
伤口世界
- 星期二, 09 7月 2024
国际糖尿病足工作组:指南的制定和方法学(2023) ———《国际糖尿病足工作组:糖尿病相关的足病预防与管理指南(2023) 》 的一部分)
Standards for the development and methodology of the 2023 International Working Group on the Diabetic Foot
Guidelines :Part of the 2023 IWGDF Guidelines on the prevention and management of diabetes-related foot desease
Sicco A. Bus1,2 ,Matilde Monteiro-Soares3.4.5, Fran Game', Jaap J. van Netten1.2, Jan Apelqvist7 ,Robert Fitidge8 ,
Eric Sennville,Nicolaas C. Schaper0 ,on behalf of the IWGDF Editorial Board
1. Amsterdam UMC, University of Amsterdam, Department of Rehabilitation Medicine,Amsterdam, the Netherlands;
2.Amsterdam Movement Sciences,program Rehabilitation & Development , Amsterdam, the Netherlands;
3. Higher School of Health of the Portuguese Red Cross, Lisbon, Portugal;
4. Department of Community Medicine, Information and Health Decision Sciences ( MEDCIDS),Faculty of Medicine, University of Porto, Porto, Portugal;
5. RISE@ CINTESIS, Faculty of Medicine, Oporto University, Porto, Portugal;
6. Department of Diabetes and Endocrinology ,University Hospitals of Derby and Burton NHS Foundation Trust, Derby, UK;
7. Department of Endocrinology, University Hospital of Malmo, Sweden;
8. Discipline of Surgery, The University of Adelaide and Vascular and Endovascular Service, Royal Adelaide Hospital, Australia;
9. Department of Infectious Diseases ,Gustave Dron Hospital, Tourcoing, France;
10. Division of Endocrinology, MUMC+,CARIM and CAPHRI Institute ,Maastricht, the Netherlands.
朱 虹1 何 洁1 (译) 刘 芳2 (审校)
( 1 . 温州医科大学附属第一医院内分泌科, 浙江 温州 325000;2 . 上海交通大学医学院附属第一医院内分泌代谢科, 上海 200080)
【摘要】 糖尿病相关的足病是造成糖尿病患者经济负担和增加社会成本的主要原因之一。 本指南以主要目标为导向,以循证医学为依据,且在全球得到合理实施。 践行国际糖尿病相关的足病指南对于减轻患者经济负担和社会成本有着重要影响。
国际糖尿病足工作组(IWGDF)从 1999 年起开始发布并随后更新国际指南。 2023 年更新版指南相关推荐均基于推荐、评估、发展和评价分级(GRADE)系统,包括制定相关临床问题和重要结局,完成系统的文献系统综述和荟萃分析,完成评判表汇总,并且给予具体、明确、操作性强的推荐以及理论依据。
本文阐述了《国际糖尿病足工作组:糖尿病相关的足病预防和管理指南(2023 版)》(以下简称为指南)的制定过程。指南由 7 个部分组成,包括预防、糖尿病相关的足溃疡分类、减压、周围动脉病变、感染、创面愈合干预以及活动性夏科神经骨关节病,分别由 7 个独立的国际专家工作组编写。 IWGDF 编辑委员会对 7 个章节进行了整合和简化,形成 IWGDF实践指南。 指南中的每条推荐均经过 IWGDF 编辑委员会成员和相关领域的独立的国际专家审阅通过。 本文是 IWGDF指南的制定和方法学。
我们相信,医务人员、公共卫生机构和政策制定者采用和实施 2023 年 IWGDF 指南,将会改善糖尿病相关的足病的预防和管理水平,从而减少全球该疾病患者和减轻该疾病引起的全球社会负担。
【关键词】 指南; 糖尿病; 糖尿病相关的足病; 方法学; 国际糖尿病足工作组
www.iwgdfguidelines.org
中图分类号:R587.2;R-01
文献标识码:C
- 星期一, 08 7月 2024
A new framework for the diagnosis, staging and management of obesity in adults
Luca Busetto, Dror Dicker, Gema Frühbeck, Jason C. G. Halford, Paolo Sbraccia, Volkan Yumuk & Gijs H. Goossens
The European Association for the Study of Obesity presents a new framework for the diagnosis, staging and management of obesity in adults to better align with the concept of obesity as an adiposity-based chronic disease.
Obesity is a multifactorial, chronic, relapsing, non-communicable disease marked by an abnormal and/or excessive accumulation of body fat that presents a risk to health. It is well established that obesity acts as a gateway to a range of other non-communicable and communicable diseases1–3 .
Despite this wide recognition of obesity as a chronic disease, the clinical recommendations that guide the diagnosis of obesity and its management have not been aligned sufficiently with the clinical processes normally adopted for other chronic diseases. In many settings, the diagnosis of obesity is still based solely on body mass index (BMI) cut-off values, and does not reflect the role of adipose tissue distribution and function in the severity of the disease1 . Moreover, the indications for using the different therapeutic approaches now available for obesity management remain mostly based on anthropometric measurements, rather than on a more complete clinical evaluation of the individual4 . This is in sharp contrast with other chronic diseases, for which clear therapeutic indications are described, targets are set, and the choice of the type and intensity of treatment is based on the probability of reaching the treatment target, with adequate and prompt treatment intensification when the target is not reached.
To stimulate the development and implementation of clinical guidelines for obesity that are more aligned with those already in place for other chronic diseases, the European Association for the Study of Obesity (EASO) initiated and conducted a consensus process to propose a new framework for the diagnosis, staging and management of obesity in adults.
Consensus process
We performed a modified Delphi study5,6 to identify a set of statements that can aid in the diagnosis, staging and management of obesity according to a framework that is more adherent to the concept of obesity as an adiposity-based chronic disease (ABCD)1 . A steering committee identified by the EASO, consisting of the authors of this paper, discussed and prepared an initial set of statements used for a voting process by a group of experts. Voting was performed on a five-point scale, as follows: (1) strongly disagree; (2) disagree; (3) neither agree nor disagree; (4) agree; and (5) strongly agree. In each round of voting, experts were also asked to provide comments to explain their voting score, and responses were anonymized. The steering committee evaluated the voting and comments received at each round and generated a modified set of statements for the subsequent round of voting. Consensus was defined as ≥75% of expert agreement on a statement (score ≥4).
The steering committee retained responsibility for the selection of experts involved in the process. Selection was based on international reputation and known expertise in obesity science and management.
In total, 29 experts were contacted, and all agreed to participate in the present study. Most of the experts belong to the endocrinology, nutrition or internal medicine fields (72%), but the group also included five bariatric surgeons, two primary care physicians and one expert on patient advocacy. A standard conflict of interest form was completed by each participant before the start of the Delphi process. This study was performed by the EASO without any external funding, and approval by the ethics committee was not required.
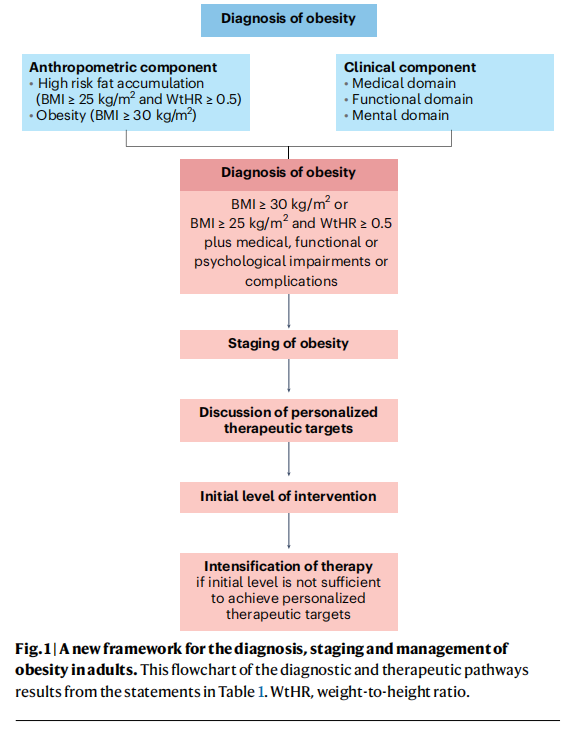
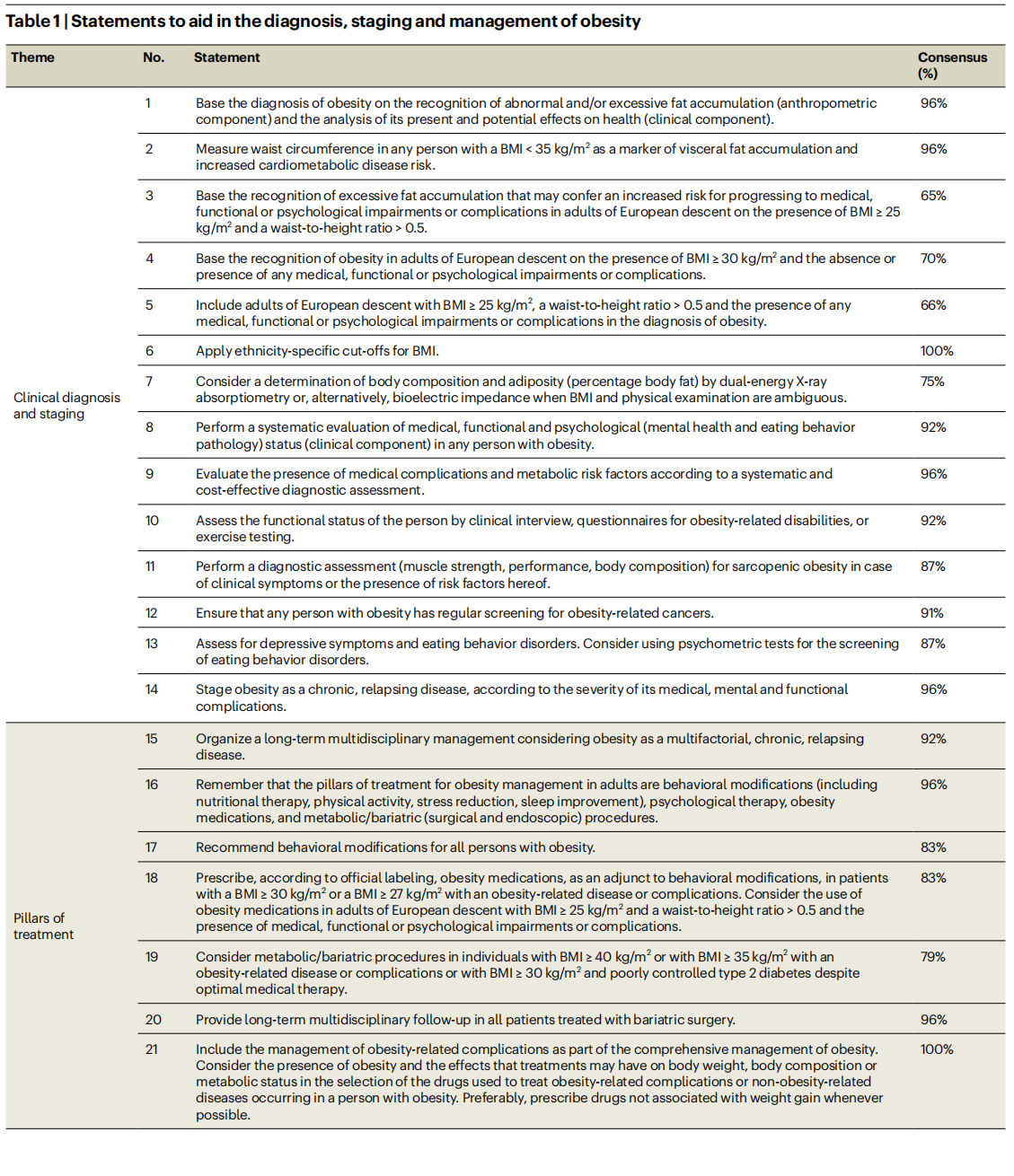
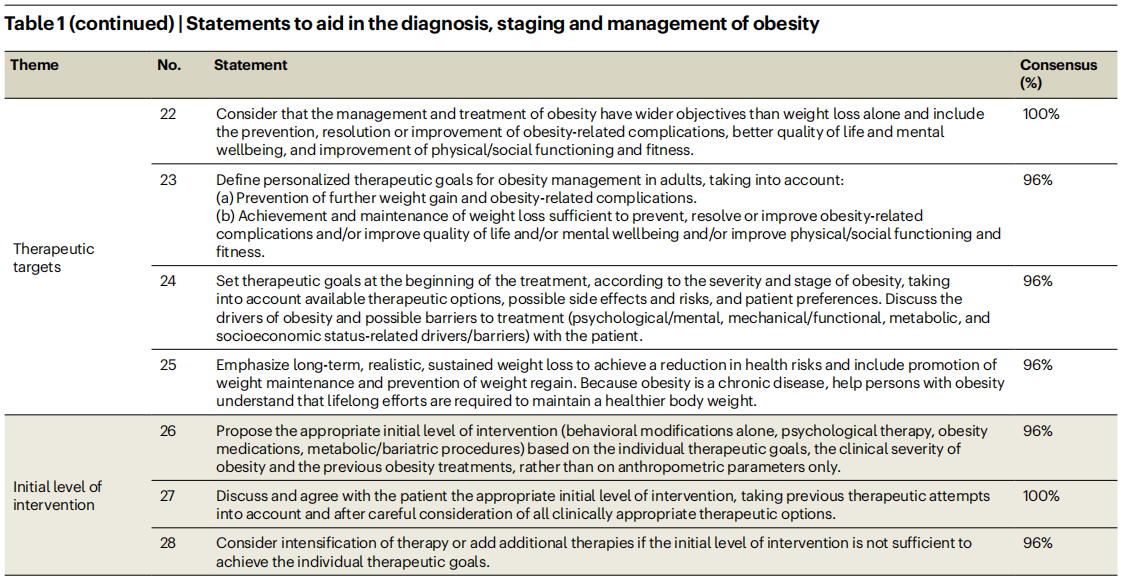
The study comprised three Delphi rounds. In the first round, 25 experts (86%) voted and commented on 30 original statements that were prepared by the steering committee. A total of 21 statements (70%) received consensus. The steering committee evaluated voting and comments and generated a second set of 28 statements submitted for a second Delphi round. In the second round, 24 experts (83%) voted and commented on the statements. A total of 24 statements (86%) received consensus. The steering committee discussed the comments received for the four non-consented statements, reconsidered the formulations of these statements, and submitted the four revised statements for the final Delphi round. In the third round, 24 experts (83%) voted and provided final comments related to the four revised statements. One of these four statements (statement 12) reached full consensus, whereas most experts approved the other three revised statements (statements 3–5), with only a few experts providing a score <3 (that is, strongly disagree or disagree). The steering committee performed a final revision and decided to approve a list of 28 statements, covering clinical diagnosis and staging of obesity, pillars of treatment, therapeutic targets, and initial level of intervention. The final list of statements and final percentages of approval by the experts is shown in Table 1. A flowchart of the diagnostic and therapeutic pathways resulting from the statements is presented in Fig. 1.
A chronic progressive disease
The recognition of obesity as a complex chronic non-communicable disease should inform the development of evidence-based guidelines for the diagnosis and management of obesity. We anticipate that, in conjunction with other ongoing initiatives7 , this Delphi process will contribute to improving obesity management in adults living with obesity.
