
伤口世界
电子邮件地址: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。

- 星期四, 06 11月 2025
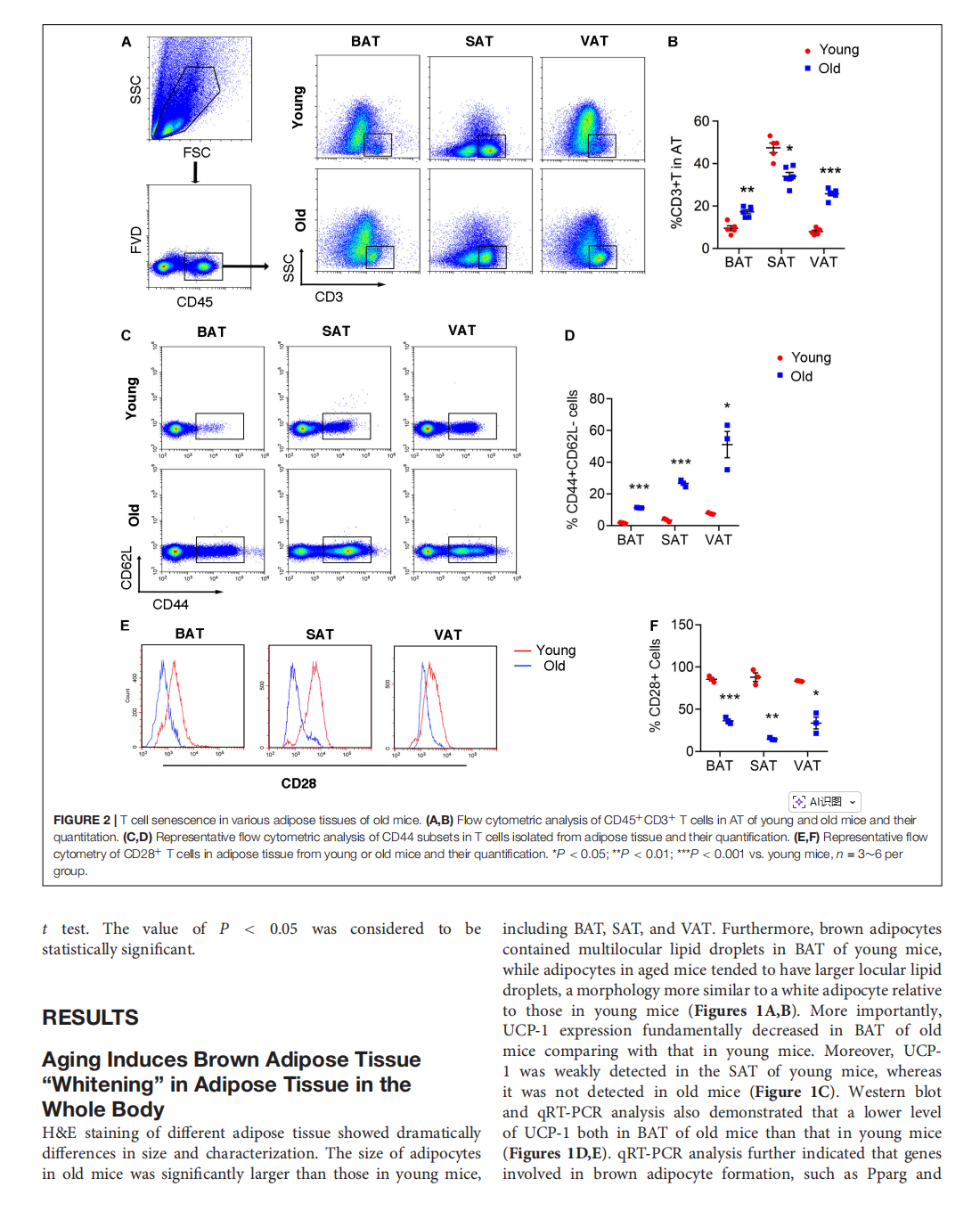
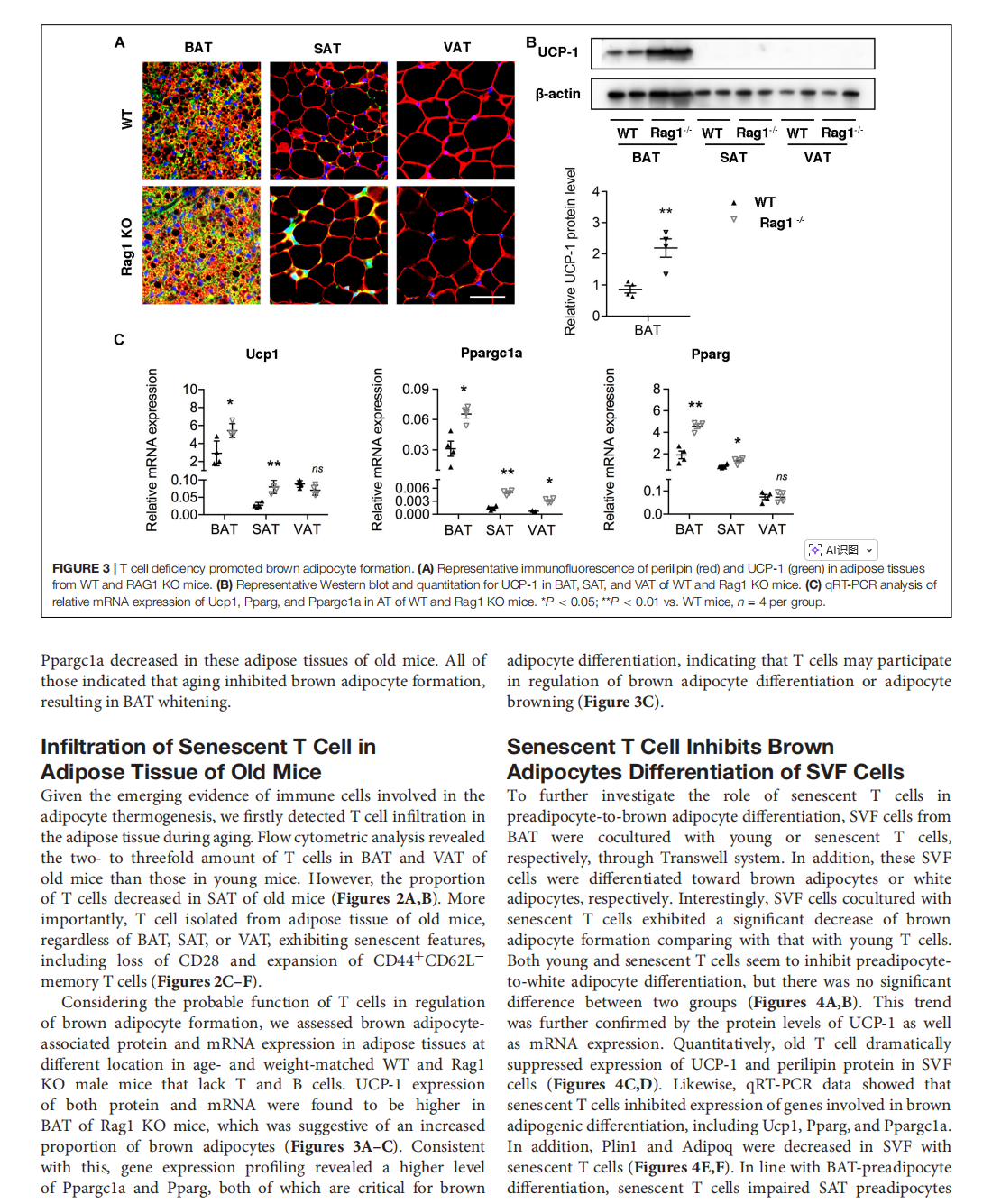
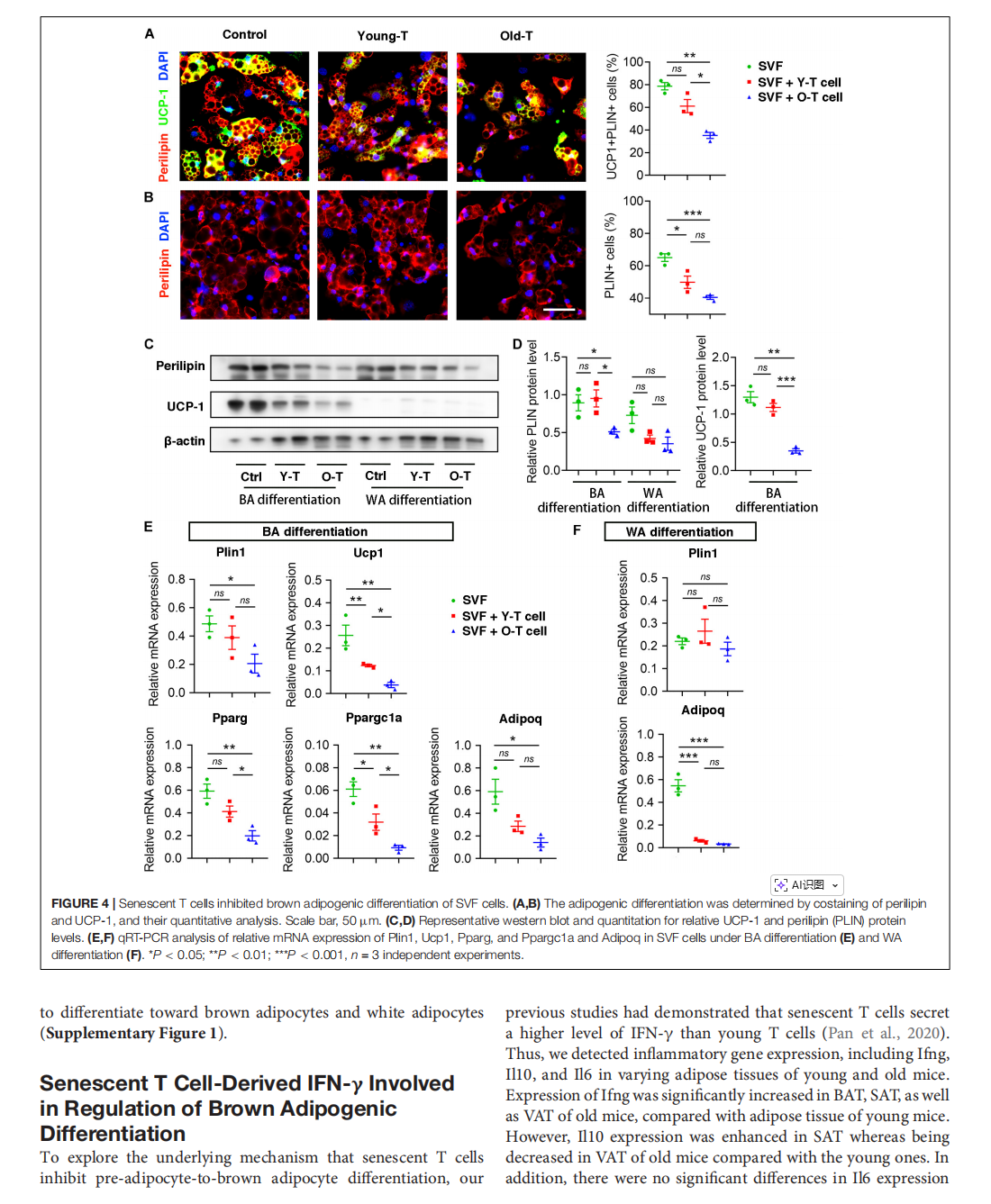
