文献精选








This article is excerpted from the《Journal of Toxicology and Environmental Health, Part B》 by Wound World

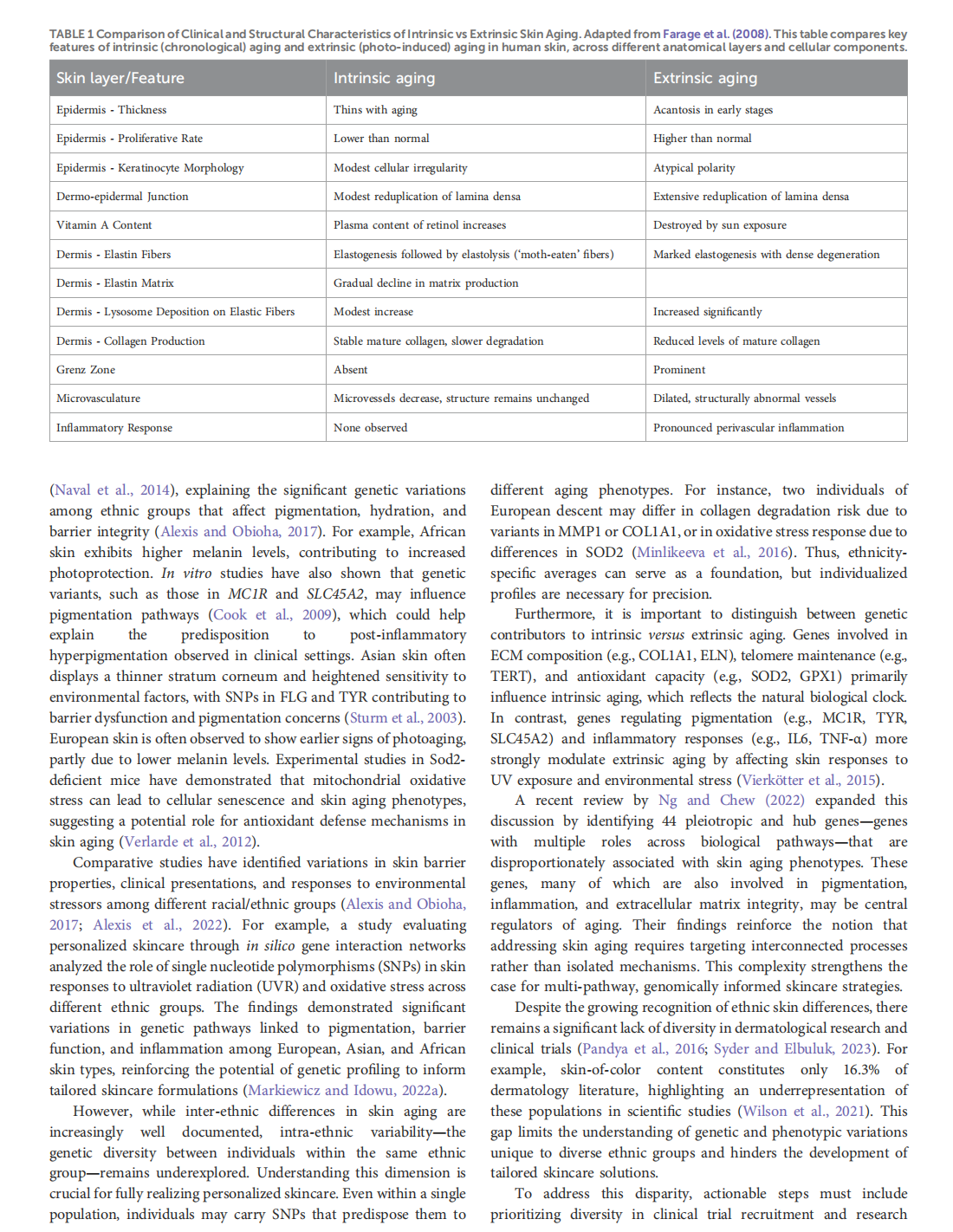



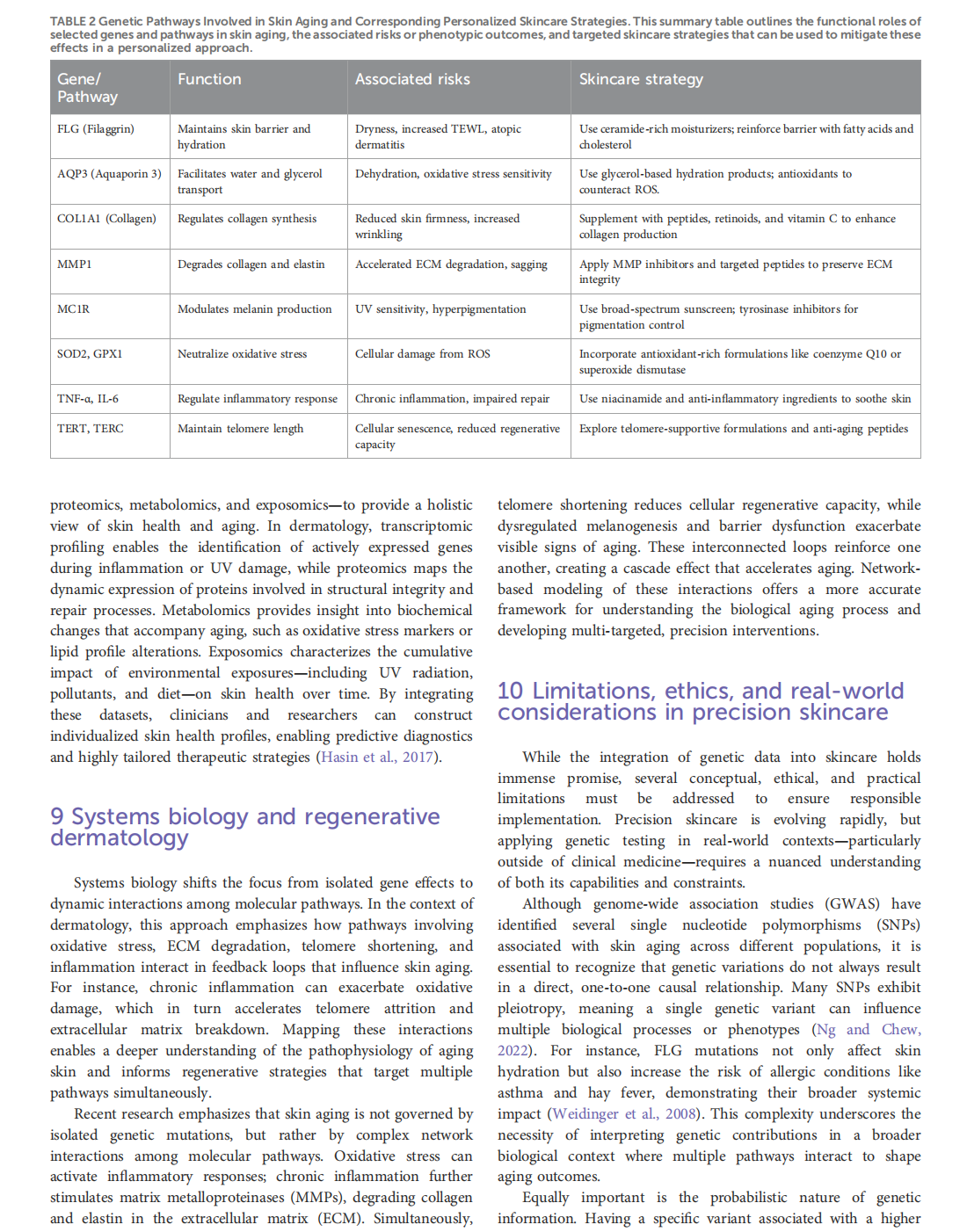


This article is excerpted from the《Frontiers in Genetics》by Wound World