Based on current clinical evidence, the diagnosis of obesity should not be based solely on the presence of an abnormal and/or excessive fat accumulation (anthropometric component). The diagnosis of obesity should instead include a careful analysis of the present and potential effects that dysfunctional and/or excessive fat accumulation may have on health (clinical component) (statement 1). This statement aligns with what has been suggested by other recent guidelines on obesity management8,9 . Moreover, this statement fully adheres to the concept that obesity should be considered a chronic progressive disease process that may transit from a relatively asymptomatic state to a phase in which abnormal and/or excessive fat accumulation is accompanied by health impairments, and finally to a life-threatening or disabling condition10.
Abdominal fat accumulation
An important novelty of our framework regards the anthropometric component of the diagnosis. The basis for this change is the recognition that BMI alone is insufficient as a diagnostic criterion, and that body fat distribution has a substantial effect on health. More specifically, the accumulation of abdominal fat is associated with an increased risk of developing cardiometabolic complications and is a stronger determinant of disease development than BMI, even in individuals with a BMI level below the standard cut-off values for obesity diagnosis11. This is reflected by two important statements. First, we make explicit that abdominal (visceral) fat accumulation is an important risk factor for health deterioration, also in people with low BMI and still free of overt clinical manifestations (statement 3). Second, the new framework includes people with lower BMI (≥25–30kg/m2 ) but increased abdominal fat accumulation and the presence of any medical, functional or psychological impairments of complications in the definition of obesity, hence reducing the risk of undertreatment in this particular group of patients in comparison to the current BMI-based definition of obesity (statement 4). The choice of introducing waist-to-height ratio, instead of waist circumference, in the diagnostic process is due to its superiority as a cardiometabolic disease risk marker12.
Diagnostics and staging
The clinical component of the diagnosis should include a systematic evaluation of medical, functional and psychological (such as mental health and eating behavior pathology) impairments in any person with obesity, as also suggested in other guidelines8,9 . A detailed description of the clinical aspects and methodologies that need to be included in this systemic clinical evaluation was beyond the scope of this exercise. For the medical evaluation (statement 9), several documents are available to provide guidance4,8 . For the functional and psychological evaluation, examination may be performed using an array of methods, ranging from easy-to-perform tests that are applicable in the primary care setting to more sophisticated tests, which may be reserved for specialized centers (statements 10 and 13). Considering the emerging problem of obesity in older individuals, statement 11 was included to emphasize the importance of performing a diagnostic assessment (muscle strength, performance and body composition) for sarcopenic obesity13. Finally, considering the strong association between obesity and several types of cancer, a statement calling for regular screening for obesity-related cancers in any person with obesity was included (statement 12).
Clinical staging processes are frequently used to evaluate and describe an individual’s health status and the progression of chronic diseases. Clinical staging usually expresses the severity of a disease in a simplified, condensed and standardized way. This has prognostic implications, and it may guide or mandate therapeutic interventions. In our Delphi process, the experts agreed on the importance of staging obesity as a chronic, relapsing disease, according to the severity of its clinical manifestations and complications (statement 14), as proposed by previous guidelines9 .
Obesity management
Considering the pillars of treatment of people with obesity (statements 15–21), our recommendations substantially adhere to current available guidelines4,8,9 . Behavioral modifications, including nutritional therapy, physical activity, stress reduction and sleep improvement, were agreed as main cornerstones of obesity management, with the possible addition of psychological therapy, obesity medications and metabolic or bariatric (surgical and endoscopic) procedures. For the latter two options, the steering committee discussed the fact that current guidelines are based on clinical evidence derived from clinical trials, in which inclusion criteria were mostly based on anthropometric cut-off values rather than on a complete clinical evaluation4,8,9,14. In current practice, the strict application of these evidence-based criteria precludes the use of obesity medications or metabolic/bariatric procedures in patients with a substantial burden of obesity disease, but low BMI values. Therefore, members of the steering committee proposed, and experts subsequently agreed (79%), that, in particular, the use of obesity medications should be considered in patients with BMI ≥ 25 kg/m2 and a waist-to-height ratio > 0.5 and the presence of medical, functional or psychological impairments or complications, independently from current BMI cut-off values (statement 18). This statement may also be seen as a call to pharmacological companies and regulatory authorities to use inclusion criteria that are more adherent to the clinical staging of obesity and less to traditional BMI cut-offs when designing future clinical trials with obesity medications15.
Full agreement among the experts was reached for the statement that the management of obesity should move beyond weight loss alone, and should include the prevention, resolution or improvement of obesity-related complications, a better quality of life and mental wellbeing, and improvement of physical and social functioning and fitness (statement 22). This statement will move obesity management closer to the management of other non-communicable chronic diseases, in which the goal is not represented by short-term intermediate outcomes, but by long-term health benefits. Defining long-term personalized therapeutic goals should inform the discussion with the patients from the beginning of the treatment, considering the stage and severity of the disease, the available therapeutic options and possible concomitant side effects and risks, patient preferences, individual drivers of obesity and possible barriers to treatment (statements 23 and 24). Emphasis on the need for a long-term or life-long comprehensive treatment plan rather than short-term body weight reduction is warranted.
The concept of obesity as a chronic disease and the discussion of therapeutic targets should also inform the choice of the initial level of intervention and eventual intensification of therapy (statements 26–28), avoiding the same repetitive and futile cycles of intervention that are not effective enough to achieve patient benefit, and preventing therapeutic inertia16.
This Delphi process represents the current vision of the EASO on the diagnosis, staging and management of obesity as a complex, relapsing, non-communicable chronic disease in adults. We anticipate that the recommendations outlined in this paper, in conjunction with other ongoing international initiatives7 , will contribute to improved obesity management strategies that are more consistent with treatment algorithms already applied for other non-communicable chronic diseases. Moreover, this framework may aid scientific advancements and the development of new clinical practice guidelines.
Luca Busetto1 , Dror Dicker2 , Gema Frühbeck 3 , Jason C. G. Halford4 , Paolo Sbraccia5 , Volkan Yumuk6 & Gijs H. Goossens 7
1 Department of Medicine, University of Padova, Padova, Italy.
2 Internal Medicine Department and Obesity Clinic, Hasharon Hospital-Rabin Medical Center, Petach-Tikva, Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel.
3 Department of Endocrinology and Nutrition, Clínica Universidad de Navarra, CIBEROBN, IdiSNA, Pamplona, Spain.
4 School of Psychology, University of Leeds, Leeds,UK.
5 Department of Systems Medicine, University of Rome Tor Vergata, Rome, Italy.
6 Division of Endocrinology, Metabolism and Diabetes, Department of Internal Medicine, Cerrahpasa Faculty of Medicine, Istanbul University-Cerrahpasa, Istanbul, Turkey.
