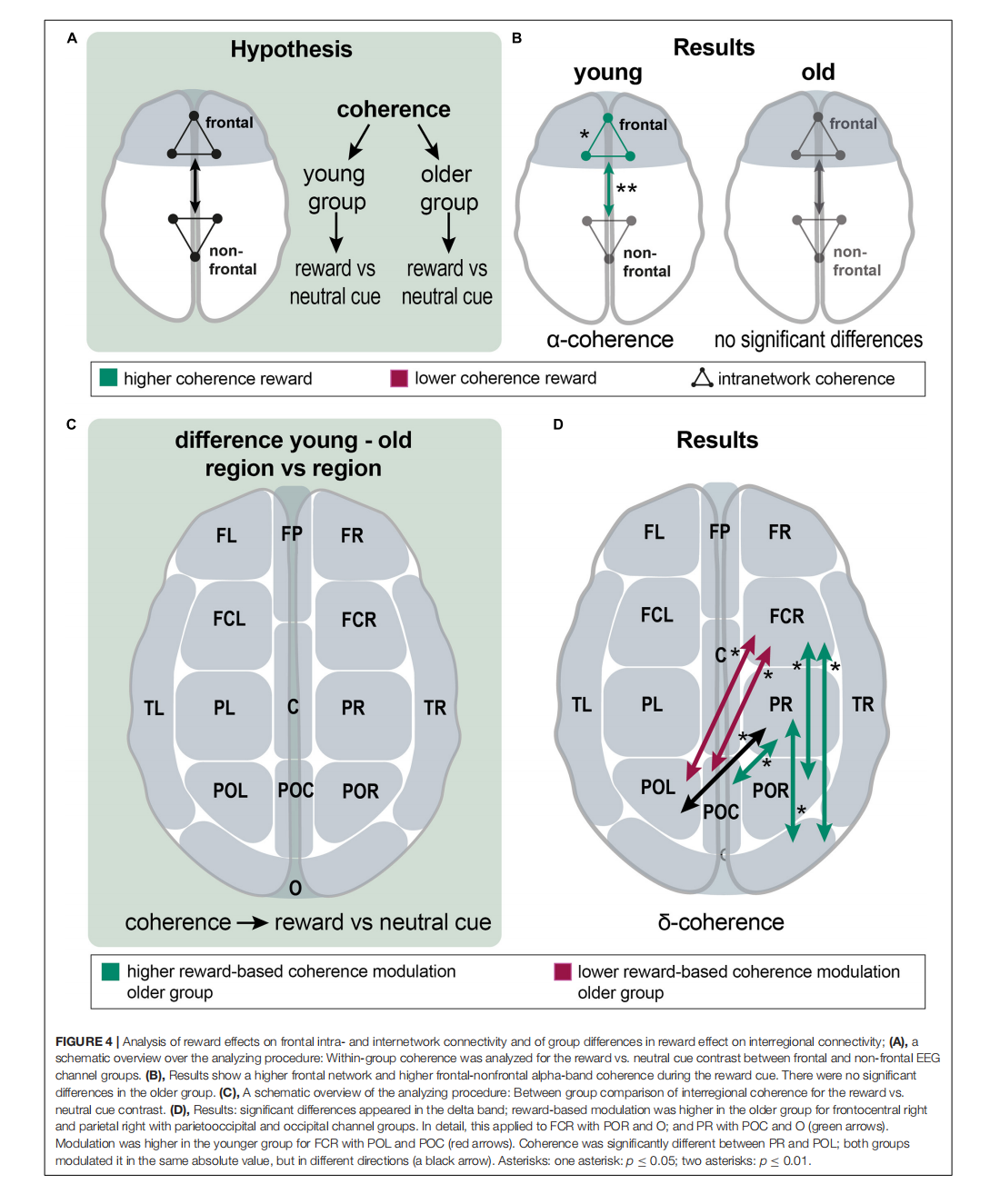
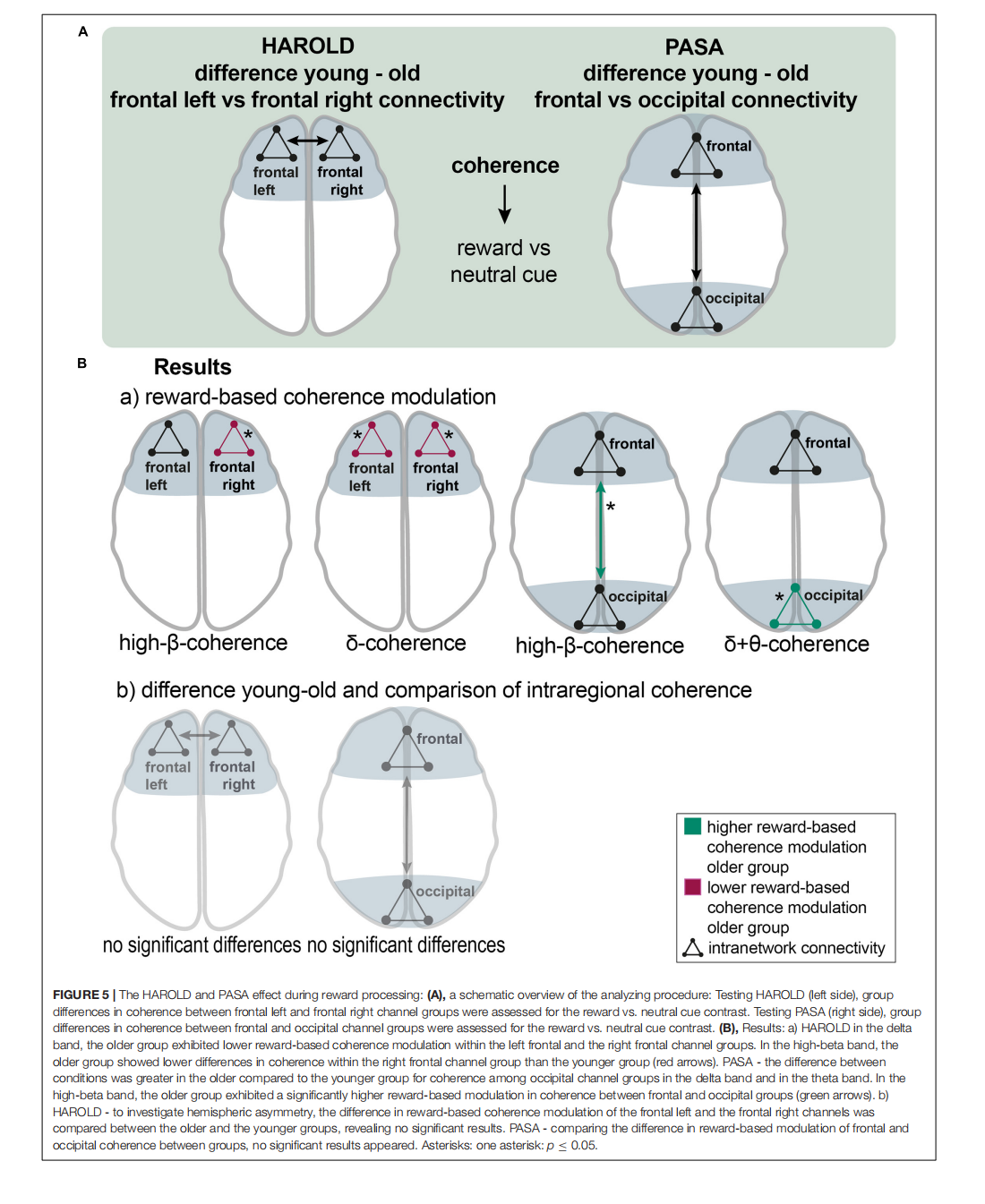
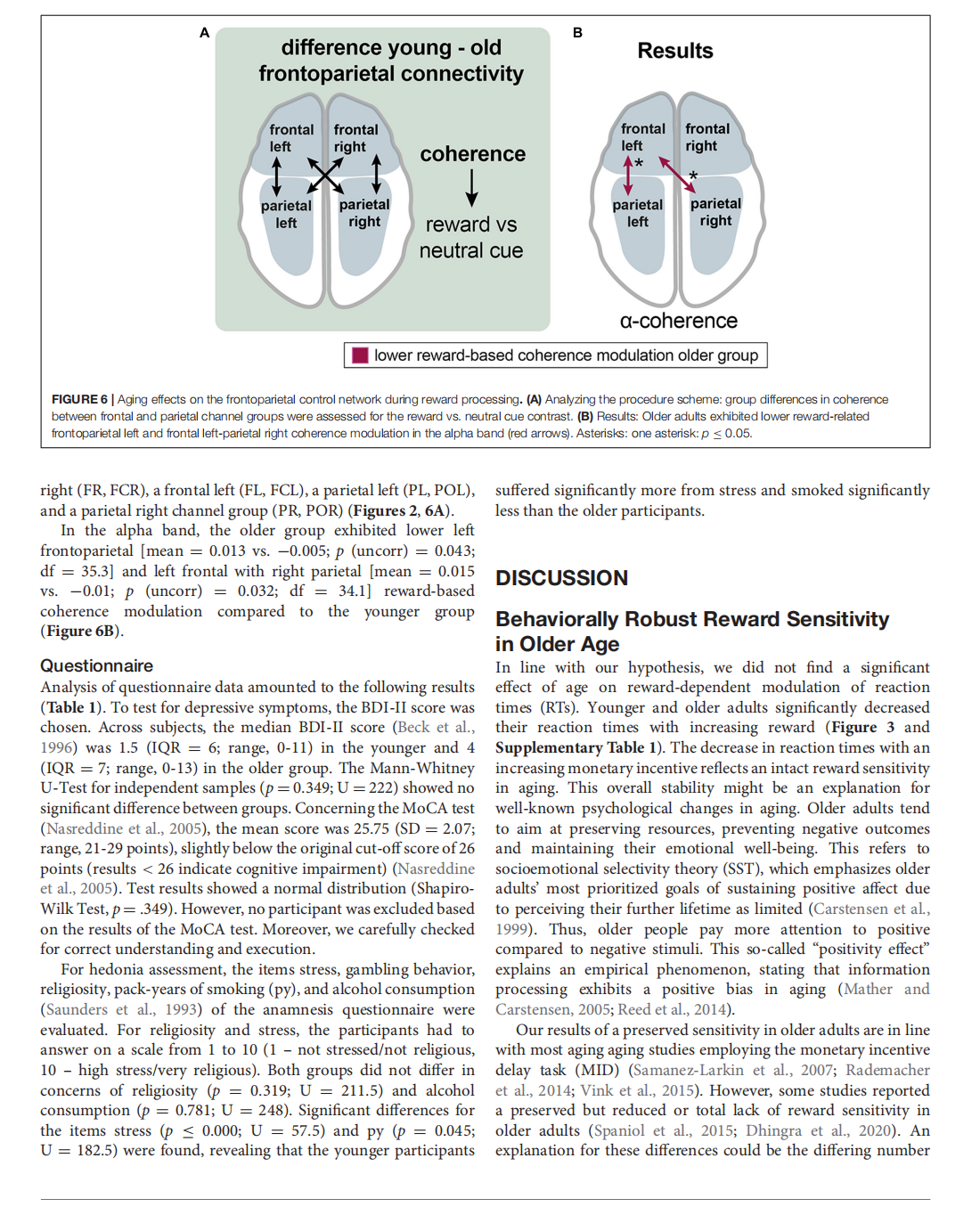