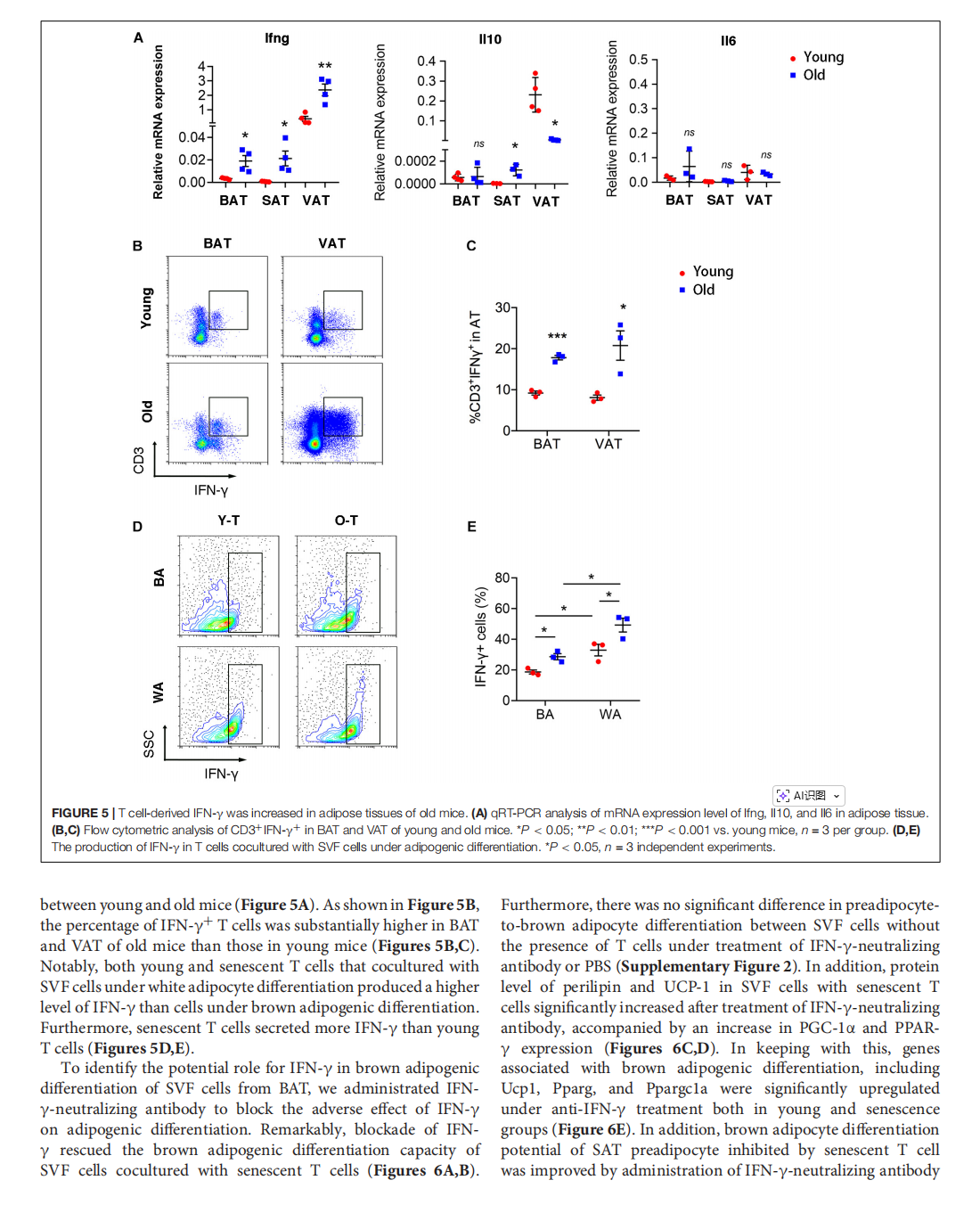
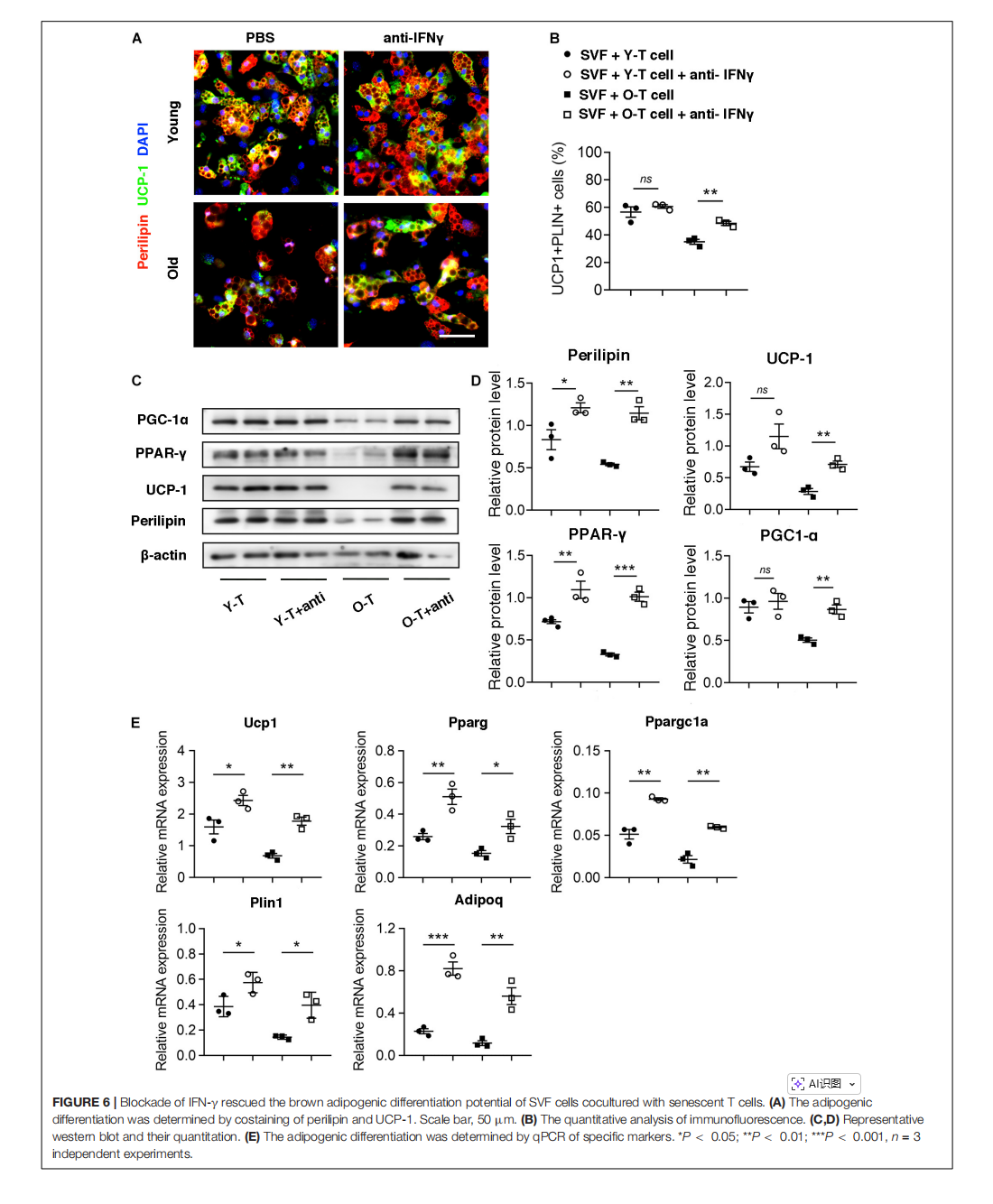
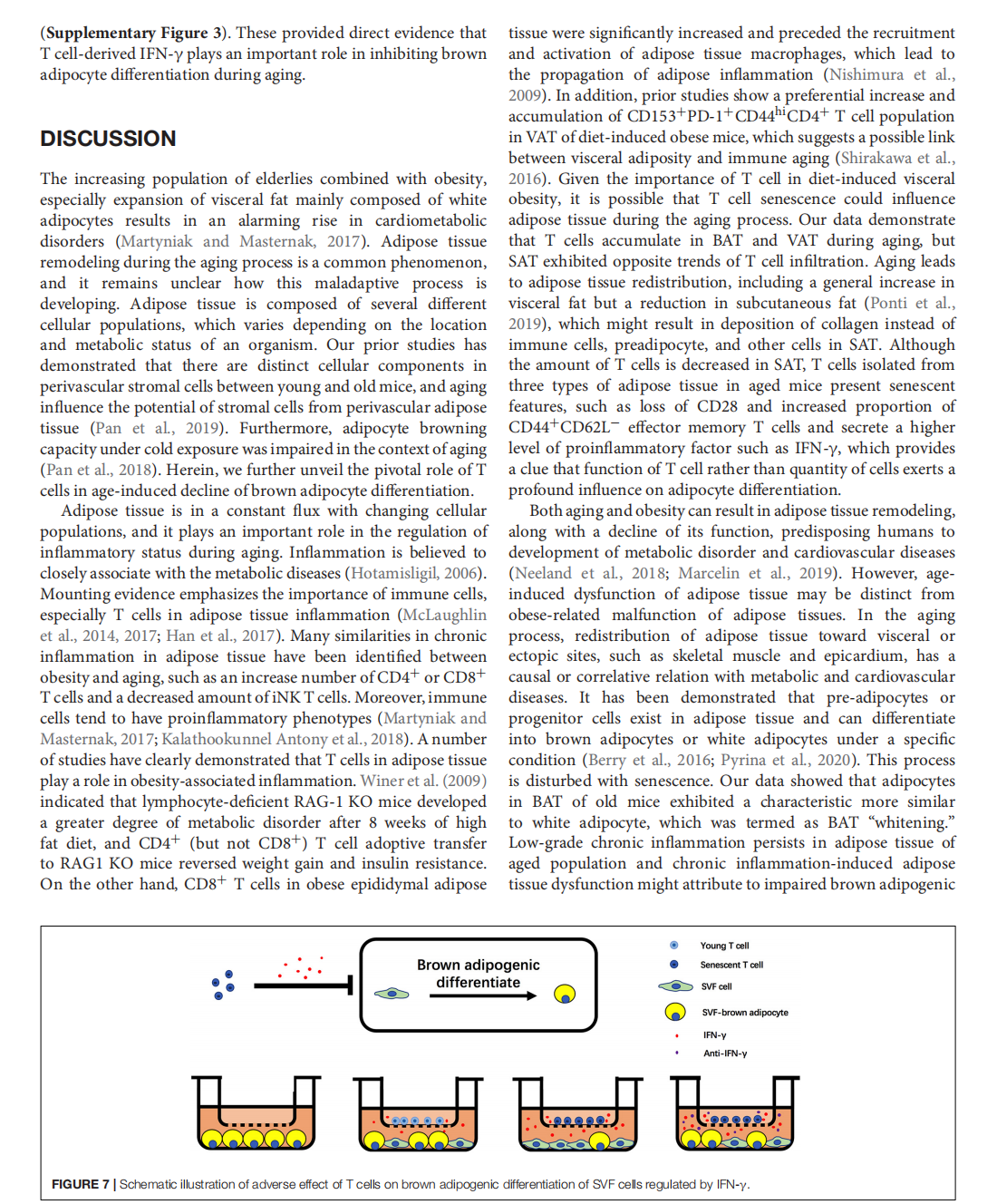
Senescent T Cell Induces Brown Adipose Tissue “Whitening” Via Secreting IFN-γ