7 Department of Human Biology, Institute of Nutrition and Translational Research in Metabolism (NUTRIM), Maastricht University Medical Center⁺, Maastricht, The Netherlands.
e-mail: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。
Published online: 05 July 2024
References
1. Fruhbeck, G. et al Obes. Facts12, 131-136 (2019).
2. Dicker, D. et al. Obes. Facts 13, 430- -438 (2020).
3. Burki, T. Lancet Diabetes Endocrinol.9, 418 (2021).
4. Yumuk, V. et aL Obes. Facts 8, 402- -424 (2015).
5. Clayton, M. J. Educ. Psychol. 17, 373- -386 (1997).
6. Hasson, F., Keeney, S. & McKenna, H. J. Adv. Nurs.32, 1008- 1015 (2000).
7. Rubino, F. et aL Lancet Diabetes EndocrinoLl. 11, 226- 228 (2023).
8. Garvey, W. T. et al Endocr. Pract. 22, 1-203 (2016).
9. Wharton, S. et aL CMAJ192, E875-E891 (2020).
10. Bray, G. A.,. Kim, K. K., Wilding, J P. H. & on behalf of World Obesity Federation. Obes. Rev. 18, 715-723 (2017).
11. Goossens, G. H. Obes. Facts 10, 207 -215 (2017).
12. Ashwell, M.. Gunn, P. & Gibson, S. Obes. Rev. 13, 275- -286 (2012).
13. Donini, L. M. et al. Obes. Facts.15, 321-335 (2022).
14. Di Lorenzo, N. et al Surg. Endosc.34, 2332- -2358 (2020).
15. Agarwal, A. A., Narayan, A. & Stanford, F. C. JAMA Intern. Med. 184, 341-342 (2024).
16. Busetto, L, Sbraccia, P. & Vettor, R. Eat Weight Disord. 27, 761-768 (2022).
List of experts
The Steering Commitee identifed by EASO for this project, consisting of the authors of this paper, takes full responsibility for the contents of this Comment. The below specialists participated in the voting process of the Delphi methodology, but not in interpretation of the results or writing of the Comment, and agreed to be mentioned here: M. Agarwal, R. Barazzoni, T. Comuzzie, M. De Luca, N. Di Lorenzo, D. Durrer-Schutz, T. Garvey, C. Hughes, L. Kaplan, C. LeRoux, J. Mechanick, N. Montano, Jean-M. Oppert, R. Peterli, K. Pietilainen, G. Prager, X. Ramos-Salas, D. Ryan, M. Ryden, A. Sharma, and E. van Rossum.
Competing interests
L.B. received personal funding from Novo Nordisk, Boehringer Ingetheim, Eli Lilly, Pfizer, Bruno Farmaceutici as a member of advisory boards, and from Rythms Pharmaceuticals and Pronokal as a speaker. D.D. received personal funding from Novo Nordisk, Boehringer Ingelheim, Eli Lilly as a member of advisory boards, and from Novo Nordisk, Boehringer Ingelheim, Eli Lilly as a speaker. G.F. received payment of honoraria from Lilly and Novo Nordisk as a member of advisory boards, and payment of honoraria for lectures as member of the OPEN Spain Initiative. The University of Leeds received funding from Novo Nordisk for J.C.G.H.s participation in the ACTION-Teens study. PS. received payment of honoraria and consulting fees from Novo Nordisk, Eli Lly, Pfizer, Boehringer Ingelheim and Bruno
Farmaceutici as a member of advisory boards. V.Y. received personal funding from Novo Nordisk and Eli Lilly as a member of advisory boards and from Novo Nordisk as a speaker. G.H.G. received research funding from the European Foundation for the Study of Diabetes, the Dutch Diabetes Research Foundation and the Dutch Research Council (NWO).
This article is excerpted from the naturemedicine by Wound world.
- 星期五, 05 7月 2024
女性雄激素性脱发诊断与治疗中国专家 共识(2022 版)
中华医学会整形外科学分会女性雄激素性脱发诊断与治疗专家共识编写组 中国女医师协会整形美容专业委员会
通信作者:张菊芳,浙江大学医学院附属杭州市第一人民医院医学美容科,杭州
310006,Email: zhjuf@ vip.sina. com;吴文育,复旦大学附属华山医院皮肤科,上海200040,Email: wuwenyu@ huashan.org.cn
【摘要】 女性雄激素性脱发与男性雄激素性脱发在病因、诊断、治疗等方面均有所不同,但目前国内外缺乏针对女性雄激素性脱发的诊断与治疗共识。 为了统一女性雄激素性脱发诊断及治疗标准,我国多个学术组织的专家共同启动了女性雄激素性脱发诊断与治疗专家共识的制定。 该共识包括女性雄激素性脱发的命名、流行病学、发病机制、临床表现、诊断依据及鉴别诊断要点、脱发分级、诊断流程、治疗方法。 基于相关循证医学证据,将共识编写组专家意见汇总,形成推荐意见,为临床医生提供参考。
【关键词】 脱发; 女性雄激素性脱发; 诊断; 治疗; 专家共识
基金项目: 国家自然科学基金 ( 82173442, 82103759); 上海毛发医学工程技术研究中心(19DZ2250500);上海申康医院发展中心临床三年行动计划( SHDC2020CR2033B);上海市科学技术委员会西医引导类项目(19411962400);杭州市医学重点学科(OO20200044)
DOI:10
- 星期一, 01 7月 2024
|指南与共识|中国黄褐斑诊疗专家共识(2021版)
黄褐斑(melasma)是一种慢性、获得性面部色素增加性皮肤病,临床表现为对称分布于面颊、前额及下颌深浅不一、边界不清的淡褐色或深褐色斑片,亚洲育龄期女性发病率高达30%[1],易复发,难治愈。2015年12月,中国中西医结合学会皮肤性病专业委员会色素病学组、中华医学会皮肤性病学分会白癜风研究中心、中国医师协会皮肤科医师分会色素病工作组在杭州共同制订了中国黄褐斑治疗专家共识(2015版)[2]。随着对黄褐斑发病机制研究的深入及临床分期分型的提出,其治疗有了新进展,2020年7月上述专家组在昆明修订了中国黄褐斑诊疗专家共识。
中国黄褐斑诊疗专家共识(2021版)
中国中西医结合学会皮肤性病专业委员会色素病学组
中华医学会皮肤性病学分会白癜风研究中心
中国医师协会皮肤科医师分会色素病工作组
通信作者:何黎,Email:该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。:许爱娥,Email:该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。
【引用本文】 中国中西医结合学会皮肤性病专业委员会色素病学组,中华医学会皮肤性病学分会白风研究中心,中国医师协会皮肤科医师分会色素病工作组.中国黄褐斑诊疗专家共识(2021版)[J],中华皮肤科杂志,2021.54(2):110-115.doi:10.35541/cjd.20200900
【关键词】黄褐斑;指南;诊断;治疗
- 星期五, 28 6月 2024
中国年龄相关性黄斑变性临床诊疗指南(2023年)
年龄相关性黄斑变性(age-related macular degeneration,AMD)是老年人群低视力乃至失明的主要原因[ 1 ],2040年全球AMD患者数量预计将达到2.88亿例[ 2 , 3 ]。我国70岁以上人群AMD的患病率为20.2%[ 3 ],随着我国人口老龄化的加剧,AMD的患者数量也在持续上升。