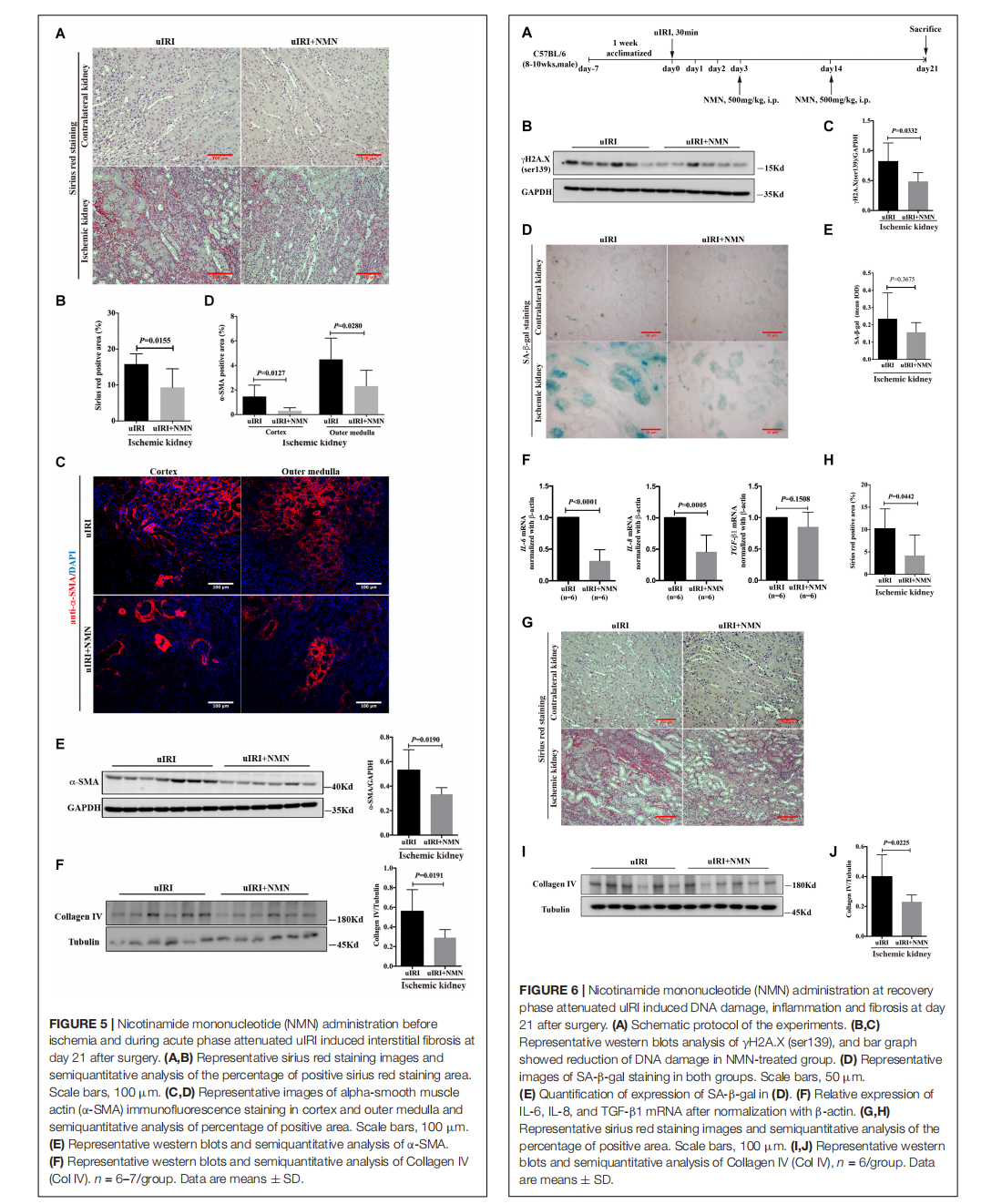

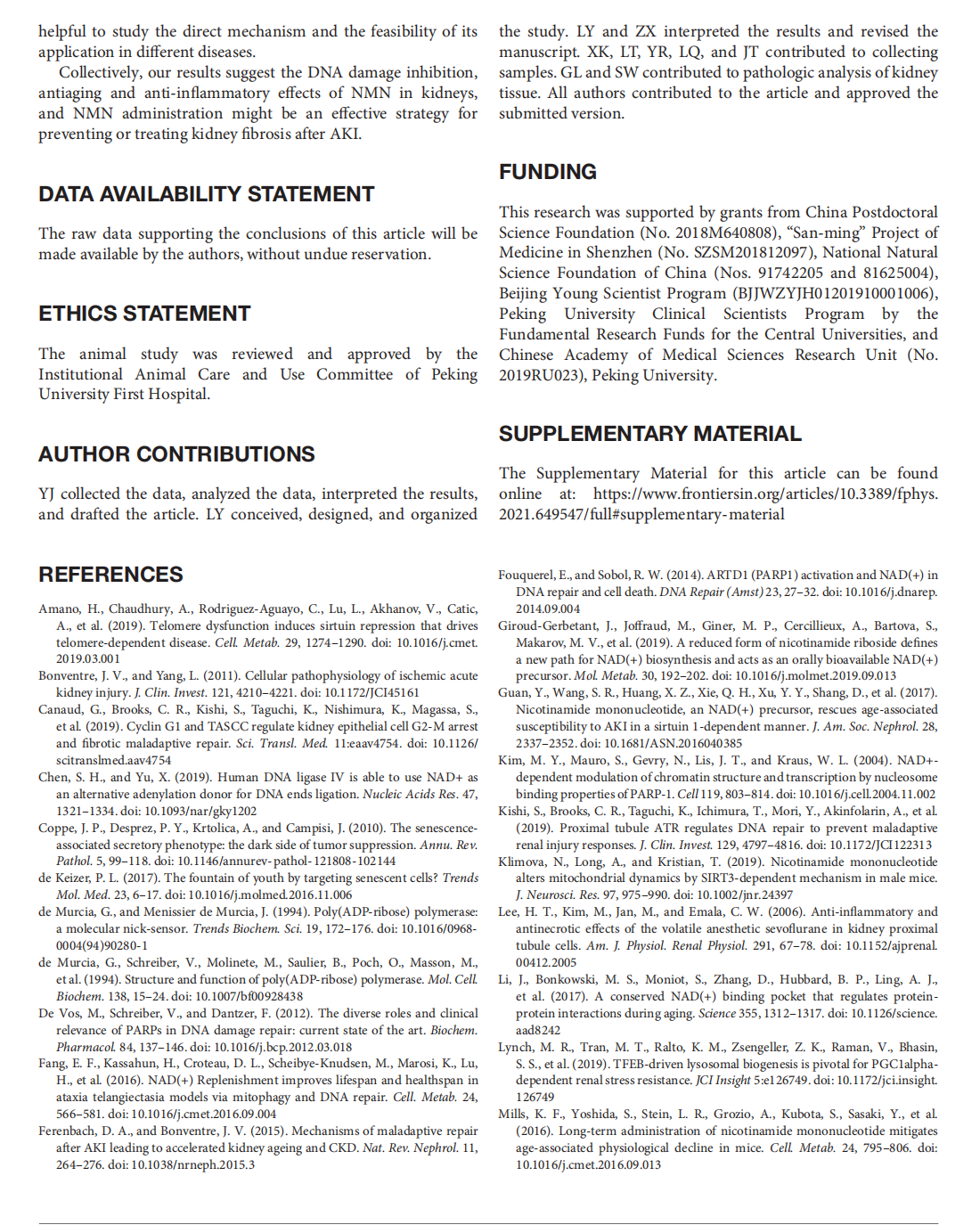
This article is excerpted from the 《Frontiers in Physiology》 by Wound World







This article is excerpted from the 《Frontiers in Physiology》 by Wound World