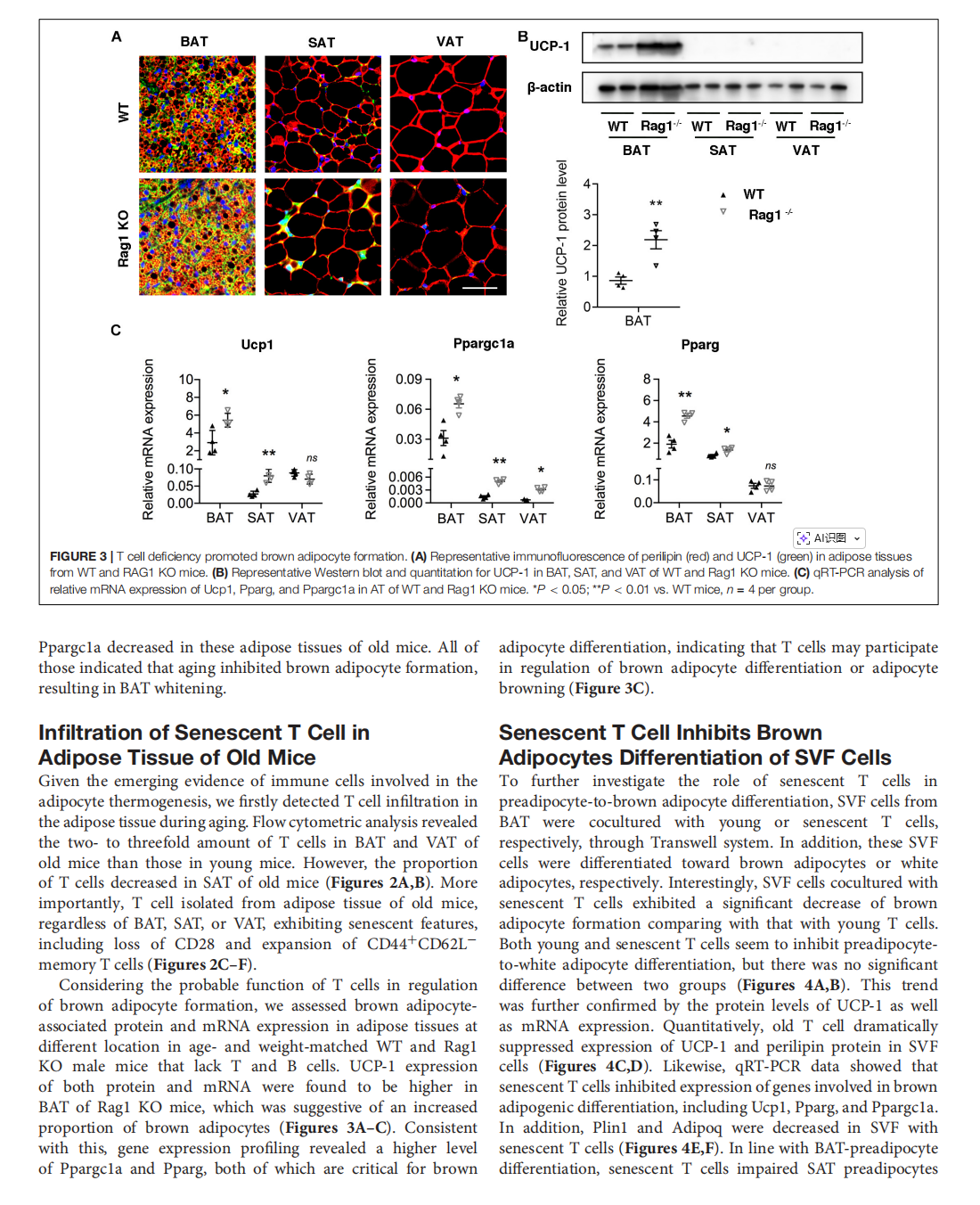
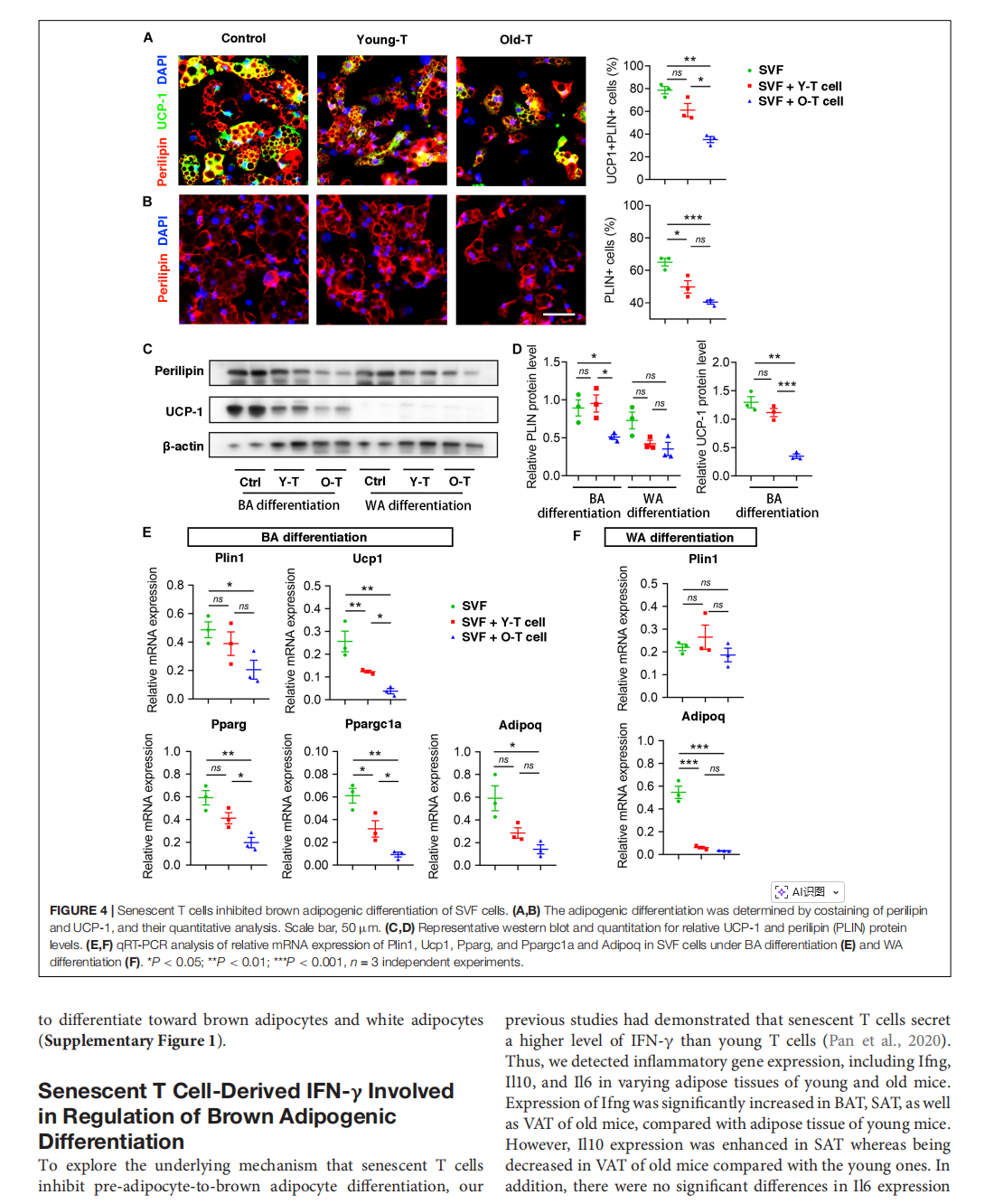
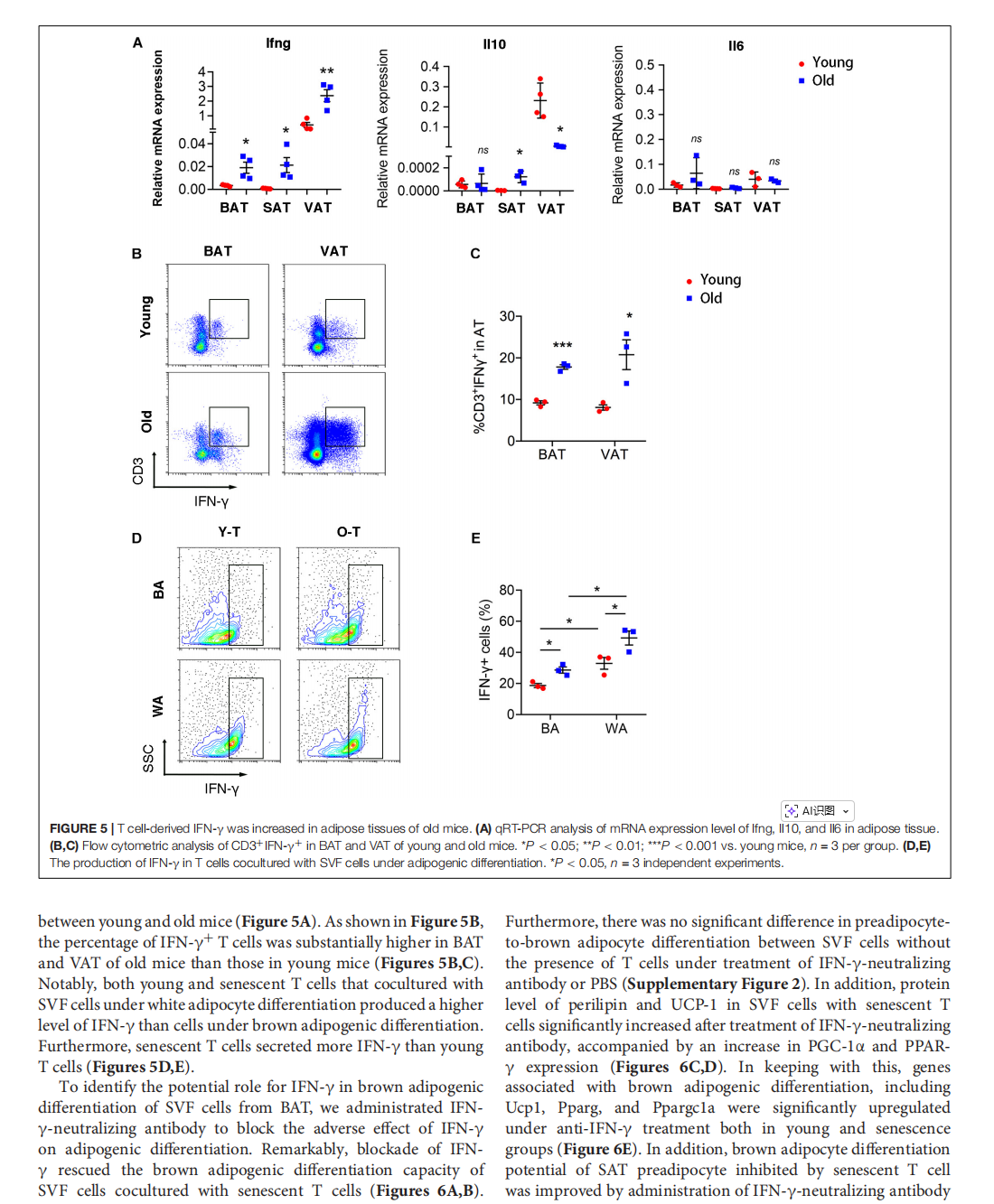
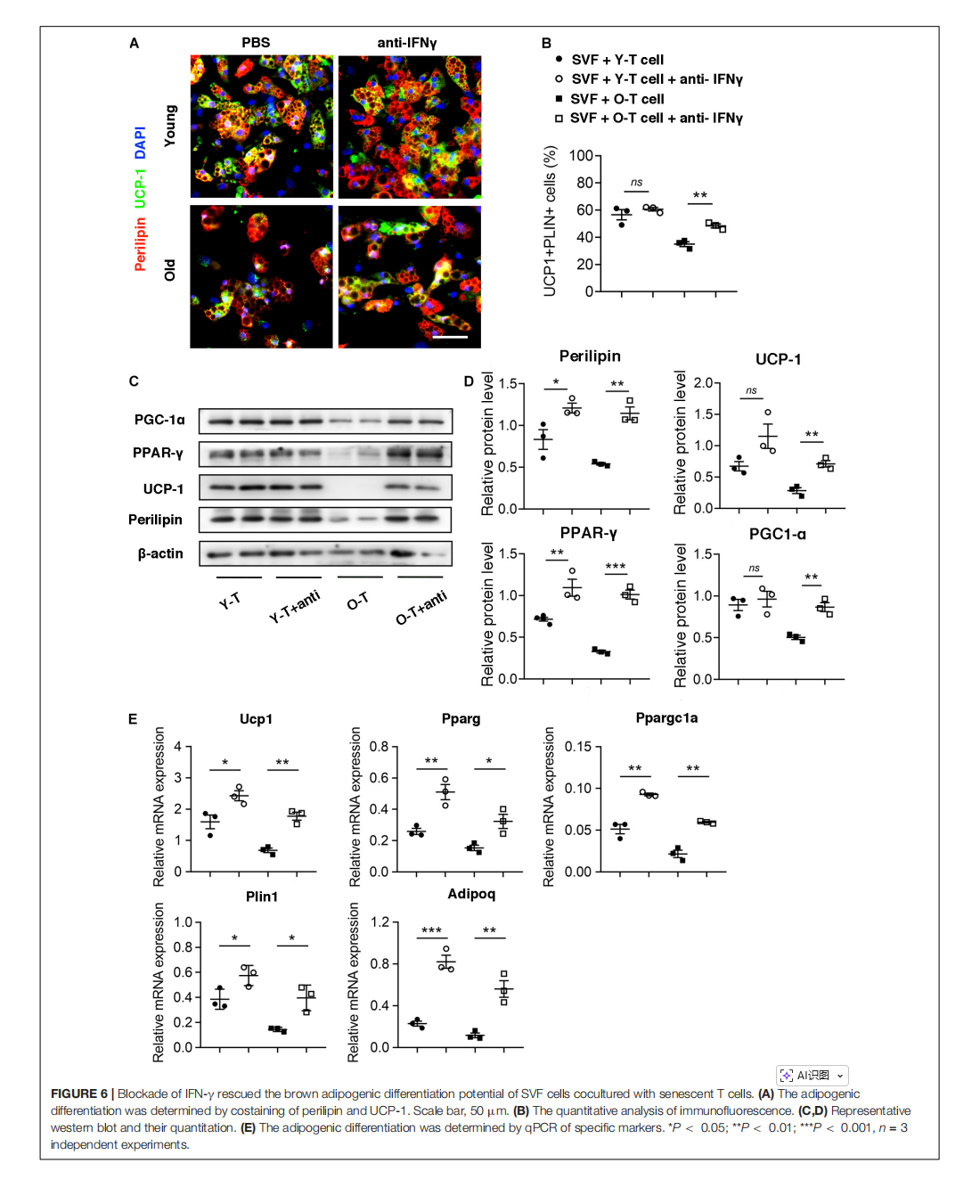