2013年国际Beckmann AMD分类研究小组根据临床表现,将AMD分为无明显年龄性改变、正常年龄性改变、早期AMD、中期AMD和进展期AMD[ 4 ]。年龄相关性眼病研究(Age-related Eye Disease Study,AREDS)小组的AMD分期标准与Beckmann分期类似[ 5 ]。进展期AMD又分为地图样萎缩(geographic atrophy,GA)和新生血管性AMD,新生血管性AMD也称为渗出性或湿性AMD,占AMD的10%~20%[ 1 ]。随着相干光层析成像术(optical coherence tomography,OCT)的应用和AMD研究深入,国际AMD命名共识研究组于2020年更新了新生血管性AMD黄斑区新生血管(macular neovascularization,MNV)的分型,根据OCT图像中MNV的起源和位置,将其分为1、2和3型[ 6 ]。
除了AMD相关分型更新,近10年眼底影像学检查技术和设备也飞速发展,相干光层析血管成像术(optical coherence tomography angiography,OCTA)等多模影像为AMD的诊断和随访提供了新的视角和工具[ 7 , 8 ];在新生血管性AMD的治疗方面,单克隆抗体类和融合蛋白类抗血管内皮生长因子(vascular endothelial growth factor,VEGF)药物不断更新和发展,不同的给药方案和随访间隔也为患者提供了更为多样的干预策略[ 9 , 10 , 11 ]。在强调精准、个体化治疗的时代,对于疾病的不同阶段需要选择合适的检查和治疗方案,这对眼底病医师提出了更高要求,也给临床工作带来了新的挑战。
然而,目前我国眼科医师对于AMD新的分型、检查设备和干预策略的认识尚不充分,眼底病医师与眼科其他亚专科医师对AMD的认知存在差距,各地区、各层级医院AMD的检查设备等硬件设施以及防治理念和水平等不同,因此AMD的规范诊疗亟待加强和完善。
基于此,为了更好地指导我国眼科医师开展相关临床工作,中华医学会眼科学分会眼底病学组、中国医师协会眼科医师分会眼底病学组与国家眼部疾病临床医学研究中心,基于最新循证医学证据,结合国际指南和我国社会经济发展现状,在2013年《中国年龄相关性黄斑变性临床诊断治疗路径》[ 12 ]基础上,于2023年制订我国AMD临床诊疗指南,以期有助于规范我国AMD的诊断、治疗、预防和随访工作。
一、指南制订方法
(一)指南制订的理论依据和方法学
本指南由中华医学会眼科学分会眼底病学组和中国医师协会眼科医师分会眼底病学组发起制订,证据质量和推荐意见强度的评价方法采用GRADE(grading of recommendations,assessment,development and evaluation,推荐分级的评估、制订与评价)系统( 表1 )[ 13 , 14 , 15 , 16 ],由宁波诺丁汉GRADE中心提供方法学支持。指南设计与制订步骤依据世界卫生组织(world health organization,WHO)发布的《世界卫生组织指南制订手册》,参考美国医学科学院提出的临床实践指南定义[ 17 ]以及2016年中华医学会发布的《制订/修订〈临床诊疗指南〉的基本方法及程序》[ 18 ]。本指南已在国际实践指南注册与透明化平台(http://www.guidelines-registry.cn)注册(注册号:IPGRP-2021CN111)。
展开阅读
| 分级 | 描述 |
|---|---|
| 证据质量分级 | |
| 高(A) | 对观察值非常有把握:观察值接近真实值 |
| 中(B) | 对观察值有中等把握:观察值有可能接近真实值,但也有可能差别很大 |
| 低(C) | 对观察值的把握有限:观察值可能与真实值有很大差别 |
| 极低(D) | 对观察值几乎无把握:观察值与真实值可能有极大差别 |
| 推荐强度分级 | |
| 强(1) | 明确显示干预措施利大于弊或弊大于利 |
| 弱(2) | 干预措施利弊不确定或无论证据质量高低,均显示利弊相当 |
GRADE的证据质量和推荐强度分级[ 13 , 14 , 15 , 16 ]
注:GRADE示推荐分级的评估、制订与评价
GRADE是目前使用最广泛的证据评价和推荐意见分级系统,包括2个部分。第1部分为证据评价,根据证据中的偏倚风险、不一致性、间接性、不精确性和发表偏倚,将证据质量分为高、中、低和极低4个水平。第2部分为推荐意见分级,参考医学干预的利弊平衡、证据质量、价值观念与偏好以及成本与资源耗费等因素制订推荐意见,并将推荐意见分为强推荐和弱推荐(有条件推荐)2种。医学干预的利弊差别越大,证据质量越高,价值观念与偏好越清晰越趋同,成本与资源耗费越小,则越应为强推荐;反之,则应为弱推荐(有条件推荐)[ 15 , 16 ]。强推荐代表绝大多数甚至全部目标群体的医学决策应遵循推荐意见;弱推荐代表推荐意见应有条件适用于目标群体,并应考虑医患共同决策( 表1 )。
(二)指南使用者和目标人群
本指南供我国从事眼科专业的临床医师及与AMD健康管理相关的专业人员使用。指南推荐意见的主要应用目标人群为我国AMD患者。
(三)指南工作组
指南工作组由指南指导委员会、指南共识专家组、指南制订工作组(包括指南学术秘书组和证据评价组)及指南外审专家组构成。参与指南制订的工作人员均由首席临床专家和方法学专家推荐。指南共识专家组和指南外审专家组成员由来自全国24个省或直辖市的80余名眼科专家和循证医学专家组成。
(四)利益冲突说明
依据WHO以及国际指南联盟的利益冲突管理指导原则,对参与指南制订的工作人员进行利益冲突管理,均向中华医学会眼科学分会提供《个人利益冲突声明表》(包含财务和专业相关的利益冲突内容),均不存在利益冲突。
(五)临床问题遴选和确定
指南指导委员会和指南共识专家组对AMD诊疗相关临床问题进行探讨。以最初提出可能相关的临床问题为基础,使用在线调查形式对所有指南共识专家组和指南外审专家组成员进行调查。随后由指南指导委员会、指南共识专家组和指南学术秘书组召开会议,对最初临床问题进行多轮修改和讨论,最终确定拟解决的8个临床问题,其中1个临床问题聚焦于AMD诊断,其余7个临床问题聚焦于AMD治疗。
指南指导委员会和指南共识专家组通过讨论,针对每个临床问题选取了对推荐意见至关重要(以*表示)及重要的临床结局(观测时间点均为1年及以上)。(1)针对诊断临床问题:诊断方法的灵敏度和特异度*,不良事件发生率*(包括严重的眼部不良事件、严重的系统性不良事件等),经济学指标;(2)针对治疗临床问题:最佳矫正视力(best corrected visual acuity,BCVA)字母数较基线水平的平均变化值*,至少改善5、10、15个BCVA字母数患者的占比*,至少丢失5、10、15个BCVA字母数患者的占比*,中央视网膜厚度(central retinal thickness,CRT)较基线水平的变化值,色素上皮脱离(pigment epithelial detachment,PED)高度较基线水平的平均变化值,PED消退率,治疗次数,治疗后OCT检查显示无神经上皮内或神经上皮下积液的患者人数,生活质量,严重的眼部不良事件发生率,严重的系统性不良事件发生率,抗血小板研究协作组事件,经济学指标。
(六)证据检索
1.文献检索:指南证据评价组针对最终纳入的临床问题和结局指标,按照人群(population,P)、干预(intervention,I)、对照(comparator,C)、结局(outcome,O)进行解构。对相关研究证据进行系统且全面检索。检索中国知网、万方数据知识服务平台、维普论文检测系统和中国生物医学文献服务系统等中文数据库,以及PubMed、Embase、Web of Science、the Cochrane Library等英文数据库。检索时间跨度为自建库至2022年6月1日。除数据库检索外,同时检查国内外相关指南、系统评价中的纳入研究,以及指南指导委员会、指南共识专家组和指南学术秘书组成员补充的相关关键研究,以最终确定符合纳入标准的研究。
2.文献筛查提取与质量评估:事先针对每个临床问题制订纳入和排除标准,并设计数据提取表格。优先纳入随机对照试验(randomized controlled trial,RCT);缺乏RCT证据时,根据证据强度补充纳入非RCT或非对照研究证据。由2名指南证据评价组成员独立进行文献筛查(根据文题、摘要及全文)及数据提取工作,由第3名指南证据评价组成员协助解决出现的分歧。采用Cochrane偏倚风险评估工具[ 19 ]对纳入的RCT实施风险偏倚评估;采用Newcastle-Ottawa量表(Newcastle-Ottawa Scale,NOS)对纳入的非随机对照研究(如队列研究、病例对照研究、自身前后对照研究)进行风险偏倚评估[ 20 ]。
(七)证据评价和推荐意见形成
在针对每个临床问题进行证据汇总时,使用GRADEpro指南开发工具(www.gradepro.org)构建GRADE证据概要和证据到决策(evidenc to decision,EtD)框架,总结系统评价的结果[ 13 , 14 , 16 ]。每个临床问题对应的EtD表格均包括与干预和对照措施相关的有效性和安全性、资源使用(医疗费用等)、成本效益、患者价值和偏好、对卫生公平性的影响、可接受度和可行性等部分。
指南指导委员会及指南共识专家组通过多轮线上视频讨论会和线下专家共识会,审阅和讨论了指南证据评价组提供的关于AMD诊断、治疗等方面的国内外循证医学证据概况、证据的质量或可信度以及EtD表格。最终使用GRADE系统进行临床推荐意见强度评级。指南指导委员会和指南共识专家组以讨论和投票相结合的方式,就推荐意见的方向和强度以及相关使用注意事项达成共识。
(八)外部评审
推荐意见达成共识并形成文字初稿后,提交指南外审专家组进行评审。
(九)指南的传播和实施
本指南发布后,将主要通过以下方式进行传播、实施和评价:(1)在《中华眼科杂志》发表本指南全文,包括本指南制订的具体方法、步骤以及指南工作组的成员和分工。(2)在全国性学术会议中宣讲,为从事AMD诊疗工作的眼科医师解读本指南内容并进行相关培训;(3)在国内部分省(市)有计划组织针对本指南内容的推广会议,推动临床眼科医师全面、准确掌握和应用本指南;(4)通过线上多媒体形式推广本指南内容;(5)在未来2年定期开展相关研究,对国内AMD诊断和治疗现状进行评价,进一步了解本指南实施后的传播应用价值和对临床决策的作用。
二、AMD的流行病学特征
AMD是全球范围内导致严重及不可逆性视力损伤的主要原因之一[ 2 ]。全球AMD的总患病率约为8.69%(年龄范围为45~85岁)。预计到2040年,患者数量将增长至2.88亿例[ 2 ]。
我国AMD的患病率从45~49岁人群的2.44%逐渐提升至85~89岁人群的18.98%。早期AMD的患病率为1.79%~10.05%,进展期AMD的患病率为0.38%~3.88%;在进展期AMD患者中,GA的患病率为0.15%(45~49岁人群)~1.09%(85~89岁人群),新生血管性AMD的患病率为0.24%~2.79%[ 21 ]。我国AMD患者数量从1990年的1 201万例增加至2015年的2 665万例,预计到2050年将增加至5 519万例[ 21 ]。在地区分布方面,我国中南部地区AMD患者数量最多(2010年为752万例),西北地区最少(2010年为95万例)[ 21 ]。随着我国社会老龄化进程发展,未来AMD导致的社会经济负担将进一步加重。