This article is excerpted from the《Frontiers in Aging Neuroscience》 by Wound World

- 星期二, 09 12月 2025
Comparative efficacy of Jaungo, a traditional herbal ointment, and a water-in-oil type non-steroidal moisturizer for radiation-induced dermatitis in patients with breast cancer: a prospective, randomized, single-blind, pilot study

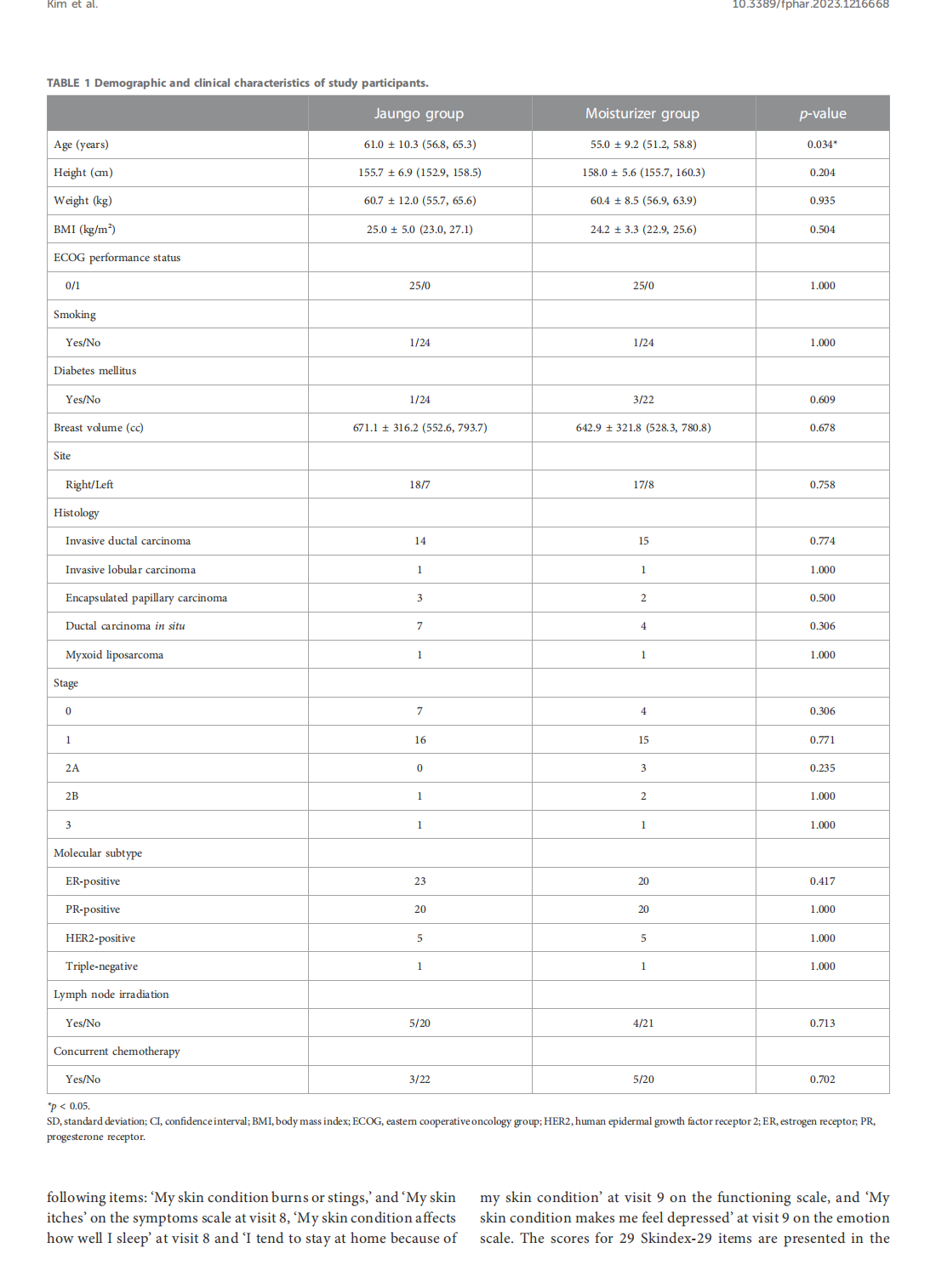
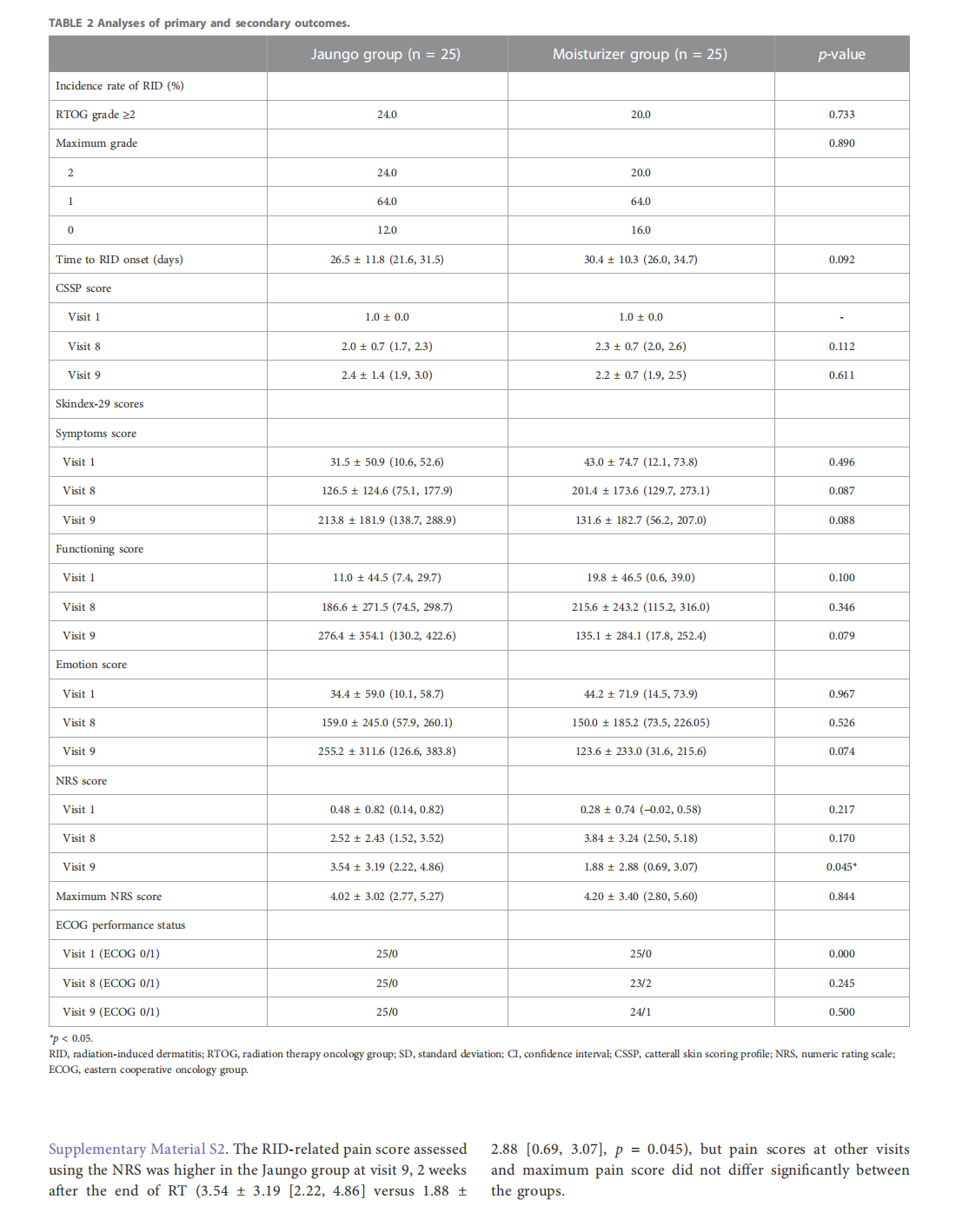
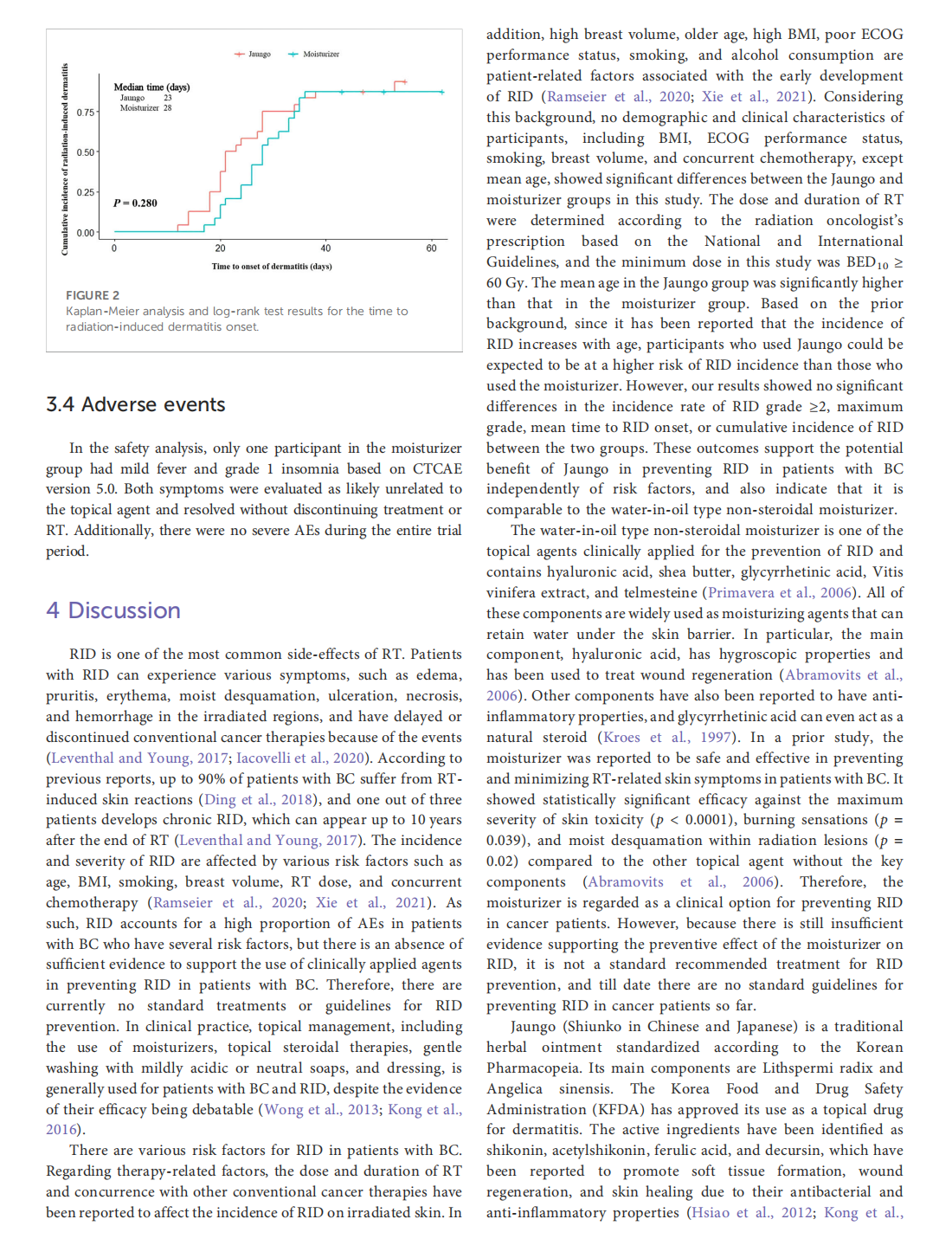