This article is excerpted from the《Frontiers in Cell and Developmental Biology》by Wound World
- 星期三, 05 11月 2025
Anti-Melanogenic Effect of Dendropanax morbiferus and Its Active Components via Protein Kinase A/Cyclic Adenosine Monophosphate-Responsive Binding Protein- and p38 Mitogen-Activated Protein Kinase-Mediated Microphthalmia−Associated Transcription Fact

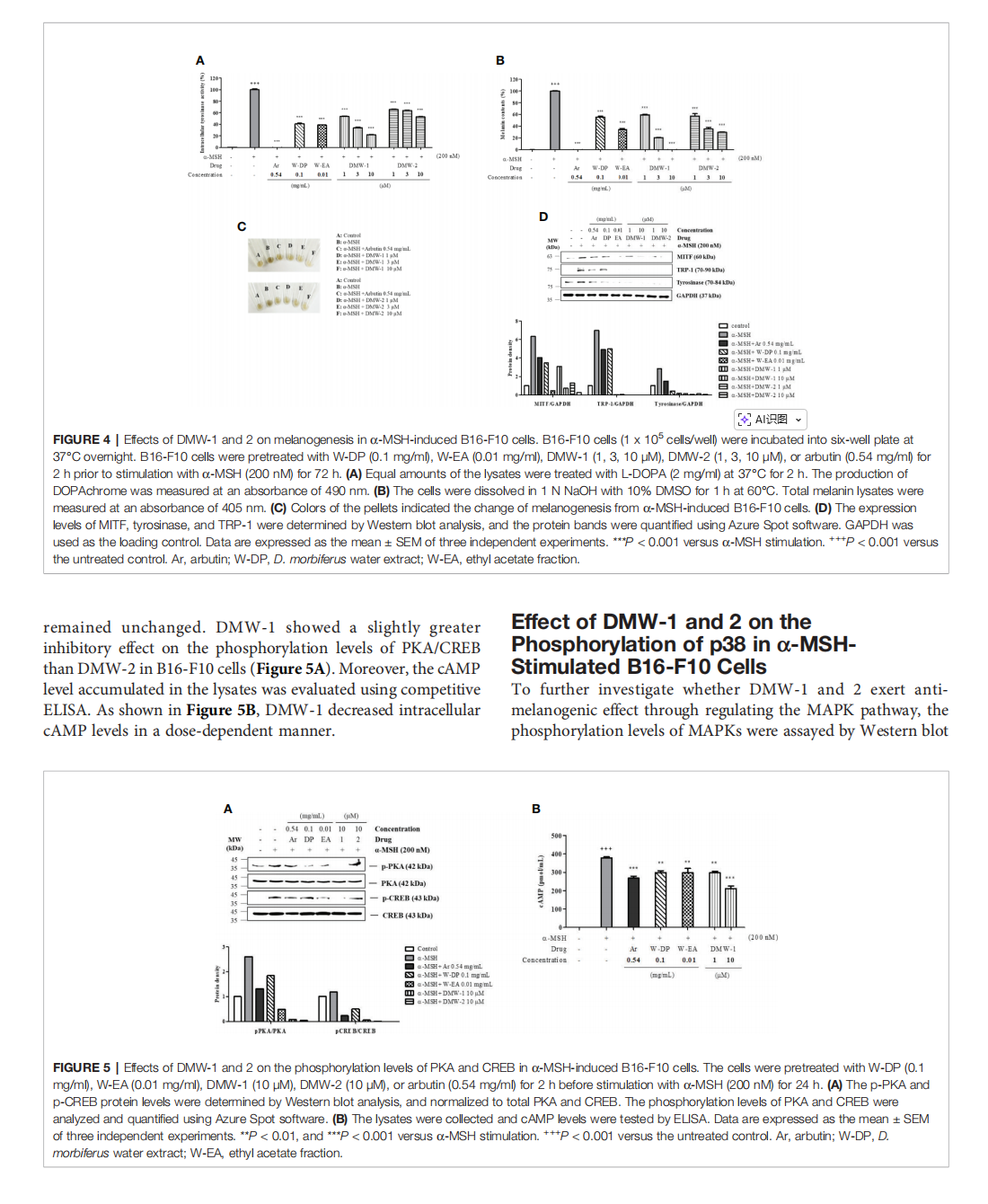

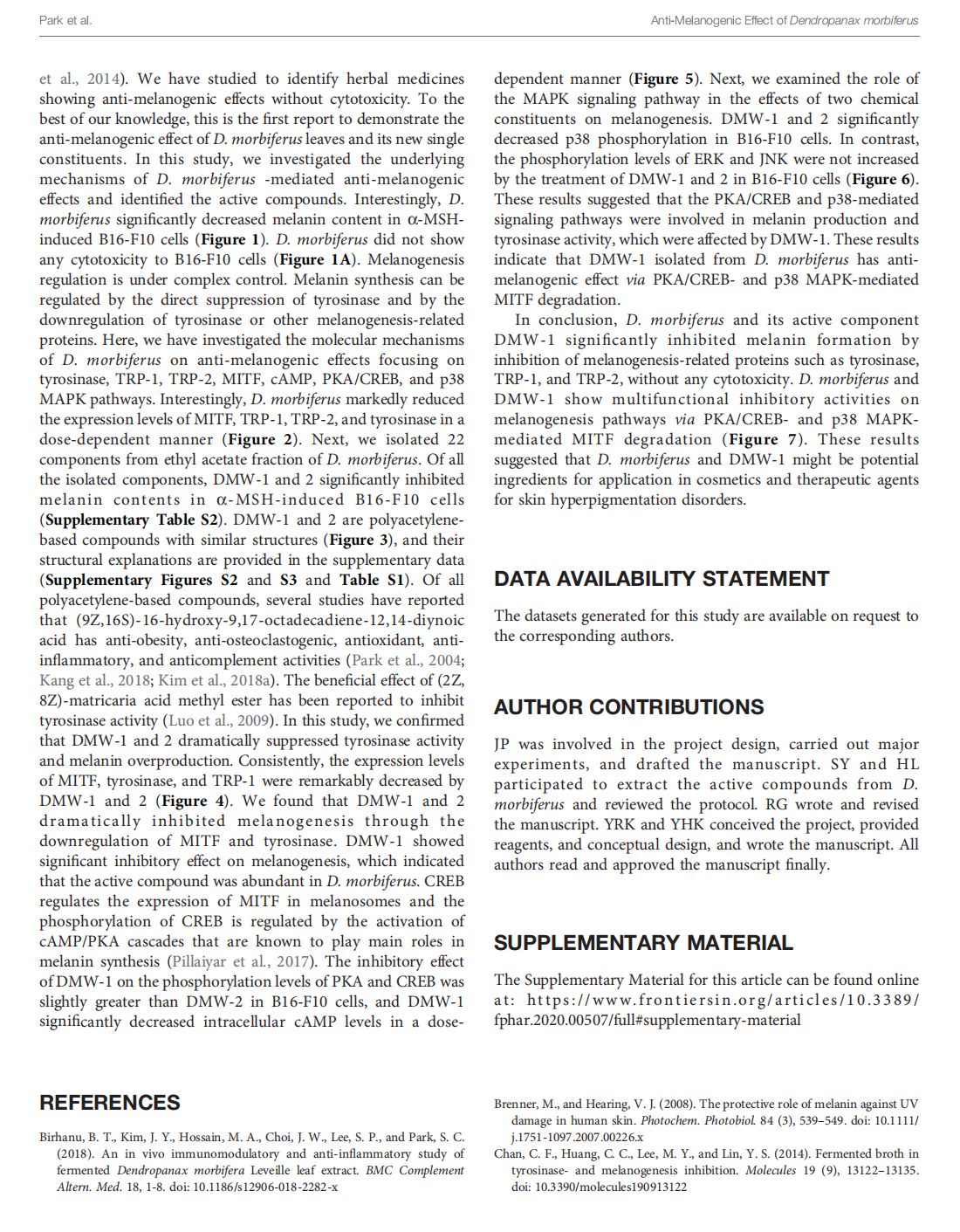

This article is excerpted from the 《Frontiers in Pharmacology》 by Wound World

- 星期二, 04 11月 2025
Plant and Microalgae Derived Peptides Are Advantageously Employed as Bioactive Compounds in Cosmetics