2020年,全球50岁及以上人群因AMD致盲人数约为180万,导致中度及重度视力损伤的人数约为620万[ 22 ]。在我国,AMD也是引起视力损伤的主要原因之一。一项针对1990至2019年我国视力障碍和失明人群的研究结果显示,由AMD导致的中至重度视力损伤以及致盲的人数分别为228万及32万[ 23 ]。
三、AMD的危险因素
(一)年龄
AMD发生和发展的主要危险因素为年龄。AMD的患病率、发生率及严重程度均随年龄的增长而增高,几乎所有进展期AMD均发生在60岁以上人群中[ 24 ]。在Beaver Dam Eye研究中,75岁及以上人群以下病变的发生率明显高于43~54岁人群:较大玻璃膜疣(24%与1.9%)、软性玻璃膜疣(23%与2.1%)、视网膜色素上皮细胞(retinal pigment epithelium,RPE)异常(26.6%与7.3%)、MNV(5.2%与0.1%)和GA(2.0%与0)[ 25 ];此外,Blue Mountains Eye研究(Blue Mountains Eye Study,BMES)的结果也显示,AMD所有典型病变的发生率随年龄增长而增加,进展期AMD在55岁以下人群中的发生率为0,而在85岁及以上人群中为18.5%[ 26 ]。一项针对1990至2013年欧洲AMD患者的荟萃分析结果也显示,早期AMD的患病率从55~59岁人群的3.5%逐渐增加至85岁及以上人群的17.6%,进展期AMD的患病率对应从0.1%增加至9.8%[ 27 ]。
(二)种族
不同种族人群的AMD患病率有差异。研究结果表明,白色人种AMD的患病率高于有色人种[ 28 , 29 ]。一项全球性荟萃分析结果显示,欧洲人AMD的患病率(12.3%)高于亚洲人(7.4%)和非洲人(7.5%),而亚洲人与非洲人的患病率无明显差异[ 2 ]。欧洲人GA的患病率高于非洲人和亚洲人,而新生血管性AMD在所有种族中的患病率接近[ 2 ]。此外,新生血管性AMD的亚型之一,即息肉样脉络膜血管病变(polypoidal choroidal vasculopathy,PCV)的患病率在不同种族间存在明显差异,亚洲地区的相关报道较多[ 30 ]。Beijing Eye 研究报道中国PCV的患病率为0.3%±0.1%[ 31 ],在中国PCV占新生血管性AMD的22.3%~43.4%[ 32 , 33 ]。
(三)其他危险因素
1.遗传性因素:遗传学研究证据显示,AMD家族史可增加AMD的发生风险[ 34 ]。目前研究确认的遗传因子主要包括补体因子H的Y402H基因、ARMS2基因、HTRA1基因等[ 35 , 36 , 37 , 38 ]。以上基因的多态性与AMD的发生风险相关,基因与其他风险因素的组合可能进一步增加AMD的患病风险[ 39 ]。
2.吸烟:吸烟是AMD的重要危险因素,已被证明可显著增加各种AMD的发生风险,且可能存在剂量反应关系[ 34 , 40 ]。被动吸烟同样可能增加AMD的发生风险,而戒烟则与AMD的进展风险降低相关[ 40 ]。
3.高血压:高血压可增加AMD的发生风险[ 41 , 42 ],但部分研究结果显示收缩压升高与AMD的发生风险降低相关[ 43 ]。由于研究结论不一致[ 43 ],冠心病等心血管疾病与AMD的关系有待进一步探讨。
4.饮食:多项研究结果显示,AMD的发生风险降低与富含Omega-3长链多不饱和脂肪酸食物(如鱼类)的摄入量增加有关[ 44 , 45 ]。AMD发生风险增加与摄入多量饱和脂肪和胆固醇以及体质量指数较高有关[ 46 ]。此外,研究结果显示,富含水果、蔬菜、豆类和鱼的地中海饮食与发展为进展期AMD的风险降低相关[ 47 , 48 ]。
四、AMD的病理生理改变
AMD的主要病理生理改变是外层视网膜、RPE、Bruch膜及脉络膜毛细血管层的退行性病变,以黄斑区细胞外沉积物为典型特征。早期病理表现为基板沉积物和基线沉积物[ 49 ]。这两种类型沉积物可能体现了RPE对细胞应激的不同反应,导致了早期AMD的主要表现,即玻璃膜疣和RPE异常[ 50 ]。基板沉积物主要位于RPE细胞膜与RPE基板之间,进行性基板沉积物沉积最终引起RPE异常。基线沉积物主要由位于RPE基板与Bruch膜内胶原层之间的弥漫性膜性碎片集合组成[ 51 ],基线沉积物聚集融合形成软性玻璃膜疣[ 51 ]。
根据临床表现、大小、位置等不同,玻璃膜疣分为4种类型。
1.硬性玻璃膜疣:彩色眼底图像中表现为小的(直径<63 μm,相当于视盘边缘视网膜主要静脉直径的一半,或1/24视盘直径)[ 51 ]、散在的RPE下黄白色沉积物,边缘清晰,在黄斑区及周边视网膜均可见;荧光素眼底血管造影术(fundus fluorescence angiography,FFA)图像中表现为轻度强荧光,吲哚青绿血管造影术(indocyanine green angiography,ICGA)图像中表现为强荧光;组织学检查表现为圆形、边界分明、充满均质透明物质[ 51 ]。硬性玻璃膜疣可以是视网膜组织衰老的表现,也可出现于AMD。
2.软性玻璃膜疣:位于后极部,尤其黄斑区,彩色眼底图像中表现为较大的黄白色沉积物,中心颜色更白;OCT图像中表现为较大的RPE下沉积,呈高反射;FFA图像中通常表现为晚期强荧光,ICGA图像中表现为强荧光;组织学检查表现为充满膜性碎片。其发生和发展可能与RPE脱离和弥漫性Bruch膜异常改变有关,可进一步导致脉络膜新生血管(choroidal neovascularization,CNV)、RPE细胞死亡和GA[ 52 ]。Ferris等[ 4 ]在研究中发现单眼和双眼黄斑区软性玻璃膜疣伴有双眼黄斑区RPE异常者,5年内发展为进展期AMD的风险分别为25.6%和47.3%,黄斑区软性玻璃膜疣和RPE异常增加了发展为进展期AMD的风险。
3.表皮玻璃膜疣:彩色眼底图像中表现为黄斑区和周边视网膜大量(数量>50个)、小的(直径为25~75 μm)点状沉积物,早期在彩色眼底图像中不易发现;OCT图像中表现为RPE下长形中等高反射、锯齿状病灶;较大的表皮玻璃膜疣可侵蚀RPE层,因此每个表皮玻璃膜疣的顶端仅覆盖1层薄色素上皮,FFA图像中表现为星空样(密集分布的强荧光点),ICGA图像中表现为早期强荧光;组织学检查表现为Bruch膜内部弥漫性和结节状增厚[ 51 ]。表皮玻璃膜疣可出现于AMD、基底膜沉积物相关性疾病(如2型膜增生性肾小球肾炎等)和补体因子H基因突变。
4.视网膜下玻璃膜疣样沉积物(subretinal drusenoid deposit,SDD):也称网状假性玻璃膜疣(reticular pseudodrusen,RPD)。沉积物位于视网膜外层与RPE之间,在彩色眼底图像中表现为点状或网状分布,多见于黄斑区,较硬性玻璃膜疣颜色更白、形态更不规则;OCT图像中表现为最初SDD在RPE与椭圆体带之间沉积,而后突破椭圆体带,随后消退;FFA图像中表现为弱荧光或无变化,ICGA图像中表现为中晚期弱荧光;组织学检查表现为RPE细胞内液泡物质从顶端表面释放形成SDD[ 51 ]。SDD与AMD的疾病进展密切相关,SDD是发展为进展期AMD的独立危险因素[ 53 ],其中点状SDD易进展为新生血管性AMD,而融合性SDD易进展为GA。
GA的核心机制是RPE功能丧失,其特征为Bruch膜严重破坏,RPE和光感受器细胞明显萎缩和丢失,视网膜其他类型细胞(水平细胞、双极细胞和无长突细胞)丢失,脉络膜毛细血管灌注不良以及炎性反应表现突出(在退行区存在大量激活的小胶质细胞和巨噬细胞)[ 54 ]。年龄相关性眼病研究2(Age-related Eye Disease Study 2,AREDS2)的结果显示,GA增长速率(经平方根转换)已发生GA的患眼为0.29 mm/年,新发GA的患眼为0.28 mm/年[ 55 ]。另一项包含BMES和Rotterdam 研究的队列研究的结果显示,GA的平均增长速率为1.09 mm2/年[ 56 ]。GA增长速率提高与更低的受教育水平,对侧眼存在GA或CNV[ 57 ],GA的大小、位置和数量以及遗传因素有关[ 55 ]。
新生血管性AMD的新生血管从脉络膜毛细血管中生长,突破Bruch膜进入视网膜下或RPE下间隙。新生血管的生长与促血管生成因子和抗血管生成因子的局部平衡改变有关,如与VEGF、胎盘生长因子(placental growth factor,PlGF)、血小板衍生生长因子(platelet-derived growth factor,PDGF)等促血管细胞因子的过表达,以及金属蛋白酶组织抑制因子(tissue inhibitor of metalloproteinase,TIMP)等抑制血管生成因子的表达减少[ 58 ]有关,而缺氧和炎性反应可能是导致平衡改变的启动因素[ 59 ]。此外,新生血管主要由增殖的血管内皮细胞组成,作为不成熟的毛细血管,可导致渗漏、出血、水肿、脂质沉积、PED、晚期纤维瘢痕形成等[ 60 ]。
五、AMD的临床表现
(一)临床分期
根据临床表现,AREDS小组将AMD分为无AMD期、早期、中期和进展期。
1.无AMD期:无或仅有少量小玻璃膜疣[ 1 ]。
2.早期AMD:主要表现为多个小玻璃膜疣(直径<63 μm),较少量中等大小玻璃膜疣(直径为63~124 μm)或轻度RPE异常[ 1 ]。
3.中期AMD:随时间推移,细胞外沉积物蓄积,色素移行进入视网膜,玻璃膜疣增大,RPE发生色素减退和色素沉着[ 6 ]。主要表现为单眼或双眼存在广泛的中等大小玻璃膜疣(直径为63~124 μm),或至少1个大玻璃膜疣(直径≥125 μm),或出现未累及黄斑中心凹的GA[ 1 ]。
4.进展期AMD:表现为累及黄斑中心凹的GA或出现异常的MNV,可能伴有出血、硬性渗出、视网膜层间积液(intraretinal fluid,IRF)或视网膜下积液(subretinal fluid,SRF)、浆液性或出血性PED、神经上皮下或色素上皮下纤维血管增生、盘状瘢痕。患者视力受到影响[ 1 ]。
(二)CNV
根据解剖位置,CNV分为中心凹下型(指病变位于黄斑中心凹无血管区正下方)、中心凹旁型(指病变与黄斑中心凹无灌注区中央的距离<200 μm)和中心凹外型(指病变与黄斑中心凹无灌注区中央的距离≥200 μm)。
根据FFA表现,CNV分为经典为主型、微小经典型和隐匿型。经典型CNV在FFA早期表现为边界清晰的强荧光区域,晚期进行性荧光渗漏。隐匿型CNV包括纤维血管性PED和不明来源的晚期渗漏(late leakage of undetermined source,LLUS)。其中,纤维血管性PED的FFA表现为边界不清、不规则的RPE染色或渗漏,病灶表面通常出现混合点状强荧光;LLUS在FFA晚期表现为边界不清的渗漏区域,但在早期和中期无经典型CNV或纤维血管性PED导致的渗漏。CNV可兼具经典型和隐匿型表现,属于混合型。经典型表现占病变区域50%及以上,为经典为主型CNV;经典型表现占病变区域不足50%,为微小经典型CNV;无经典型表现,为隐匿型CNV[ 61 ]。
根据ICGA表现对CNV进行分类。FFA表现为经典型CNV的ICGA表现与FFA表现相似。FFA表现为隐匿型的CNV,根据ICGA表现可进一步分类:(1)焦点状CNV(热点CNV),指CNV强荧光范围直径≤1视盘直径(diameter of optic disc,DD),且边界清晰;(2)斑片状CNV,指CNV强荧光范围直径>1 DD,荧光强度较焦点状CNV弱;(3)混合型CNV,指同时存在焦点状和斑片状CNV[ 62 ]。