This article is excerpted from the《Frontiers in Pharmacology》by Wound World
- 星期一, 08 12月 2025
Polyadenylated Telomeric Noncoding RNA Functions as a Pivotal Therapeutic Target of Anti-Ageing to Stabilize Telomere Length of Chromosomes Via Collaborating With Zscan4c
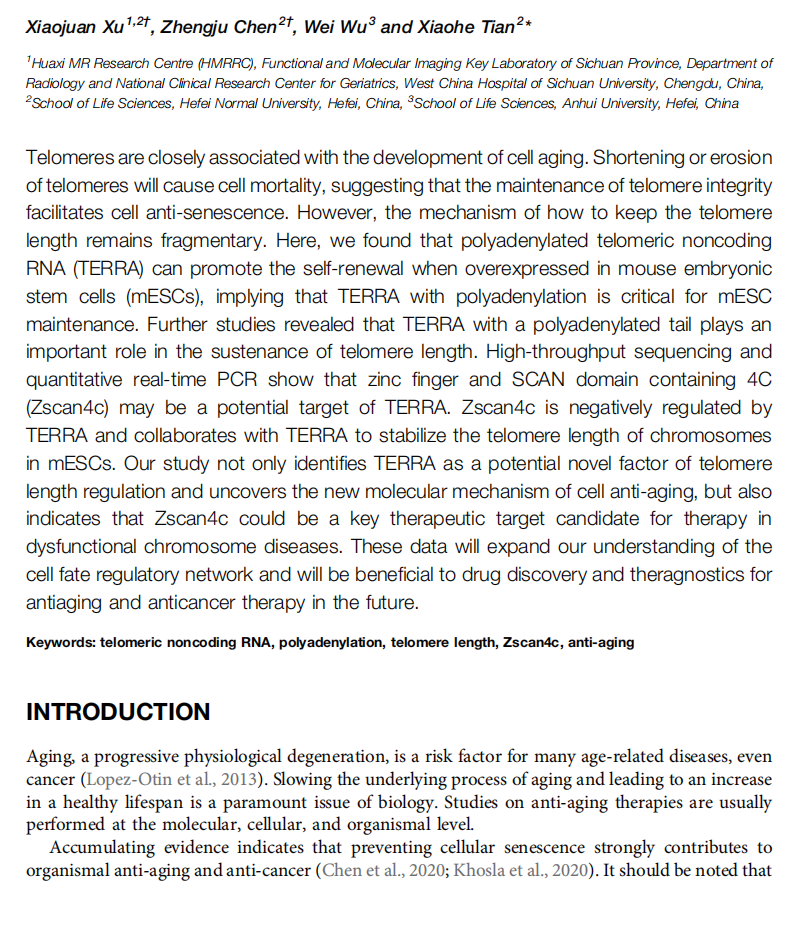