This article is excerpted from the 《Frontiers in Plant Science》 by Wound World

- 星期一, 03 11月 2025
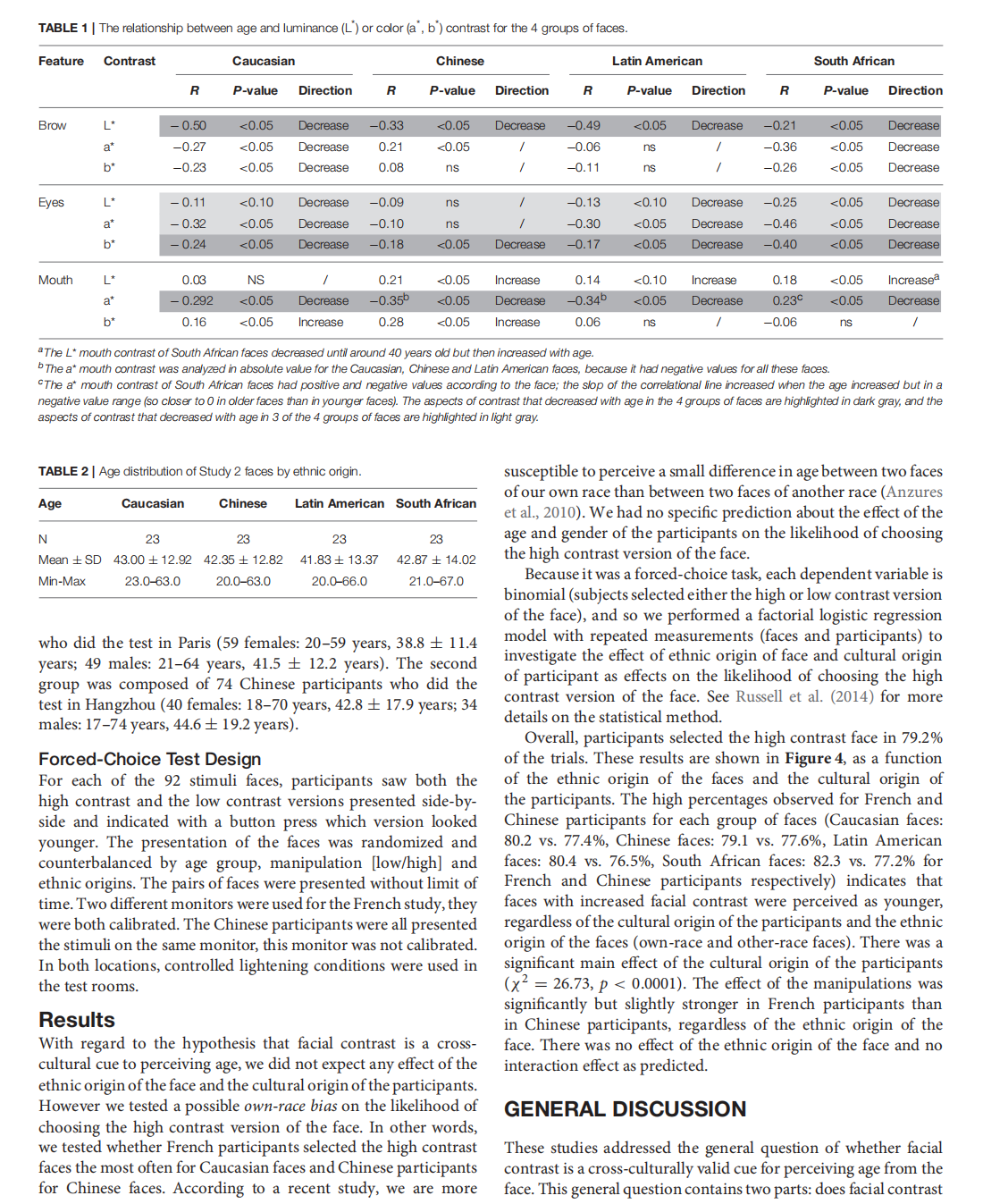
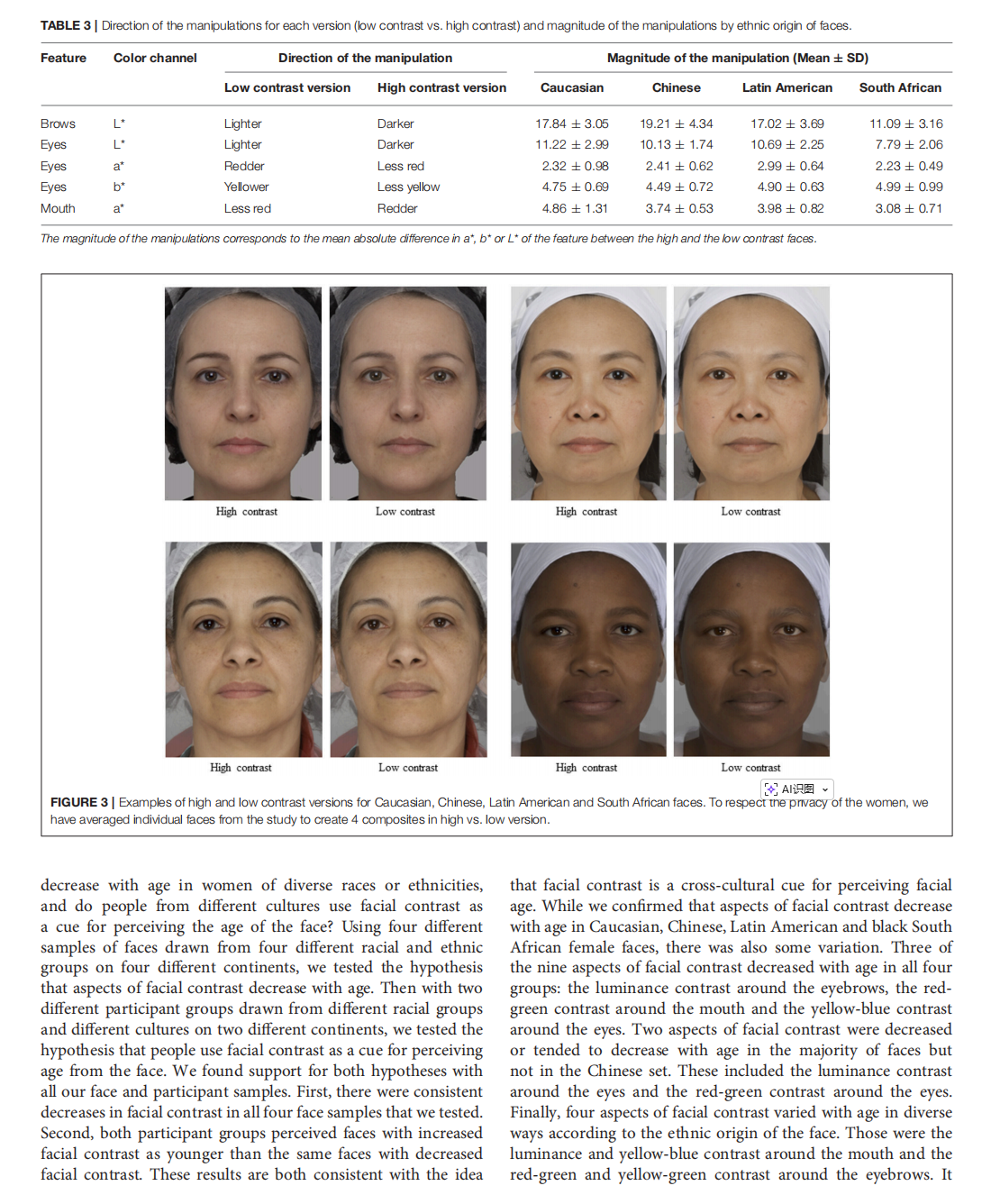
Facial Contrast Is a Cross-Cultural Cue for Perceiving Age