(三)MNV
在最新的国际AMD命名专家共识中,鉴于AMD中特殊类型视网膜血管瘤样增生(retinal angiogmatous proliferation,RAP)的新生血管来源于视网膜,而非脉络膜,使用“CNV”无法准确涵盖AMD中所有类型的新生血管,建议将既往使用的术语CNV更换为MNV[ 63 ]。MNV是指新生血管长入黄斑区视网膜、视网膜下腔或RPE下腔。基于新生血管在视网膜组织中的起源和存在部位不同,MNV分为1型、2型和3型。
1.1型MNV:起源于脉络膜毛细血管,向RPE下间隙生长,既往称为隐匿型CNV。随着病灶生长和扩大,脉络膜和病灶内的滋养血管和引流血管发生重塑,逐渐增粗。MNV在成纤维细胞、肌成纤维细胞和巨噬细胞等参与下,可形成纤维组织[ 6 , 63 ]。而新生血管的渗漏、出血和纤维组织增生又可能导致纤维血管性PED。
PCV是1型MNV的重要亚类,以脉络膜异常分支血管网和分支血管网边缘的结节样血管团块(息肉)为特征性改变[ 6 , 63 ]。表现为脉络膜血管异常扩张,大量纤维蛋白和血浆渗出,动脉硬化且平滑肌丢失;分支血管网的血管可异常粗大,部分息肉具有搏动性,并易出血。对于息肉是简单的动脉瘤还是更复杂的血管结构,目前尚未达成共识[ 6 ]。PCV通常无玻璃膜疣和色素异常,且较少发展为黄斑萎缩。
2.2型MNV:起源于脉络膜毛细血管,穿过RPE后在视网膜下间隙生长,既往称为经典型CNV。其合并的出血和渗出可直接进入视网膜下腔。2型MNV可与其他类型MNV同时存在[ 6 , 63 ]。1-2混合型MNV既有1型又有2型MNV。
3.3型MNV:既往称为RAP,异常血管并非起源于脉络膜,可能起源于视网膜深层毛细血管丛,向外层视网膜延伸。血管增生进一步蔓延至RPE,最终可导致RPE破裂、RPE下新生血管形成,并可能与更深层血管吻合[ 6 , 63 ]。视网膜内散在斑片状出血和囊样水肿出现于新生血管形成之前。3型MNV可表现为IRF、SRF、PED和渗出。
PED是因RPE下玻璃膜疣样物质、积液、出血和纤维血管组织等导致RPE层及其下方的基板与Bruch膜内胶原层分离。根据RPE与Bruch膜之间成分不同,PED分为浆液性PED、出血性PED、纤维血管性PED和混合性PED等,其中浆液性PED可发生在非新生血管性AMD。还有一类特殊的PED称为玻璃膜疣样PED,AREDS小组将其定义为直径>350 μm、边界清楚、由软性玻璃膜疣融合导致的PED。玻璃膜疣样PED是中期AMD进展为GA或新生血管性AMD的危险因素。1型和3型MNV均可出现PED,1型MNV出现PED的原因是RPE层下新生血管渗漏、出血等,而3型MNV发生PED的原因尚不明确[ 6 , 63 ]。
六、AMD的诊断
(一)病史采集
50岁以上初次就诊患者应询问患者主诉和相关病史。AMD的症状包括视力下降、视物变形、视野中心暗点、闪光感、暗适应差等。应询问症状出现的时间、严重程度、视物变形或中心暗点的范围等。应针对AMD的危险因素进行仔细询问,包括患者的年龄、性别、种族等基本资料;眼病史;高血压病、糖尿病、动脉硬化等全身疾病史;家族史,尤其AMD家族史;个人史,吸烟、饮酒史以及其他简要的社会史;饮食及服用药物情况、营养补充剂的使用情况等。
(二)初步检查
检查裸眼视力、远近最佳矫正视力、眼前节情况。使用检眼镜或裂隙灯显微镜联合前置镜检查眼底,是所有初诊患者必须进行的初步检查,有助于AMD的诊断及分期,以指导后续的检查和治疗。Amsler方格表是重要、便捷、灵敏的黄斑功能检测工具。对于具有视物变形、中心暗点、视力下降等疑似AMD症状的患者,均应进行Amsler方格表检查,有助于明确患者视物变形的范围或暗点的相对位置。
(三)眼底照相
眼底照相能够清晰、准确、客观记录AMD患者眼底病变情况,有利于评估疾病程度、病变进展及治疗效果,可作为患者随访和长期管理的重要资料。
(四)FFA和ICGA检查
FFA既往是诊断和随访AMD的唯一检查方法,可判断是否存在MNV,并评估MNV的类型、大小、位置、活动性等。然而,随着OCT、OCTA等无创检查方法广泛应用,造影检查在AMD的诊断和随访中部分被替代。但是,在必要时造影检查仍可作为确定诊断、判断疾病类型、评估MNV病灶活动性的有效方法之一。
1型MNV的FFA主要表现为边界不清、弥漫、多点状的荧光渗漏(多位于隆起的RPE下方),而ICGA多仅表现为晚期斑块状强荧光,少数可显示部分新生血管结构;PCV的形态特征则ICGA显示最佳,表现为早期异常的分枝状血管网、结节样病灶充盈,晚期荧光渗漏或着染。ICGA仍是PCV诊断的金标准[ 64 ]。2型MNV的FFA表现为较早出现的境界清晰的强荧光灶,晚期荧光渗漏。3型MNV的FFA主要表现为囊样水肿区域内的强荧光积存,而ICGA可能发现较小的强荧光病灶[ 65 ]。
检查者须密切关注使用造影剂的潜在风险,如疼痛、组织渗漏、过敏反应等,并准备应对不良反应的应急处理预案,以减少造影剂相关医疗安全事件发生。
(五)OCT检查
OCT是诊断和随访AMD的重要检查方法,无创且便捷,与其他眼科影像学检查相比,其B扫描可同时观察视网膜各层切面结构,对于发现MNV病灶、判断分型及疾病活动性更具优势[ 66 ]。尤其在随访模式下,OCT可精确采集视网膜的结构图像并比较其变化,有助于AMD的疗效评估和及时调整治疗方案。新一代扫频OCT(swept-source OCT,SS-OCT),波长为1 050~1 060 nm,穿透力更强,分辨率更高,检出视网膜和脉络膜结构异常的能力明显提高。
1型MNV的OCT主要表现为RPE层下的中高反射,常伴有纤维血管性或浆液性PED、SRF、IRF等;PCV的OCT主要表现为脉络膜息肉样病灶呈指状隆起,分枝状血管网呈扁平或波浪样RPE隆起、与Bruch膜形成双线征,常伴有PED等渗出性改变[ 64 ]。2型MNV的OCT主要表现为视网膜下的中高反射,常伴有视网膜增厚、SRF、IRF等[ 67 ]。3型MNV即RAP的OCT典型表现为视网膜内高反射条带向深层组织延伸,常伴有PED和IRF[ 68 ]。
(六)OCTA检查
OCTA是一种新型的眼底影像学检查方法。眼底血管中存在流动的血细胞,对同一横断面进行重复的相干光层析成像后,通过特殊的计算方法,获得移动血细胞即血流信号,并据此重建血管的三维结构,以冠状面形式逐层显示眼底血管影像。OCTA能够无创评估视网膜和脉络膜血管系统,与传统造影检查方法比较,具有无创、快速、安全、可重复检查等优势,已在AMD的诊断和管理中得到较为广泛应用。OCTA可用于发现、观察和随访新生血管性AMD病灶。基于循证医学证据综合分析,OCTA诊断MNV的效力与FFA接近(灵敏度为91%,特异度为73%)[ 66 , 69 , 70 , 71 , 72 , 73 ]。在PCV的诊断方面,OCTA的灵敏度为79%,特异度为72%[ 8 , 74 , 75 ];OCT联合OCTA的灵敏度为84%,特异度为67%[ 8 , 74 ]。在RAP的诊断方面,对于FFA或ICGA发现的病灶区域,OCTA可观察到对应的异常血流信号[ 76 ]。其他研究结果也显示了OCTA对新生血管类病灶具有诊断能力[ 7 , 77 ]。在分析OCTA图像过程中,应避免分层错误、投射伪影等对新生血管识别的干扰。
[推荐意见1]
诊断新生血管性AMD,相较于FFA或ICGA,有条件推荐OCT联合OCTA作为检查方法(2B)。
[推荐说明]
1.在新生血管性AMD的MNV病灶诊断方面,OCTA的灵敏度和特异度与FFA或ICGA相似,可用于检查新生血管性AMD,以便准确、无创诊断新生血管性AMD,并减少造影可能引起的不良反应。OCT的B扫描可有效显示IRF、SRF、PED等,便于对新生血管性AMD活动性进行判断。因此,对于新生血管性AMD(除外PCV和RAP),建议以OCT联合OCTA作为检查和诊断方法。
2.在PCV诊断方面,ICGA的灵敏度和特异度均优于OCTA,ICGA仍是PCV检查和诊断的金标准。
3.在RAP诊断方面,尚无充足证据证明OCTA的灵敏度和特异度优于FFA或ICGA,OCT仍为RAP的常用检查和诊断方法。
4.初诊时建议常规进行眼底照相、OCT;当OCT发现可疑病灶时(如发现PED或可疑PCV),根据需要进行FFA、ICGA或OCTA以明确病灶和诊断。若患者全身情况不允许行FFA或ICGA(如磺胺或碘过敏、肝肾功能不全等),可考虑进行OCTA。
七、AMD的治疗
(一)早至中期AMD的治疗
早至中期AMD患者视功能尚无明显损伤,治疗目标为防止向进展期AMD发展,防止视力明显下降。在防止向进展期AMD发展方面,可补充抗氧化维生素(维生素C、维生素E)、矿物质(锌、铜)、叶黄素、玉米黄质等。补充不同抗氧化维生素和矿物质呈现不同的治疗效果。
在一项针对AMD患者补充抗氧化维生素和矿物质的大型研究(AREDS)中,受试者每日口服维生素C(500 mg)、维生素E(400 IU)、β胡萝卜素(15 mg)、氧化锌(80 mg)、氧化铜(2 mg,预防锌引起的铜缺乏性贫血)[ 5 ]。在一项针对中期AMD(双眼存在大玻璃膜疣或1只眼存在大玻璃膜疣、对侧眼为进展期AMD,此类患者具有较高风险发展为进展期AMD)开展的多中心、随机、双盲、安慰剂对照的Ⅲ期临床试验(AREDS2)中,在AREDS配方基础上使用叶黄素(10 mg)和玉米黄质(2 mg)取代β胡萝卜素,补充锌(80 mg或25 mg),增加Omega-3长链不饱和脂肪酸[ 78 ]。在现有的多项相关研究中,针对早至中期AMD的营养补充剂也多为叶黄素(10 mg或20 mg)、玉米黄质(10 mg)、混合维生素和矿物质、硫酸锌(200 mg)、二十二碳六烯酸(docosahexaenoic acid,DHA)(840 mg)和二十碳五烯酸(eicosapentaenoic acid,EPA)(270 mg)等[ 5 , 78 , 79 , 80 , 81 , 82 , 83 , 84 , 85 , 86 , 87 , 88 , 89 ]。
[推荐意见2]
基于目前的循证医学证据[ 5 , 78 , 79 , 80 , 81 , 82 , 83 , 84 , 85 , 86 , 87 , 88 , 89 ],建议早至中期AMD补充抗氧化维生素、锌(氧化锌或硫酸锌)、叶黄素、玉米黄质,或者混合型抗氧化维生素和矿物质(2B);抗氧化维生素和矿物质补充需达到一定剂量才可能产生相应获益;不建议补充脂肪酸(B)。
[推荐说明]
针对早至中期AMD营养补充剂,采用循证医学方法共检索到2 632篇文献,最终纳入系统评价2项,临床试验13项。早期AMD治疗研究结果显示,补充叶黄素、玉米黄质可提高黄斑区色素水平和对比敏感度,但是目前尚无证据表明补充抗氧化维生素、矿物质能够阻止早期AMD进展为中期或进展期AMD[ 5 , 78 , 79 , 80 , 81 , 82 , 83 , 84 , 85 , 86 , 87 , 88 , 89 ]。
基于循证医学证据[ 5 , 78 , 79 , 80 , 81 , 82 , 83 , 84 , 85 , 86 , 87 , 88 , 89 ]进行综合分析,发现对于早至中期AMD,补充抗氧化维生素和矿物质等1年以上,能够降低BCVA丢失10个及以上字母患者的比例;与安慰剂相比,补充叶黄素或叶黄素及玉米黄质者的BCVA略高。与安慰剂相比,补充锌(硫酸锌或氧化锌)1年以上,发展到进展期AMD、BCVA丢失10个字母以上的风险降低。与安慰剂相比,补充营养复合制剂1年以上,发展到进展期AMD的风险降低,BCVA略高,BCVA丢失15个字母以上的风险降低,生活质量略好。
