文献精选






This article is excerpted from the 《Frontiers in Endocrinology》 by Wound World








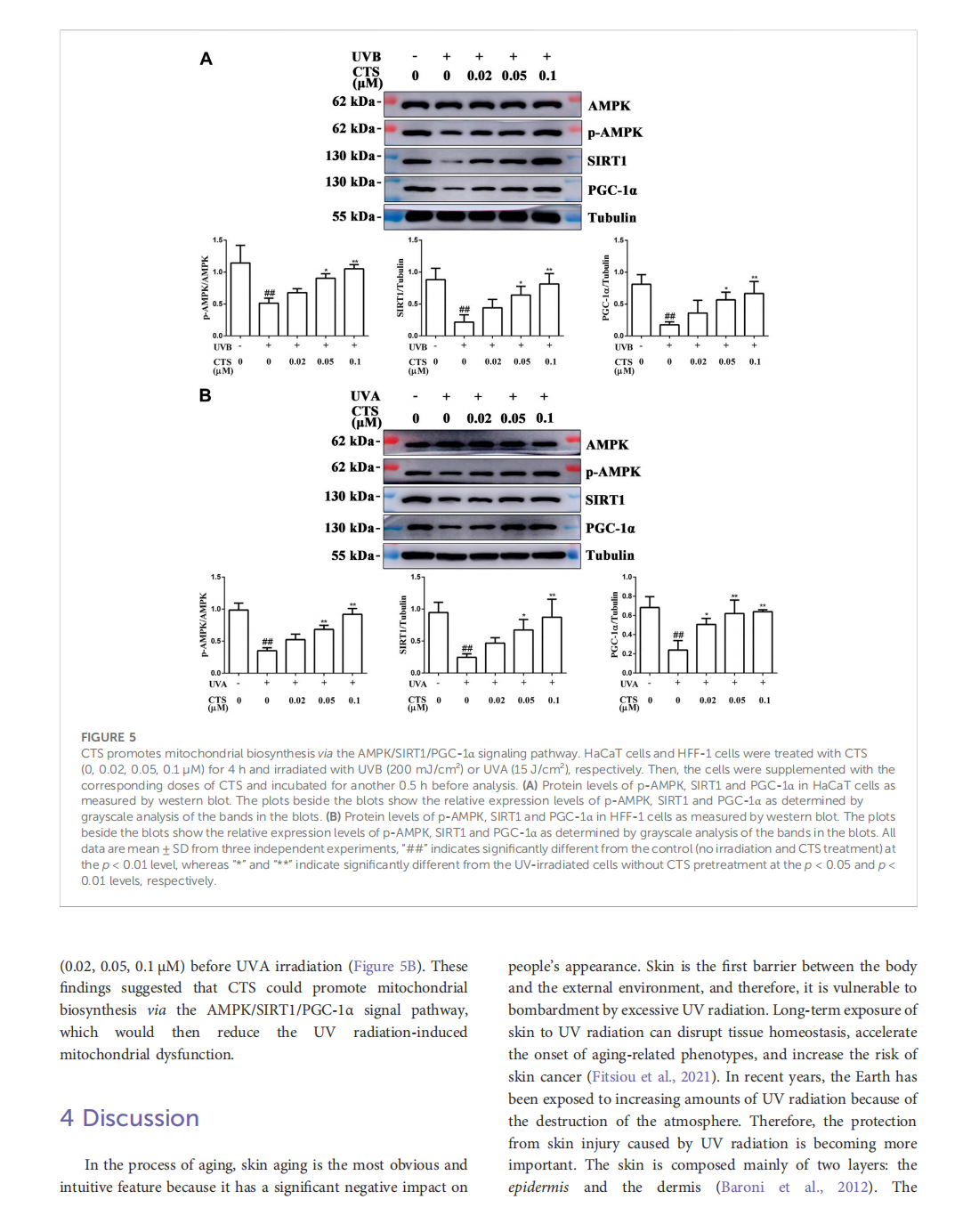
This article is excerpted from the《Frontiers in Pharmacology》 by Wound World







This article is excerpted from the 《Oxidants and Antioxidants in Medical Science》 by Wound World





This article is excerpted from the 《Frontiers in Pharmacology》 by Wound World