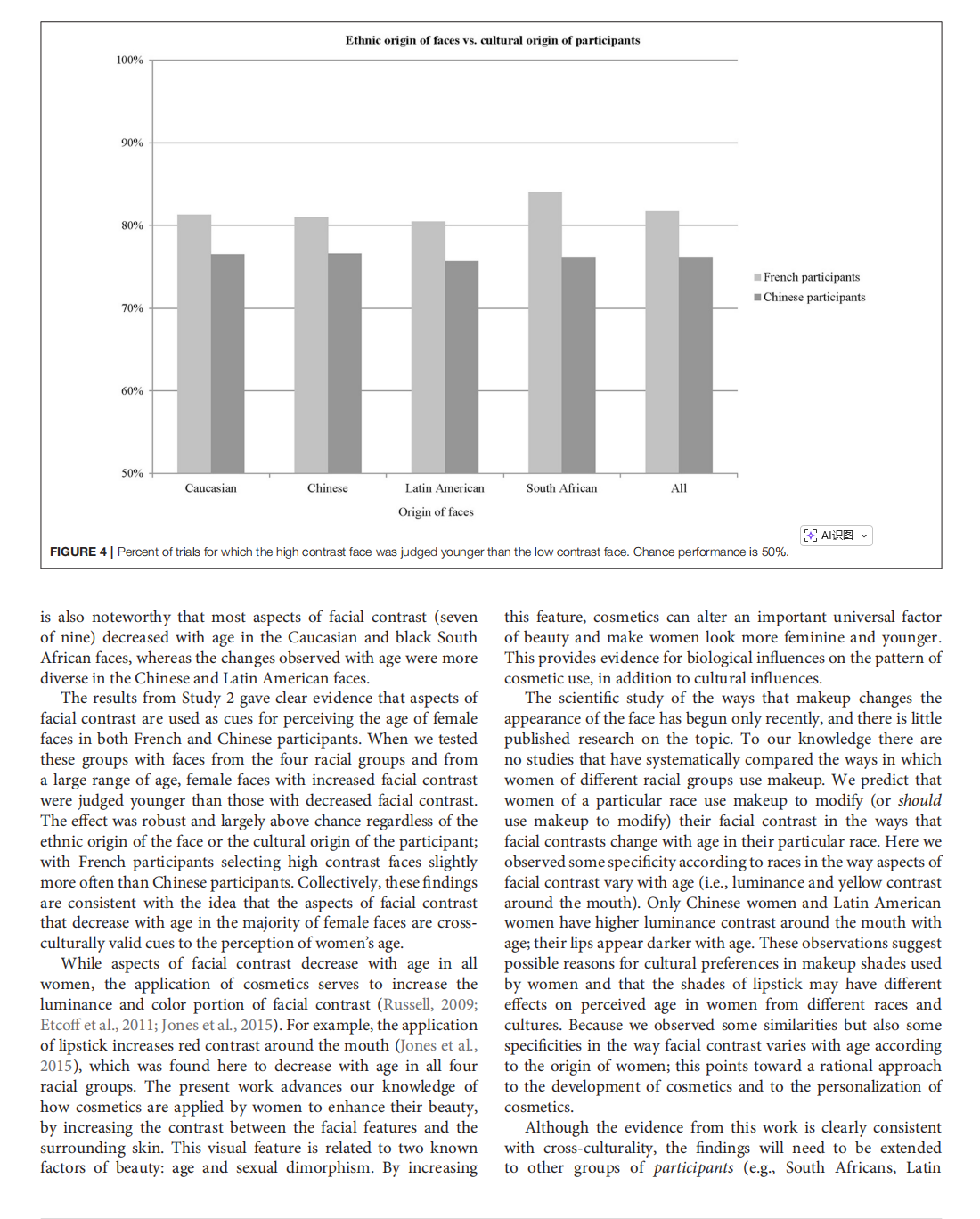

This article is excerpted from the《Frontiers in Psychology》 by Wound World

- 星期五, 31 10月 2025
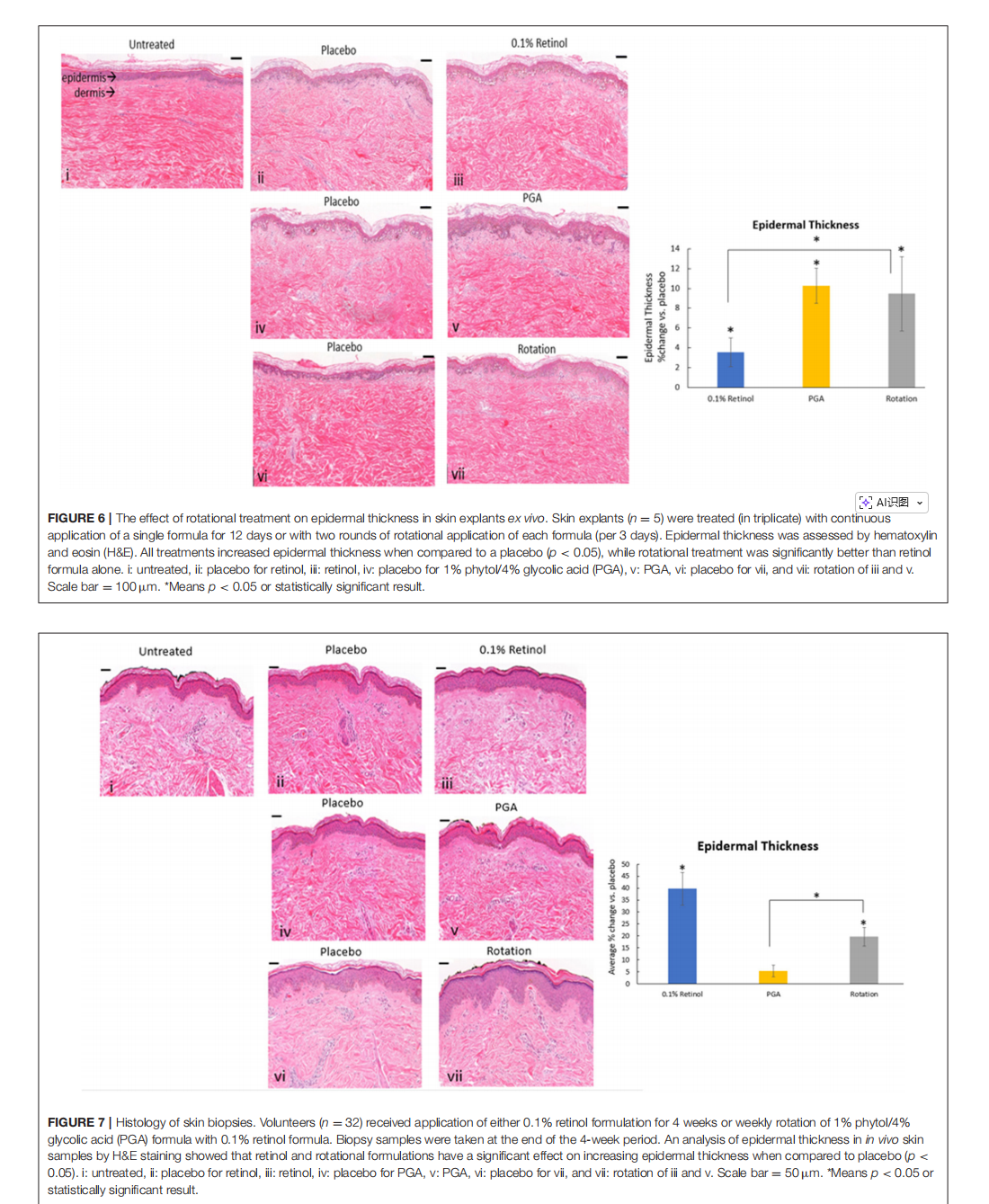
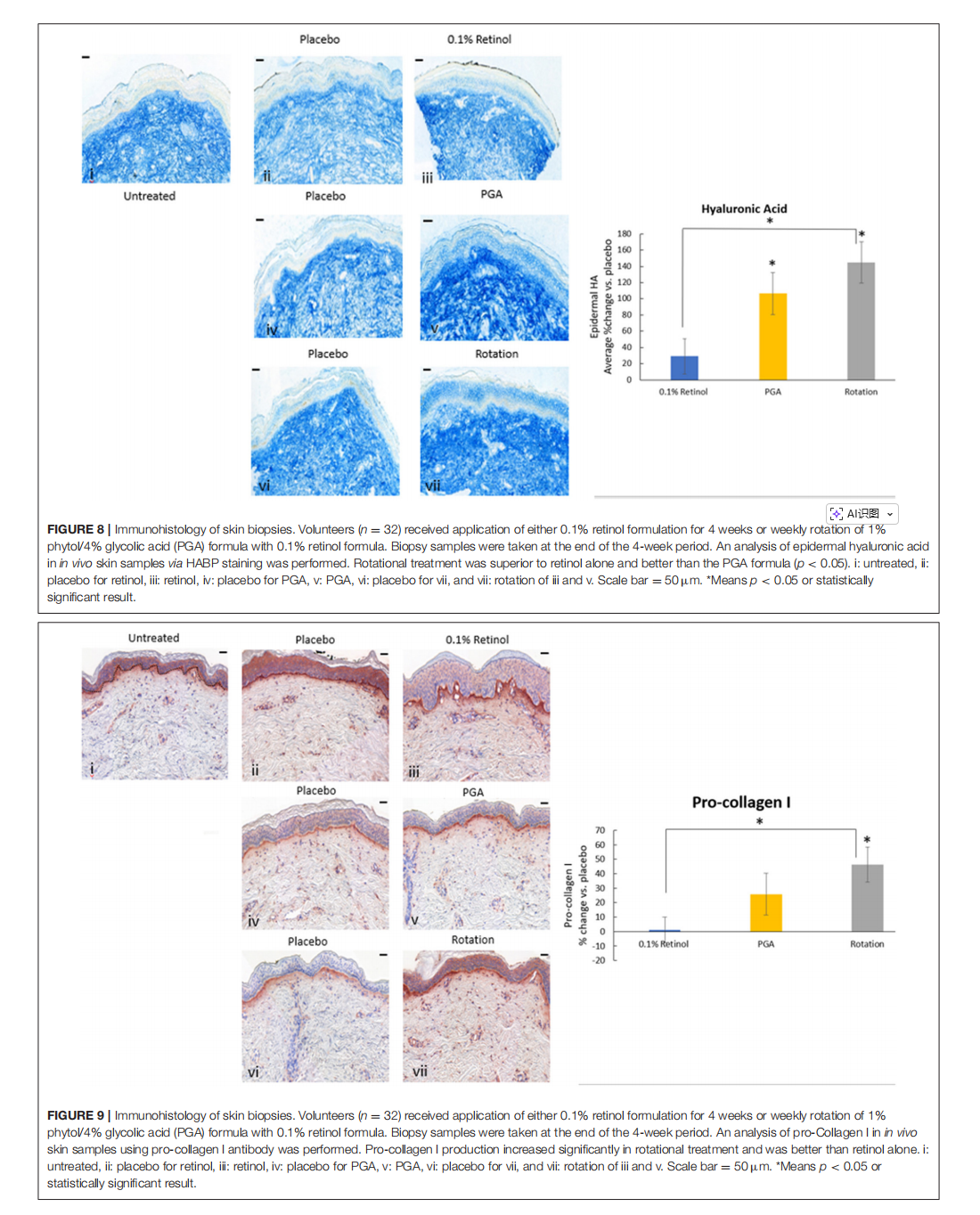
Novel Rotational Combination Regimen of Skin Topicals Improves Facial Photoaging: Efficacy Demonstrated in Double-Blinded Clinical Trials and Laboratory Validation

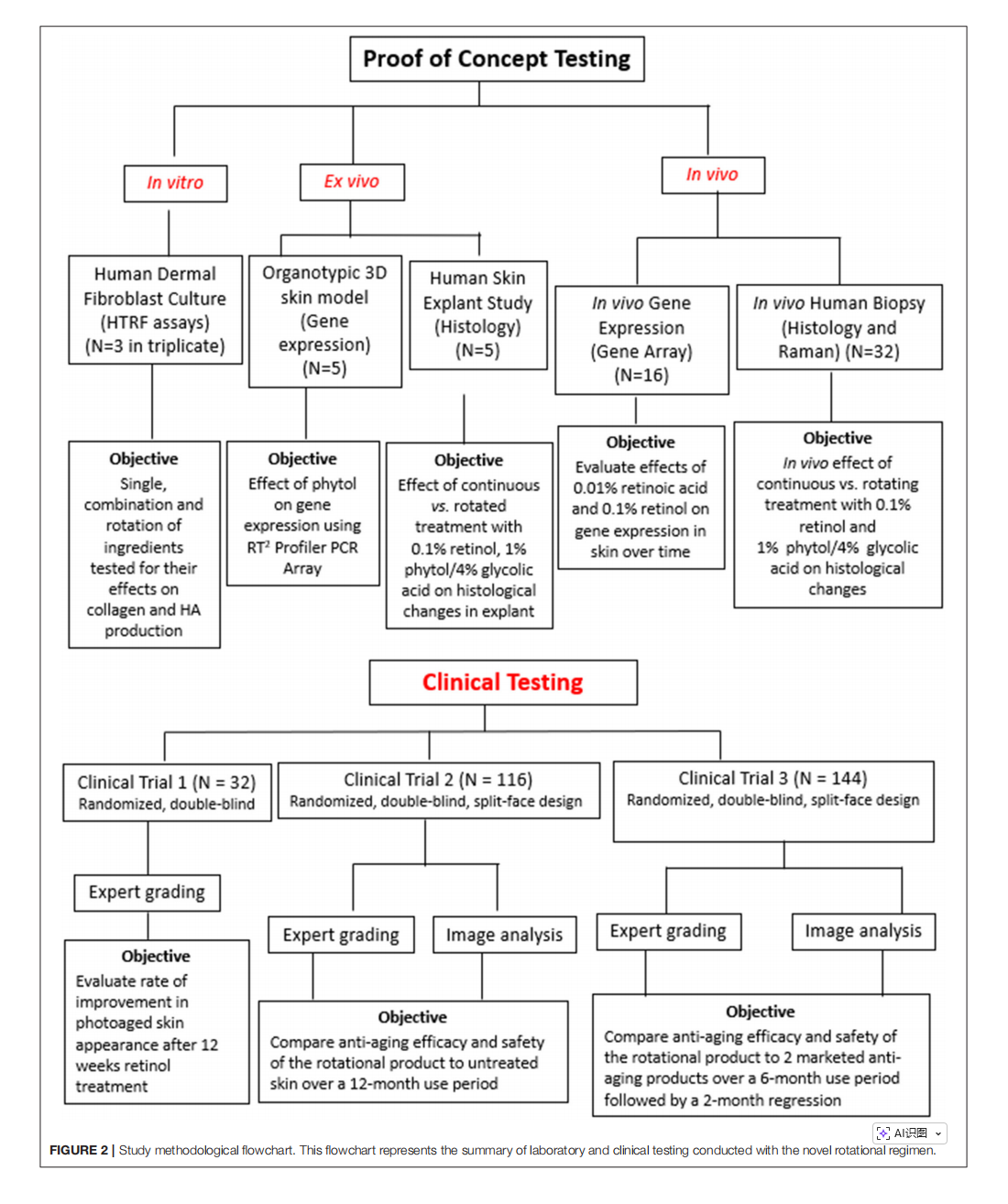
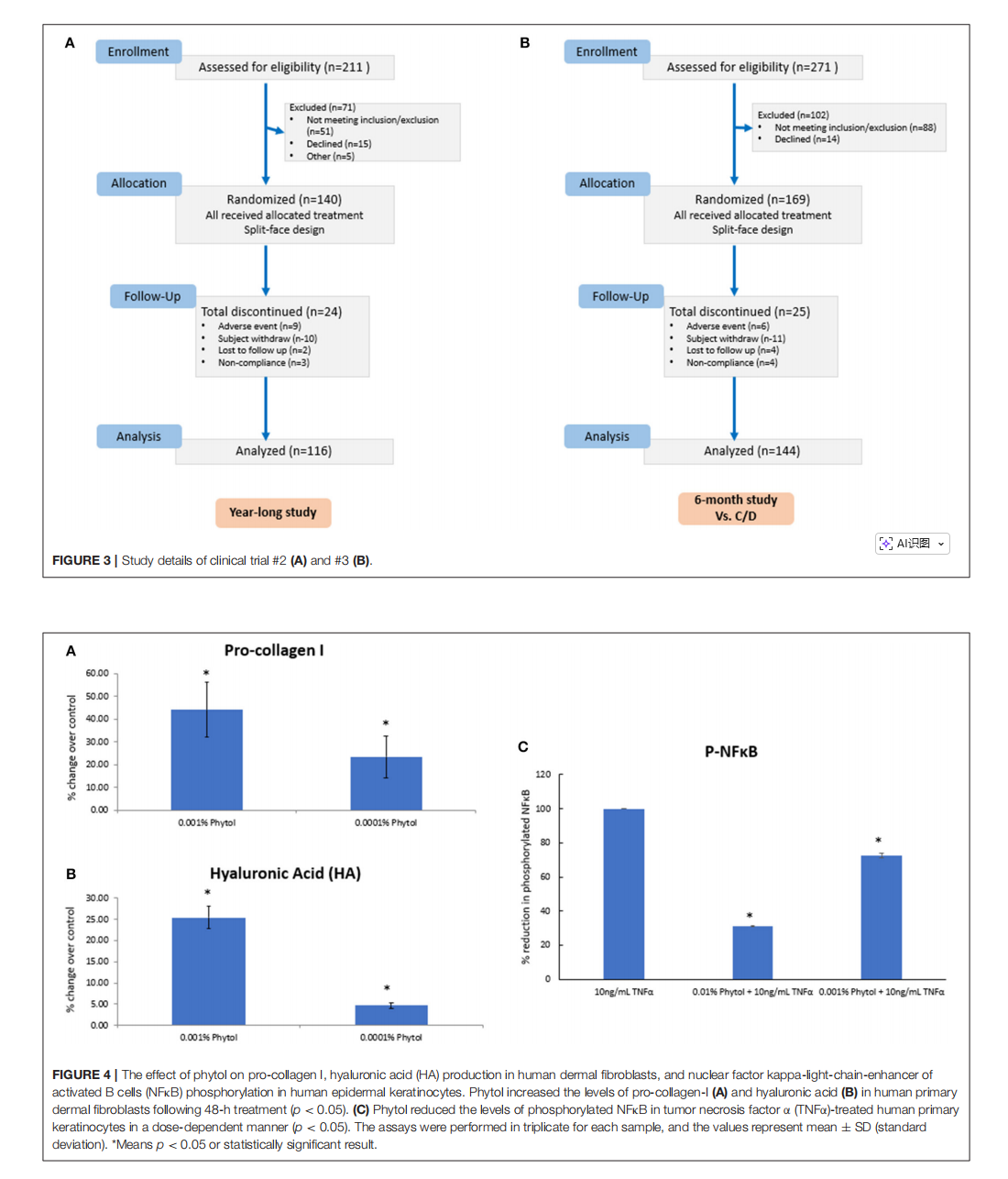