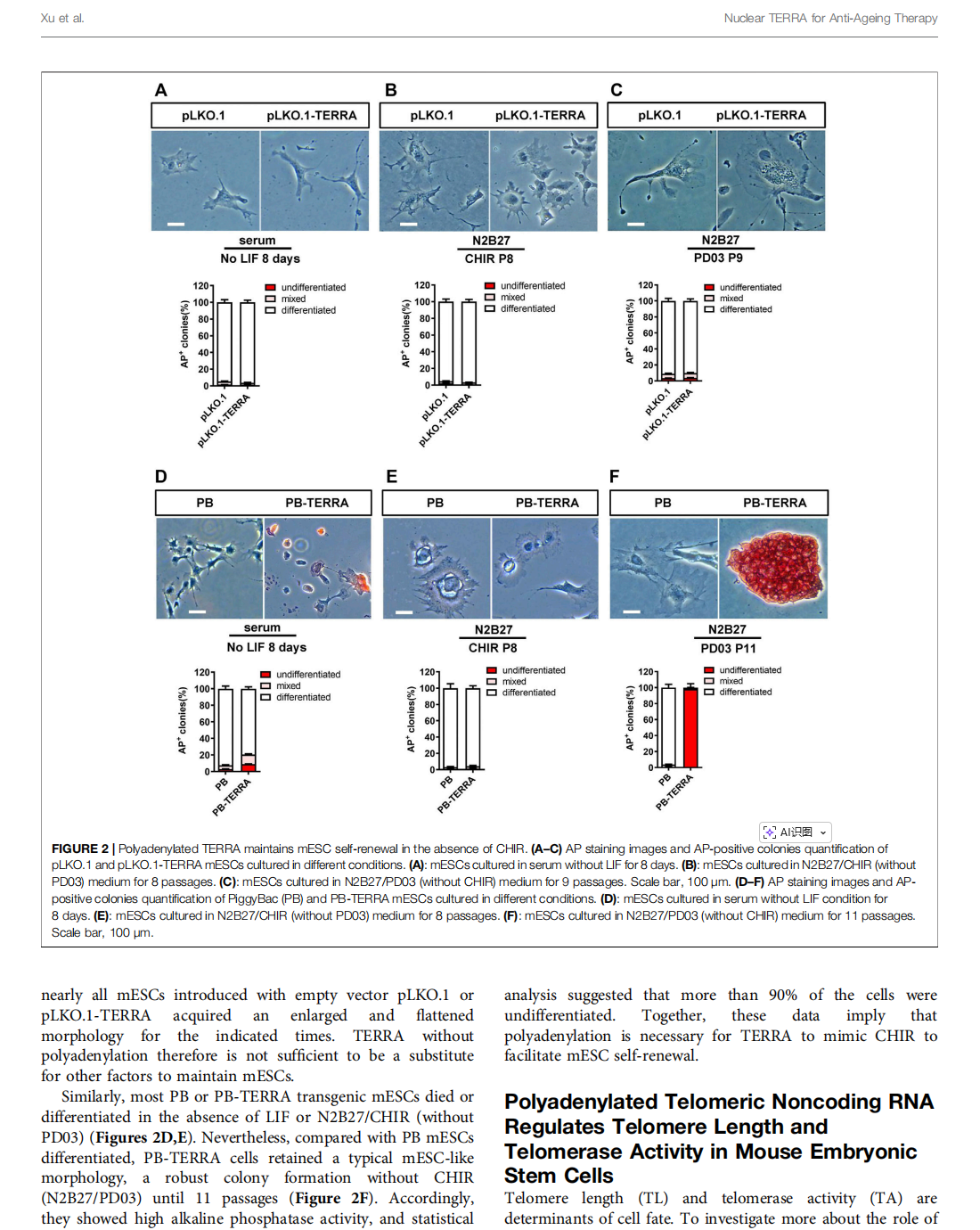


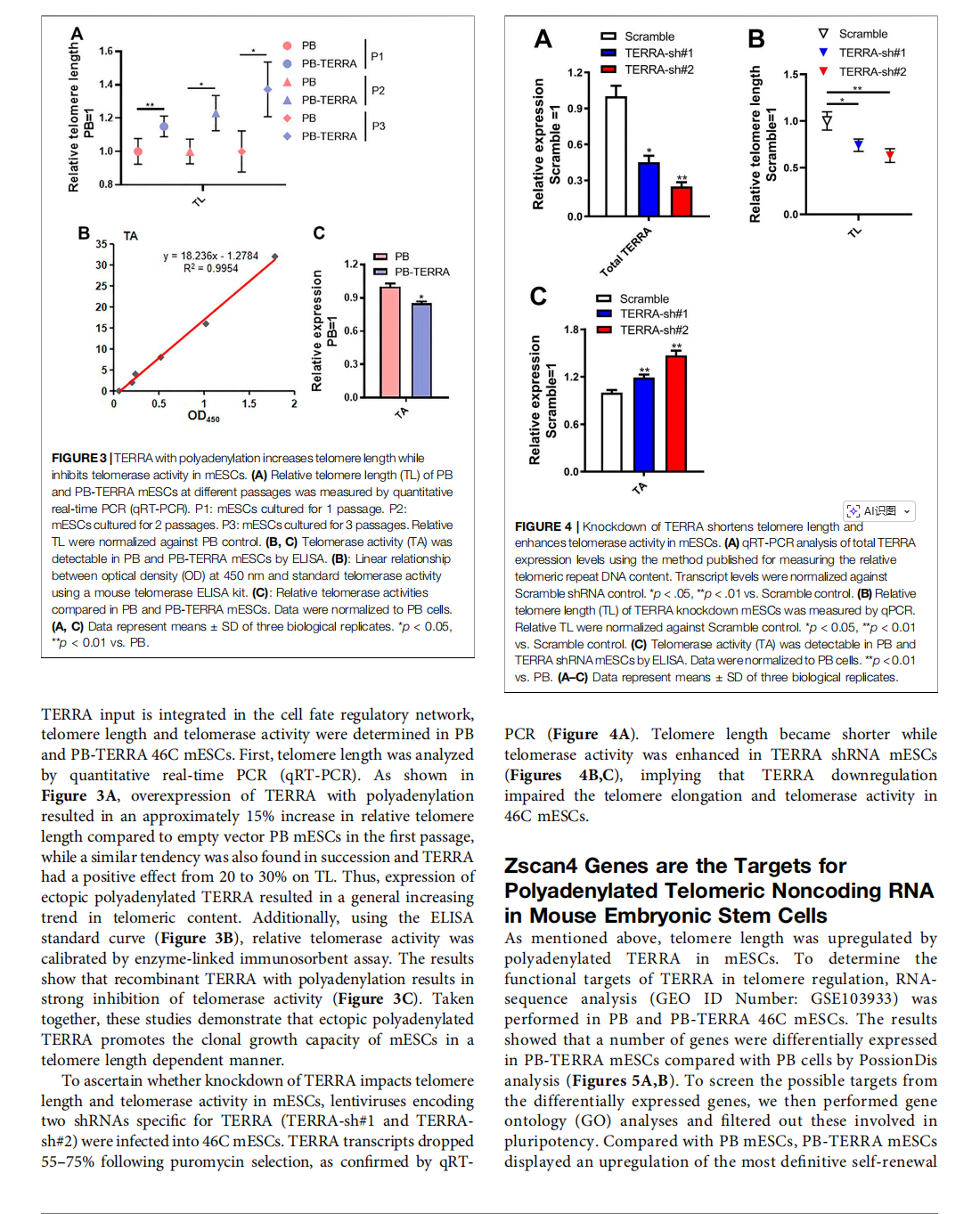
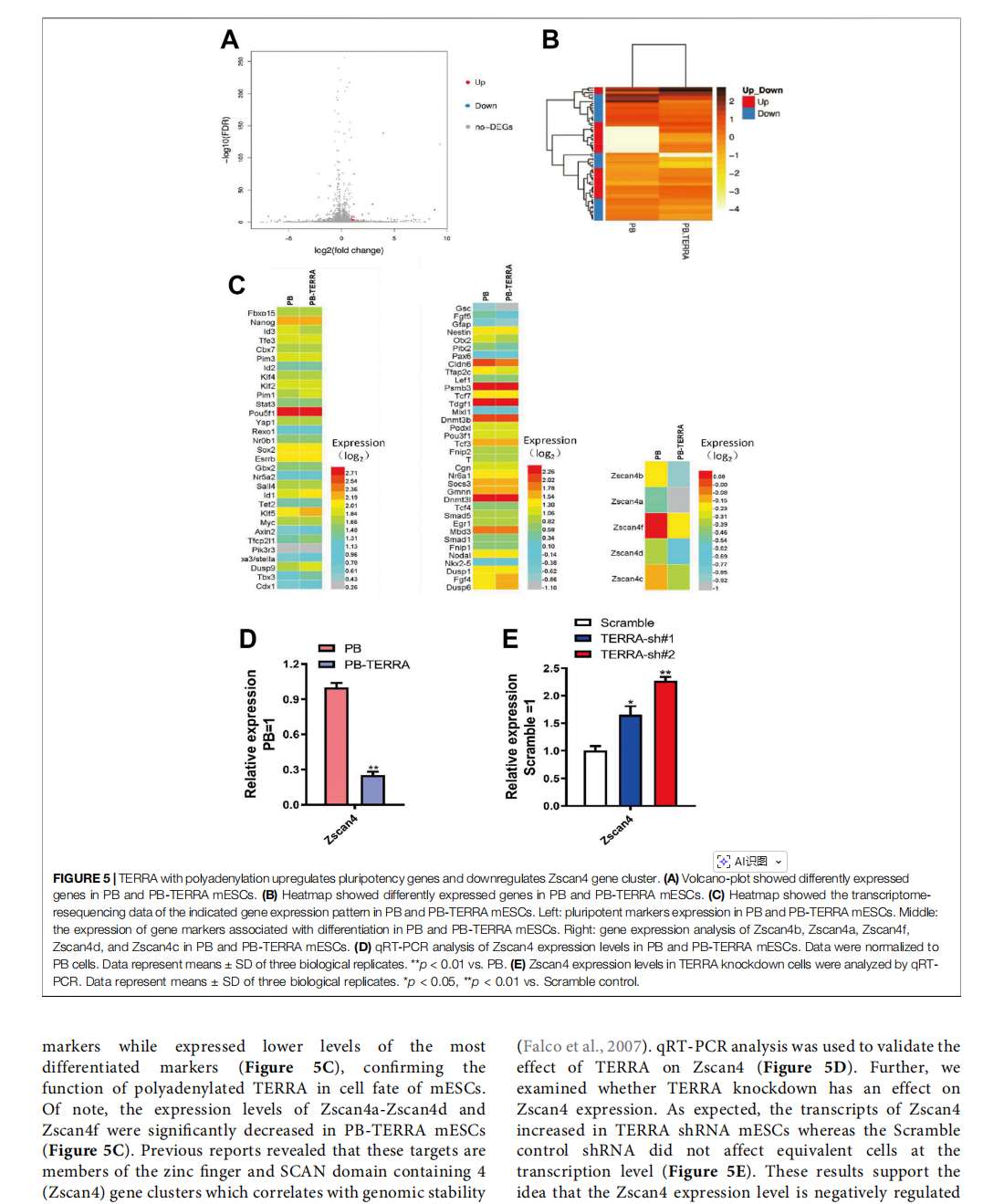
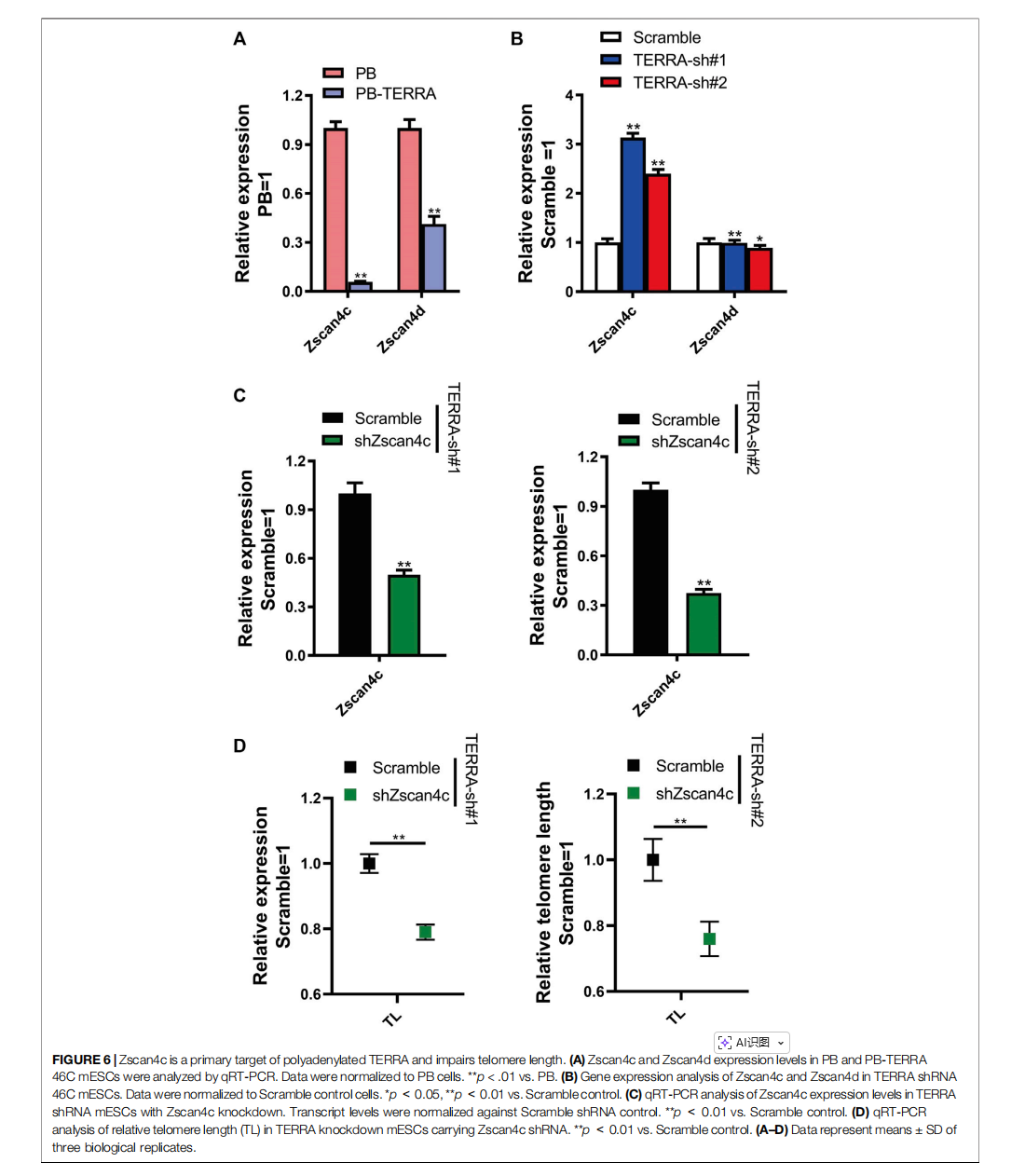



This article is excerpted from the《Frontiers in Pharmacology》by Wound World

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}