此外,补充β胡萝卜素可能引起皮肤变黄,增加吸烟患者患肺癌的风险。补充锌可能增加因泌尿系统疾病而住院的风险,可能引起铜缺乏性贫血。当考虑长期补充上述营养物质时,须结合患者的全身情况,必要时联合相关专业医师进行综合判断,防止不良反应。
(二)新生血管性AMD的抗VEGF治疗
1.抗VEGF药物:抗VEGF药物玻璃体腔注射给药能够改善新生血管性AMD患者的视功能,恢复黄斑区解剖结构,是累及中心凹或中心凹旁MNV的一线治疗方法。目前我国可用于新生血管性AMD治疗的抗VEGF药物包括雷珠单克隆抗体、康柏西普和阿柏西普。
(1)雷珠单克隆抗体:雷珠单克隆抗体眼内注射液是一种重组人源化的单克隆抗体Fab片段,可靶向抑制VEGF-A的所有亚型。雷珠单克隆抗体是国家药品监督管理局批准的首个抗VEGF药物,于2011年开始用于临床治疗新生血管性AMD。推荐给药方案为每月玻璃体腔注射给药1次(0.5 mg/次),即每月或每4周方案;或者初始3个月每月玻璃体腔注射给药1次(0.5 mg/次),后按需给药(pro re nata,PRN),即3+PRN方案。
一项前瞻性、多中心、双盲、空白对照、采用雷珠单克隆抗体每4周方案(0.3 mg组和0.5 mg组)治疗继发于新生血管性AMD的微小经典型或隐匿型CNV的2年临床试验(Marina研究)结果显示,与空白对照组比较,平均视力提高0.3 mg组为6.5个字母,0.5 mg组为7.2个字母,而空白对照组平均视力下降10.4个字母[ 9 ]。另一项国际多中心、双盲、随机、采用雷珠单克隆抗体每4周方案(0.3 mg组和0.5 mg组)与光动力治疗(photodynamics therapy,PDT)(PDT组)对照,治疗继发于新生血管性AMD的经典为主型CNV的2年临床试验(Anchor研究)结果显示,平均视力提高雷珠单克隆抗体0.3 mg组为8.5个字母,雷珠单克隆抗体0.5 mg组为11.3个字母,而PDT组平均视力下降9.5个字母,对于经典为主型CNV,雷珠单克隆抗体治疗效果优于PDT[ 90 ]。基于上述研究结果,2006年雷珠单克隆抗体在美国获准用于新生血管性AMD治疗,开启了新生血管性AMD抗VEGF治疗的历程。
(2)康柏西普:康柏西普是我国自主研发的融合蛋白类抗VEGF药物,由人VEGF受体(VEGF receptor,VEGFR)1中的Ig区域2和VEGFR2中的Ig区域3和4与人Ig Fc片段融合而成,可同时阻断VEGF-A、VEGF-B和PlGF,于2013年获准用于治疗新生血管性AMD。推荐给药方案为初始3个月每月玻璃体腔注射给药1次(0.5 mg/次),之后每3个月玻璃体腔注射给药1次,即3+每3个月方案;或者在初始3个月每月玻璃体腔注射给药1次(0.5 mg/次)后PRN,即3+PRN方案[ 91 ]。
在一项康柏西普治疗新生血管性AMD的随机、双盲、多中心Ⅱ期临床试验(Aurora研究)中,患者随机分为康柏西普0.5 mg组(0.5 mg/次)和2 mg(2 mg/次)组,在初始3个月每月玻璃体腔注射给药1次后,2个组内再随机分为每月给药亚组和PRN亚组,治疗12个月后各亚组视力分别较基线平均提高14.31(0.5 mg组中3+PRN亚组)、9.31(0.5 mg组中3+每月给药亚组)、12.42(2 mg组中3+PRN亚组)、15.43个字母(2 mg组中3+每月给药亚组),康柏西普治疗新生血管性AMD具有良好的有效性和安全性[ 92 ]。在另一项采用康柏西普(0.5 mg/次)治疗新生血管性AMD的前瞻性、多中心、双盲Ⅲ期临床试验(Phoenix研究)中,康柏西普采用3+每3个月方案,治疗12个月患者的BCVA较基线提高9.98个字母,康柏西普采用3+每3个月方案能够有效治疗并改善新生血管性AMD患者的视功能[ 10 ]。
(3)阿柏西普:阿柏西普是全人源化融合蛋白,包含人VEGFR1的Ig结构域2、人VEGFR2的Ig结构域3和人IgG1的Fc区,可同时阻断VEGF-A、VEGF-B和PlGF,于2018年在我国获准用于临床。针对新生血管性AMD治疗的推荐给药方案为初始3个月每月玻璃体腔注射给药1次(2 mg/次)后每8周玻璃体腔注射给药1次,即3+每8周方案;或者初始3个月每月玻璃体腔注射给药1次(2 mg/次),之后采取治疗-延长给药(treat and extend,T&E),即3+T&E方案。
一项全球范围内观察阿柏西普治疗累及黄斑中心凹的新生血管性AMD有效性和安全性的多中心、随机、对照、双盲Ⅲ期临床试验(View 1和2研究)结果显示,阿柏西普每4周方案(0.5 mg/次或2 mg/次)或3+每8周方案(2 mg/次),与雷珠单克隆抗体每4周方案(0.5 mg/次)比较,治疗52周后视力维持(主要结局指标)作用相当[ 11 ]。在一项中国开展的多中心、随机、对照、双盲Ⅲ期临床试验(Sight研究)中,分别采用阿柏西普3+每8周方案(2 mg/次)和PDT治疗继发于AMD的经典为主型CNV共52周,平均视力前者提升15.2个字母,后者提升8.9个字母,阿柏西普在改善视力方面的疗效优于PDT [ 93 ]。
[推荐意见3]
单克隆抗体类或融合蛋白类抗VEGF药物均可有效治疗新生血管性AMD。
2.抗VEGF治疗方案:抗VEGF药物玻璃体腔注射给药是新生血管性AMD的一线治疗方法,大量临床试验结果证实抗VEGF药物能够有效改善新生血管性AMD患者的视功能,但是在临床实践中,由于患者依从性欠佳、给药方案不同、治疗不足等原因,新生血管性AMD患者抗VEGF治疗后视功能改善情况往往不如临床试验结果。因此,选择合适的抗VEGF治疗方案,对于增强患者依从性,提高治疗的可执行性,改善抗VEGF治疗效果,维持患者远期视力获益具有重要意义。
以往临床试验中所涉及的抗VEGF治疗方案主要包括两大类:(1)固定玻璃体腔注射给药间隔时间,包括每月注射给药1次(每月或每4周)方案;初始3个月每月注射给药1次后,每8周注射给药1次(3+每8周)方案;初始3个月每月注射给药1次后,每3个月注射给药1次(3+每3个月)方案。(2)个体化玻璃体腔注射给药,包括初始3个月每月注射给药1次后PRN(3+PRN)方案,初始3个月每月注射给药1次后T&E(3+T&E)方案。
3+PRN方案和3+T&E方案均需要评估疾病的活动性。新生血管性AMD疾病活动性的判断是基于患者视功能和黄斑解剖结构变化,如黄斑区新的出血、出现IRF或SRF、患者视力下降5个字母以上等[ 92 , 94 , 95 , 96 , 97 ]。3+PRN方案是在疾病再次出现活动性时给予抗VEGF治疗,而疾病无活动性时仅每月随访观察疾病状态。3+T&E方案是在每次随访时均给予抗VEGF治疗,疾病活动性用于决定玻璃体腔注射给药的间隔时间,若疾病无活动性则延长注射给药间隔时间,若疾病出现活动性则缩短注射给药间隔时间。临床试验中T&E的注射给药间隔时间多采用每次延长或缩短2周,直到最长注射给药间隔时间为12周[ 98 ]。部分临床试验中T&E的间隔时间采用每次延长或缩短4周,可将最长间隔时间延长至16周,以期减轻患者的治疗负担[ 99 ]。
在一项多中心、单盲、随机对照比较雷珠单克隆抗体与贝伐单克隆抗体采用每4周方案或3+PRN方案治疗新生血管性AMD的临床试验(Catt研究)中,采用雷珠单克隆抗体(0.5 mg/次)按3+PRN方案治疗1年,视力改善程度与雷珠单克隆抗体(0.5 mg/次)每4周方案无显著差异(提高6.8个字母与8.5个字母)[ 100 ]。另一项长达8年的临床试验结果证实,3+PRN方案能够使50%新生血管性AMD患者视力稳定或提高[ 101 ]。真实世界研究结果同样证实,3+PRN方案和其他非固定给药方案均可使50%~60%新生血管性AMD患者的视力保持稳定[ 102 , 103 , 104 ]。
几项前瞻性、多中心、随机对照比较雷珠单克隆抗体每4周方案与3+T&E方案治疗新生血管性AMD的临床试验(Trex、Trend和Cantreat研究)结果证实,两方案治疗后患者视力获益无显著差异,而后者注射给药次数则显著少于前者[ 95 , 96 , 97 ]。
康柏西普在其注册的研究中探索了玻璃体腔注射给药固定间隔时间方案和个体化PRN方案。在Phoenix研究中,采用康柏西普(0.5 mg/次)3+每3个月方案治疗12个月,BCVA较基线平均提高9.98个字母,CRT较基线平均降低99.63 μm。在Aurora研究中,康柏西普0.5 mg 3+PRN组在治疗12个月时BCVA较基线平均提高14.31个字母,CRT较基线平均降低119.8 μm。康柏西普3+每3个月方案和3+PRN方案可有效改善新生血管性AMD患者的视功能,并恢复眼部解剖结构[ 10 , 92 ]。
在一项使用阿柏西普治疗新生血管性AMD的Ⅳ期临床试验(Altair研究)中,采用2种3+T&E方案,即玻璃体腔注射给药间隔时间每次延长或缩短2周(2周组)和玻璃体腔注射给药间隔时间每次延长或缩短4周(4周组),治疗52周后发现2周组和4周组患者的视功能和眼部解剖结构均得到明显改善,且效果维持至96周。96周时玻璃体腔注射给药间隔时间56.9%和60.2%患者可延长至12周及以上,41.5%和46.3%患者可延长至16周[ 99 ]。
[推荐意见4]
抗VEGF药物玻璃体腔注射给药是新生血管性AMD的一线治疗方法。抗VEGF药物玻璃体腔注射给药可采用不同方案。根据目前循证医学证据[ 105 , 106 , 107 , 108 , 109 , 110 , 111 , 112 , 113 ],无论是单克隆抗体还是融合蛋白类抗VEGF药物,与3+PRN方案比较,3+T&E方案具有一定程度获益(2C)。
[推荐说明]
针对比较新生血管性AMD抗VEGF个性化治疗方案,采用循证医学方法共检索到5 022篇文献,指南共识专家组补充1篇文献,最终纳入系统评价1项,临床试验9项。基于循证医学证据,综合分析结果显示,与3+PRN方案比较,3+T&E方案在治疗1和2年时,BCVA较基线提高的平均值略高,注射给药次数平均增加2.79针(1年)和2.8针(2年)。3+T&E方案较3+PRN方案注射给药次数多2~3针,注射费用有一定增加,但在长期视力和形态学指标方面可表现出一定程度获益。在新生血管性AMD抗VEGF治疗中,相较于3+PRN方案,有条件推荐3+T&E方案。鉴于不同抗VEGF药物的推荐玻璃体腔注射给药最长间隔时间不同,采用3+T&E方案时须考虑合适的随访间隔时间。
3.新生血管性AMD抗VEGF药物初始3个月每月玻璃体腔注射给药1次(负载治疗)后无应答的处理建议:在临床实践中,并非所有新生血管性AMD对抗VEGF治疗反应良好,研究结果显示,30%患者治疗后无应答或疗效欠佳,视功能改善有限[ 114 ]。目前,对新生血管性AMD抗VEGF治疗应答的定义和分类尚未达成共识[ 115 ]。一般认为,积液量(IRF、SRF和CRT)或出血量与基线相比增加,和(或)BCVA与基线或治疗后最高BCVA相比丢失字母数>5个,为新生血管性AMD抗VEGF治疗无应答[ 116 ]。
[推荐意见5]