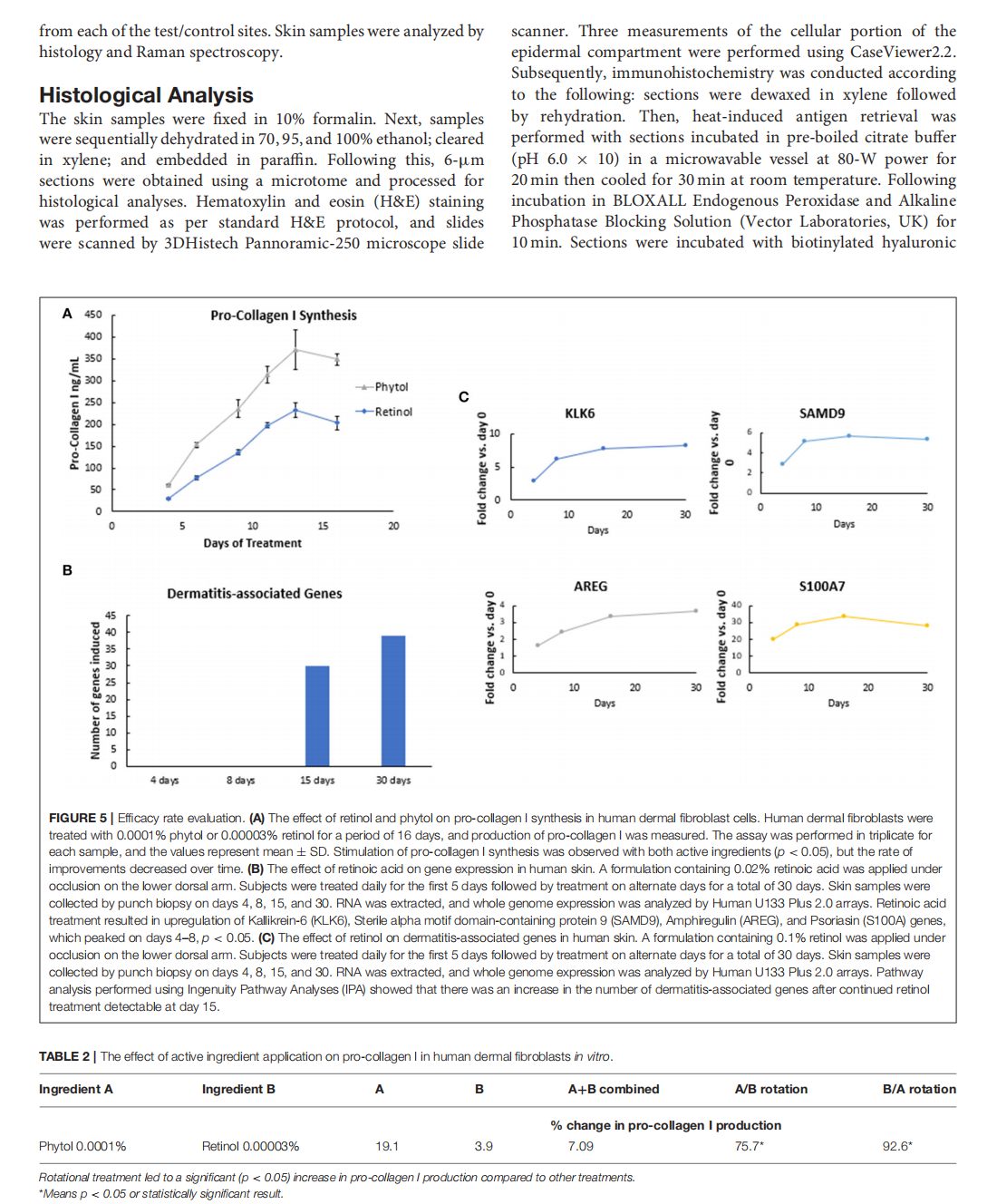
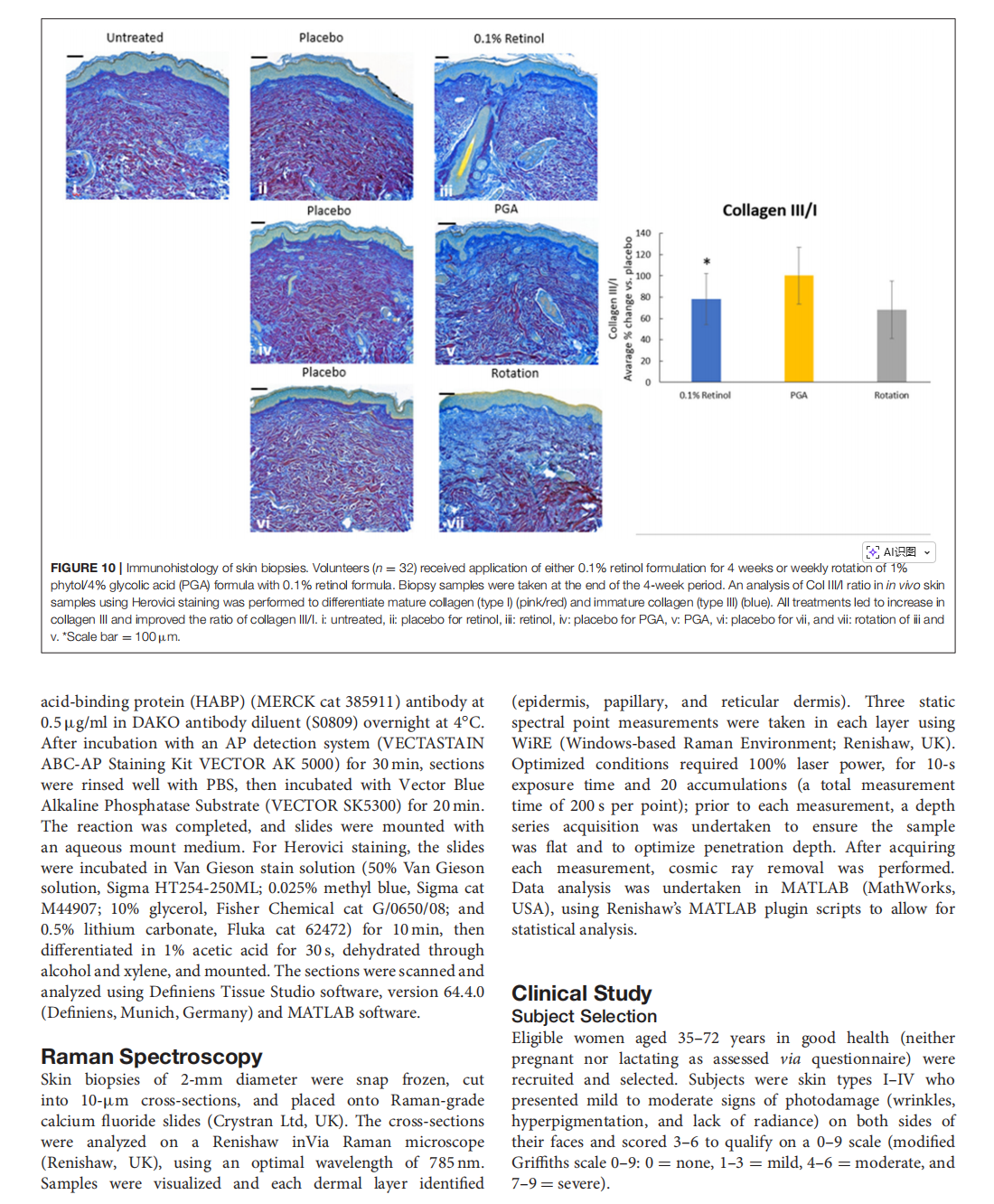
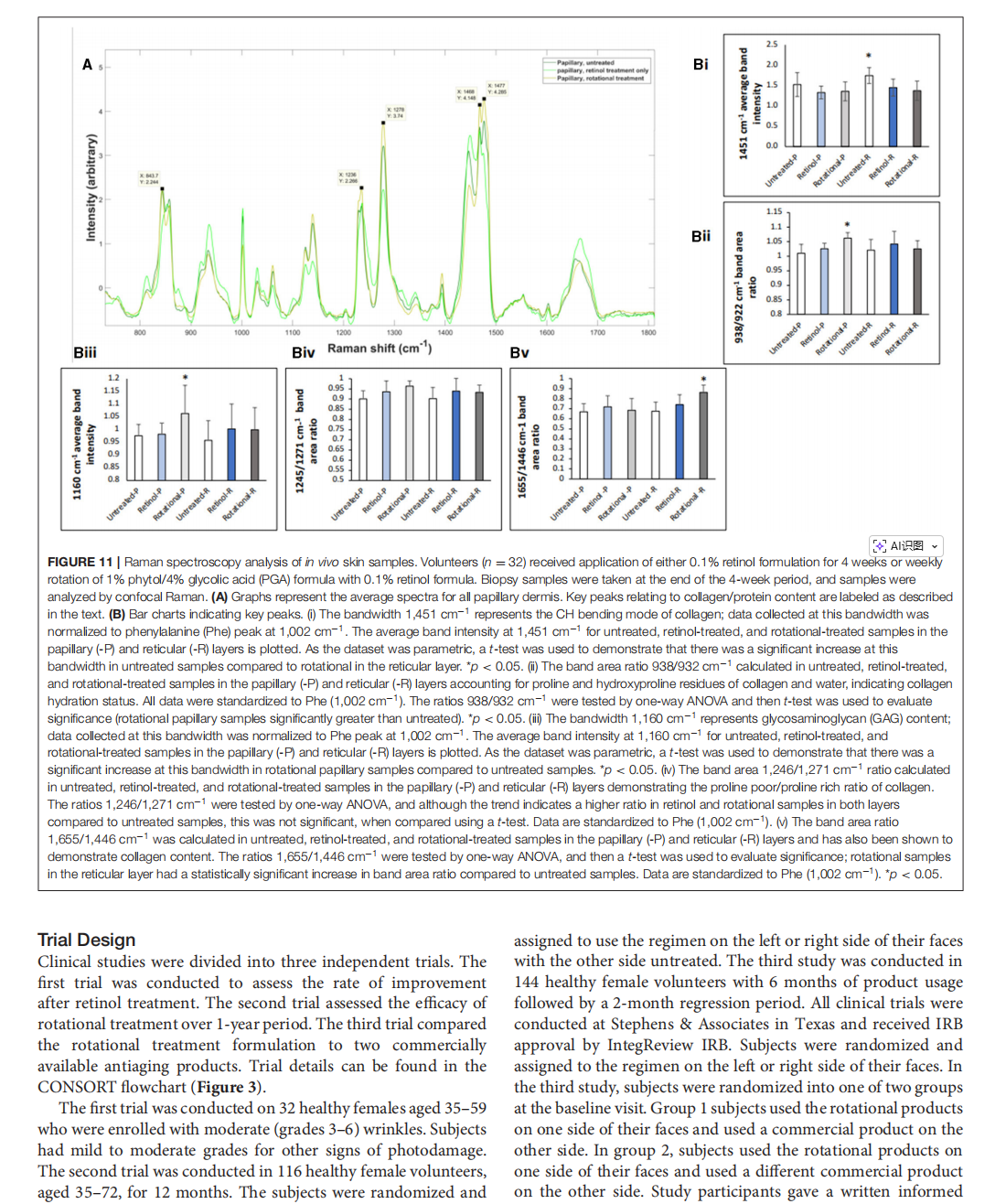
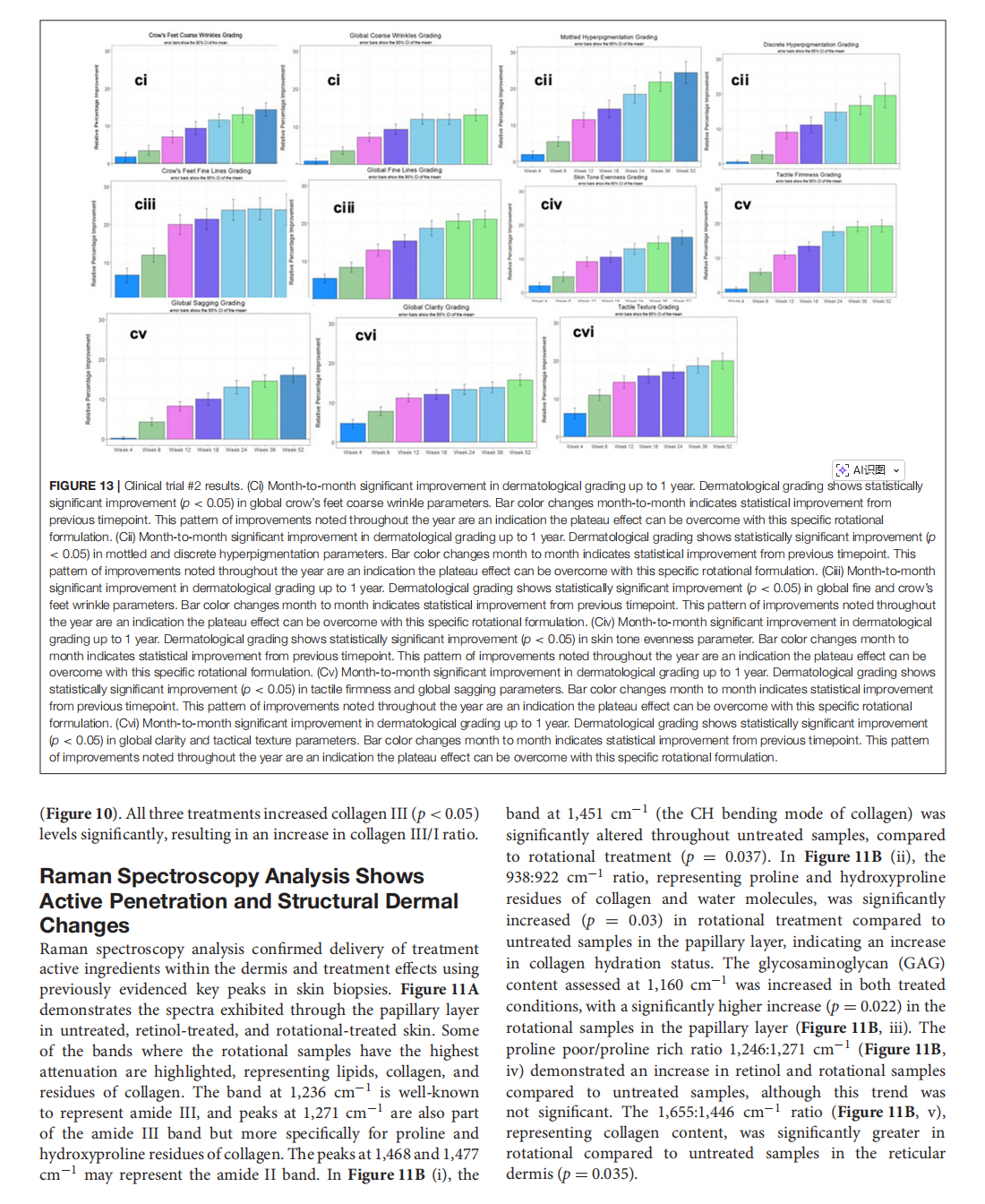
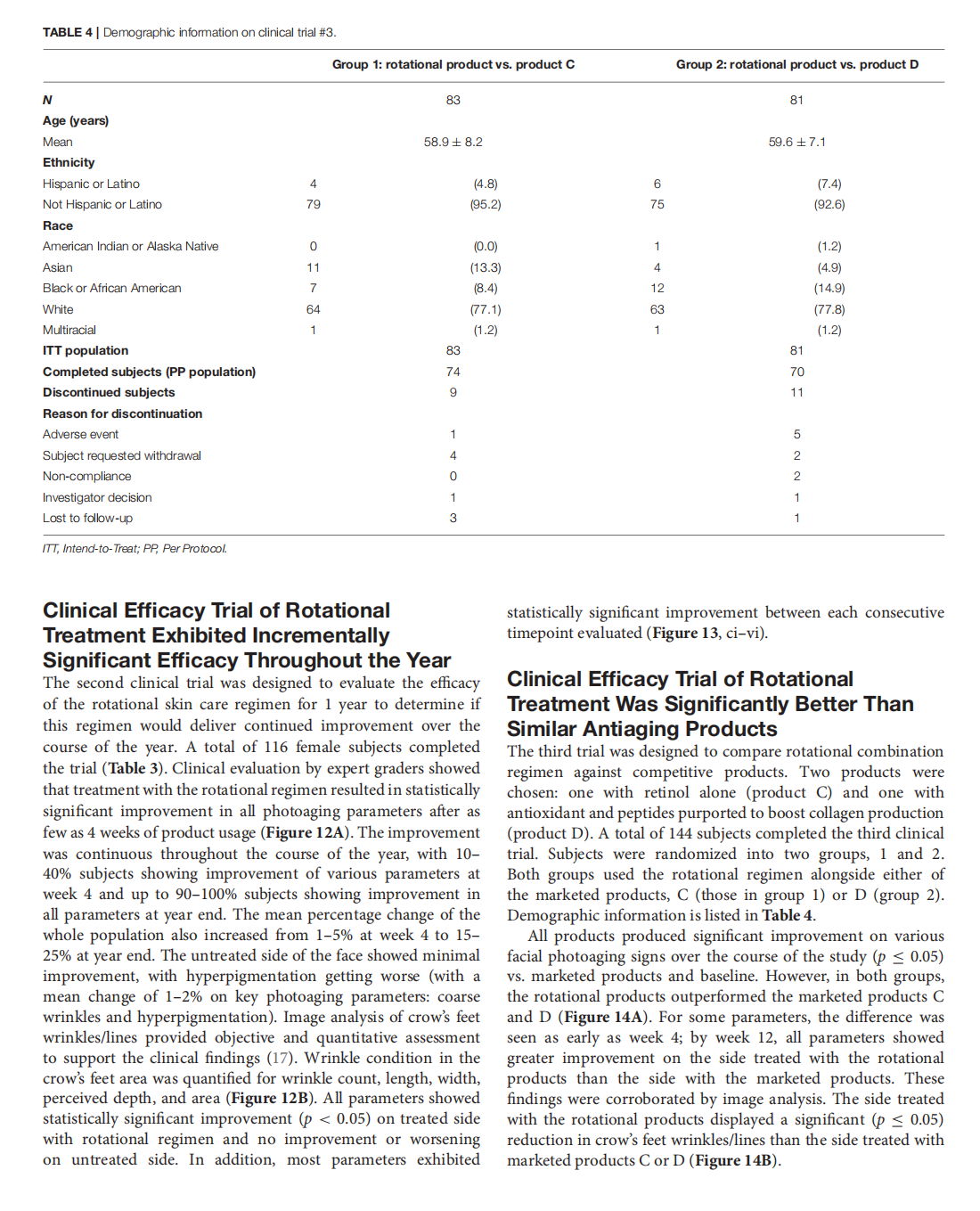
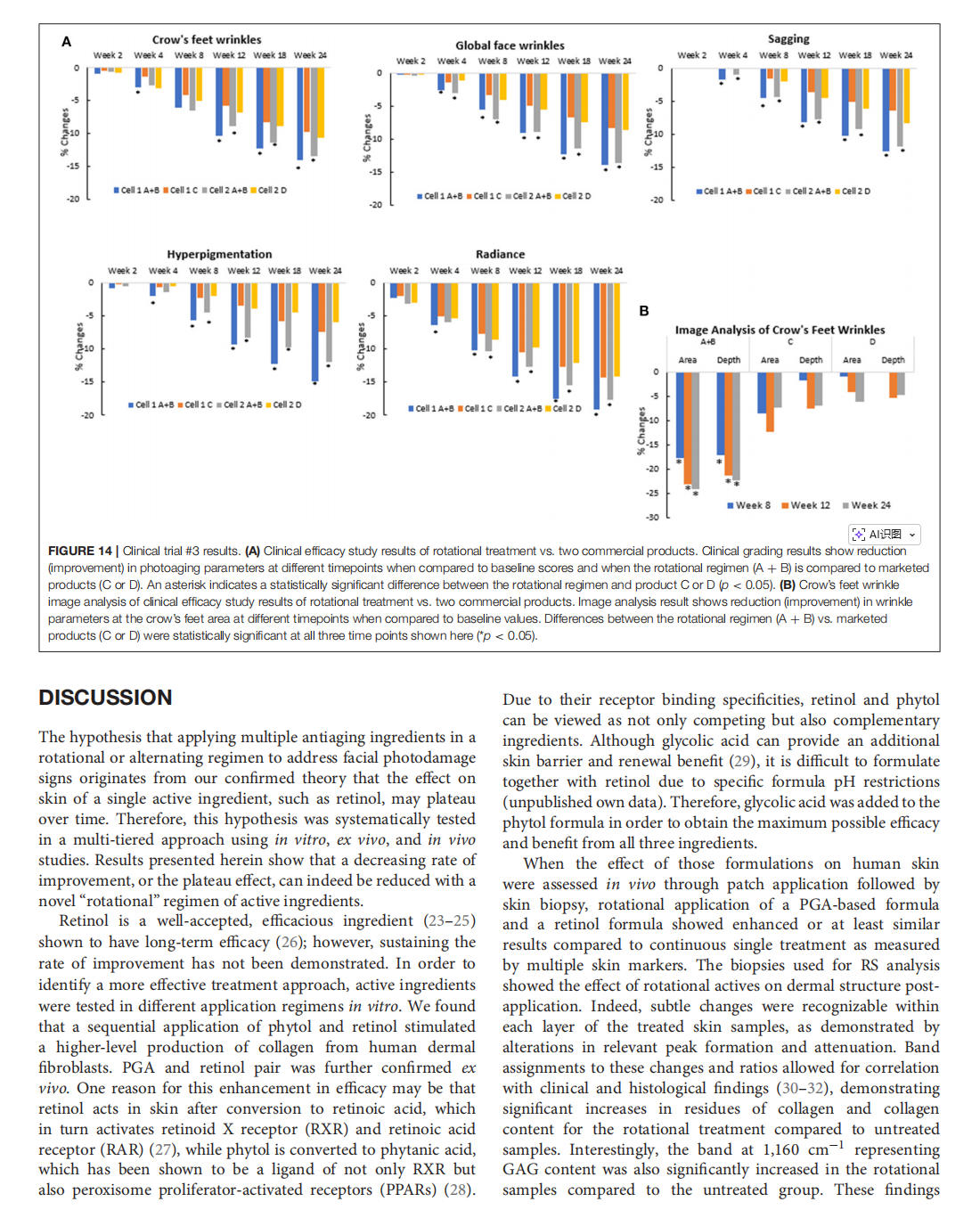
This article is excerpted from the 《Frontiers in Medicine》 by Wound World
- 星期四, 30 10月 2025
Senescent T Cell Induces Brown Adipose Tissue “Whitening” Via Secreting IFN-γ


This article is excerpted from the《Frontiers in Cell and Developmental Biology》 by Wound World

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}