对一种抗VEGF药物的治疗应答不佳,可考虑更换其他抗VEGF药物。基于目前的循证医学证据[ 117 , 118 , 119 , 120 , 121 , 122 , 123 , 124 ],更换不同抗VEGF药物进行治疗,无明显获益也无明显风险。在临床实践中,针对抗VEGF三针负载治疗后无应答的新生血管性AMD,由临床医师综合考虑决定下一步治疗方案(2D)[ 117 ]。
[推荐说明]
采用循证医学方法共检索到5 452篇文献,最终纳入系统评价1项,临床试验8项(1项为RCT[ 117 ]、7项为观察性研究[ 118 , 119 , 120 , 121 , 122 , 123 , 124 ])。其中,RCT结果显示,更换不同抗VEGF药物治疗的患者BCVA较基线平均降低2.0个字母,继续维持原抗VEGF药物治疗的患者BCVA较基线平均提高0.5个字母(B),注射次数无明显差异(C);5项观察性研究结果表明[ 119 , 120 , 121 , 122 , 123 ],更换不同抗VEGF药物的患者BCVA较基线平均增加了0.26个字母(D)。对于抗VEGF三针负载治疗无应答的新生血管性AMD,更换不同抗VEGF药物后无明显获益,但也无明显风险。
4.新生血管性AMD持续性PED的处理建议:新生血管性AMD多伴有PED,PED被认为是新生血管性AMD严重程度、疾病进展以及对治疗抵抗的潜在标志。在临床实践中,新生血管性AMD抗VEGF治疗后,SRF、IRF往往相对易吸收,而PED的解剖结构改善往往相对有限。对于正在进行抗VEGF治疗的新生血管性AMD,若SRF、IRF等疾病活动性指标得到缓解,但存在持续性PED,是继续抗VEGF治疗还是停止治疗观察,是临床医师面临的问题。
[推荐意见6]
关于新生血管性AMD持续性PED目前仅有继续抗VEGF治疗的相关证据,在解剖学相关结局(如PED高度)方面有所改善,但不能排除是否为自然病程所致结果,且视力无明显获益(D)。因此,目前证据尚不能解决临床实践中存在的问题,还需要进行高质量研究,暂无法形成推荐意见[ 125 , 126 , 127 , 128 , 129 , 130 , 131 ]。
[推荐说明]
循证医学方法共检索到5 543篇文献,指南共识专家组补充7篇文献,最终纳入观察性研究7项[ 125 , 127 , 128 , 129 , 130 , 131 , 132 ]。研究结果显示,对于持续性PED,继续抗VEGF治疗1年,PED高度较基线平均降低45.89 μm(D)[ 125 , 129 , 130 , 131 , 132 ],BCVA较基线平均降低1个字母(D)[ 125 , 129 , 130 , 132 ]。现有文献中未见关键亚型PCV的相关证据。
5.新生血管性AMD非渗出性MNV的处理建议:近年来,随着OCTA的广泛应用,在AMD患者,尤其一只眼为进展期AMD患者的对侧眼中,常检测出黄斑区异常的新生血管血流信号,但此时患者尚无明显症状。针对这种OCTA发现MNV血流信号,但OCT显示不伴有积液(SRF和IRF)的非渗出性MNV,是否需要立即采用抗VEGF治疗是临床医师面临的问题。
[推荐意见7]
当OCT或OCTA发现新生血管性AMD非渗出性MNV时,建议密切观察(2D)。一旦发现新生血管具有活动性,出现积液、渗出或出血等,应及时采用抗VEGF治疗。
[推荐说明]
采用循证医学方法共检索到934篇文献,指南共识专家组补充11篇文献,最终纳入观察性研究6项[ 133 , 134 , 135 , 136 , 137 , 138 ]。由新生血管性AMD非渗出性MNV发展为渗出性MNV的比例在1年内为25%,在2年内为31%。由此可见,新生血管性AMD非渗出性MNV在短期内发展为渗出性MNV且患者出现明显视力下降的风险高,应建议患者注意视力变化并密切随访,一旦MNV出现活动性,则应采用抗VEGF治疗[ 133 , 134 , 135 , 136 , 137 , 139 , 140 , 141 , 142 , 143 , 144 , 145 ]。
(三)新生血管性AMD的激光治疗
1.视网膜激光光凝术:对于位于黄斑中心凹外的MNV,视网膜激光光凝术是可用的治疗方法之一。对于边界清晰的黄斑中心凹外MNV病灶,视网膜激光光凝术可防止2年内严重视力下降,但是约50%患者持续存在MNV病灶或复发。黄斑中心凹外MNV视网膜激光光凝术后5年,48%患眼视力下降30个字母及以上[ 146 , 147 ]。以往采用抗VEGF药物治疗新生血管性AMD的临床试验均针对黄斑中心凹下或中心凹旁MNV,未纳入黄斑中心凹外MNV,因此缺少针对黄斑中心凹外MNV抗VEGF治疗的循证医学证据。目前针对MNV位于黄斑中心凹外的新生血管性AMD,抗VEGF治疗或视网膜激光光凝术均是可采用的治疗方法。
2.PDT:既往研究结果证实,对于新生血管性AMD,抗VEGF治疗在改善视力和恢复解剖结构方面优于PDT[ 90 , 93 ]。对于新生血管性AMD中PCV亚型,可考虑行单纯抗VEGF治疗或抗VEGF治疗联合PDT(在患者无禁忌证和PDT可使用的情况下)。单纯抗VEGF治疗可有效改善PCV患者视功能,抗VEGF治疗联合PDT可减少抗VEGF治疗的次数[ 33 , 148 , 149 , 150 , 151 , 152 ]。
八、AMD的随访
(一)检查
调查病史和进行相关影像学检查是AMD随访的主要内容。随访病史应考虑以下几点:(1)症状,如视力下降和视物变形;(2)摄入的药物和营养补充剂;(3)疾病史,尤其眼科疾病史;(4)社会史,如吸烟等[ 40 ]。
随访应检查BCVA,并行Amsler方格表和眼底镜检查。根据临床发现和医师的判断进行OCT、OCTA和FFA或ICGA等后续检查,有助于检测疾病的活动性并监测疾病的进展。初始治疗和抗VEGF治疗应约每隔4周进行1次随访或根据给药方案决定[ 9 , 153 ]。告知患者治疗后若出现严重眼痛、眼红或视力下降等,应立即就诊,重新进行检查。
[推荐意见8]
AMD属于慢性疾病,需要长期观察和随访。鉴于FFA和ICGA为有创检查,不适宜多次反复使用。对于新生血管性AMD,考虑到OCTA检查在不同级别医院中的可行性可能存在差别,建议使用OCT联合OCTA进行随访观察[ 7 , 8 , 66 , 69 , 70 , 71 , 72 , 73 , 74 , 75 , 76 , 77 , 154 , 155 ]。
(二)对侧眼
1.对侧眼无MNV病灶:对于一只眼为新生血管性AMD而对侧眼无MNV的患者,对侧眼发展为进展期AMD的风险较高[ 156 ]。服用AREDS或AREDS2中的营养补充剂,10年内风险可降低36%[ 153 ]。告知患者即使在无症状的情况下,仍需监测视力并定期随访,在出现任何新的或明显的视觉症状时更应如此。具有极高风险的患者(如一只眼为进展期AMD,对侧眼存在大量玻璃膜疣)可增加检查频次(每6~12个月1次),以在可治疗阶段发现无症状MNV。同时,提示患者定期进行自我测试。此外,OCT和OCTA有助于评估高危对侧眼。
2.对侧眼有MNV病灶:对于一只眼已发展为进展期AMD的患者,若对侧眼发现非渗出性MNV,则对侧眼发展为渗出性MNV的可能性增大[ 5 , 136 ],尤其在第1年内,MNV面积每月可增长20%,更应注意转化为渗出性MNV[ 136 ]。此外,OCT和OCTA检查若发现黄斑区视网膜厚度增加、PED的宽度和高度增加、MNV面积增大以及有分支模式和病灶旁出现低密度晕,均预示非渗出性MNV可能向渗出性MNV转变,应密切关注,必要时及时给予治疗,避免视功能发生不可逆性损伤[ 157 ]。
九、总结
本指南是我国第1部严格遵循WHO指南制订规范和国际指南标准制订的基于循证医学证据的AMD诊断和治疗临床实践指南。指南指导委员会和指南共识专家组通过广泛调研和征集意见,确定了与AMD诊疗相关的8个临床关键问题。通过全面的文献检索和研究证据分析,结合患者的价值观和偏好,并充分考虑我国的国情和基层卫生医疗资源的可及性,最终形成针对AMD诊断和治疗的推荐意见,并对推荐意见进行了详细的解释和说明。本指南更新了对AMD病理生理及分型等的认识,涵盖了眼底影像学、治疗药物及其给药方案方面的最新进展,对于我国AMD的诊断、治疗和预防具有重要的指导意义。同时,指南工作组提示,眼科及相关领域的临床医师在使用本指南时,应接受相关培训,并结合当地的医疗条件和患者个体化因素具体分析和综合判断。
本指南由中华医学会眼科学分会眼底病学组、中国医师协会眼科医师分会眼底病学组与国家眼部疾病临床医学研究中心共同承担制订工作,由指南工作组分工完成。欢迎对本指南存在的不足提出宝贵的建议和意见,使得本指南能够不断更新和完善。
形成指南意见的专家组成员:(#示中华医学会眼科学分会眼底病学组委员,*示中国医师协会眼科医师分会眼底病学组委员)
指南指导委员会
首席临床专家:许迅#*(上海交通大学医学院附属第一人民医院眼科,中华医学会眼科学分会眼底病学组组长,中国医师协会眼科医师分会眼底病学组组长)、黎晓新(北京大学人民医院眼科,现在厦门大学厦门眼科中心,中华医学会眼科学分会眼底病学组前任组长)
首席方法学专家:夏君(宁波诺丁汉GRADE中心)
刘堃*(上海交通大学医学院附属第一人民医院眼科,执笔)
指南共识专家组(按姓氏拼音排序)
陈有信#*(中国医学科学院 北京协和医学院 北京协和医院眼科)、戴虹#*(北京医院眼科)、刘堃*(上海交通大学医学院附属第一人民医院眼科)、吕林#*(中山大学中山眼科中心)、苏冠方#*(吉林大学第二医院眼科医院)、孙晓东#*(上海交通大学医学院附属第一人民医院眼科)、唐罗生#*(中南大学湘雅二院眼科)、王雨生#*(解放军空军军医大学西京医院眼科)、魏文斌#*(首都医科大学附属北京同仁医院北京同仁眼科中心)、夏君(宁波诺丁汉GRADE中心)、徐格致#*(复旦大学附属眼耳鼻喉科医院眼科)、杨培增(重庆医科大学附属第一医院眼科)、赵明威#*(北京大学人民医院眼科)、赵培泉#*(上海交通大学医学院附属新华医院眼科)
指南外审专家组(按姓氏拼音排序)
常青*(复旦大学附属眼耳鼻喉科医院眼科)、陈蕾#(中国医科大学附属第一医院眼科)、陈松#*(天津眼科医院)、陈伟奇*(汕头大学·香港中文大学联合汕头国际眼科中心)、陈晓隆#*(中国医科大学盛京医院眼科)、崔彦#(山东大学齐鲁医院眼科)、方肖云#(浙江大学医学院附属第二医院眼科中心)、贺涛#(武汉大学人民医院眼科)、黄厚斌(解放军总医院眼科医学部)、姜春晖*(复旦大学眼耳鼻喉科医院眼科)、蒋沁*(南京医科大学眼科医院)、柯根杰#(安徽省立医院眼科)、李燕#*(昆明医科大学第一附属医院眼科)、李秋明#(郑州大学第一附属医院眼科)、李甦雁#(徐州市第一人民医院眼科)、李筱荣*(天津医科大学眼科医院)、梁建宏*(北京大学人民医院眼科)、梁小玲#(中山大学中山眼科中心 海南眼科医院)、刘静#(中国中医科学院望京医院眼科)、刘武*(首都医科大学附属北京同仁医院北京同仁眼科中心)、刘勇#(解放军陆军军医大学第一附属医院眼科)、刘庆淮*(南京医科大学第一附属医院眼科)、刘铁城#(解放军总医院眼科医学部)、刘晓玲*(温州医科大学附属眼视光医院)、刘早霞*(吉林大学第二医院眼科中心)、柳林*(上海交通大学医学院附属仁济医院眼科)、陆方*(四川大学华西医院眼科)、马翔#*(大连医科大学附属第一医院眼科)、曲进锋*(北京大学人民医院眼科)、佘海澄*(首都医科大学附属北京同仁医院北京同仁眼科中心)、沈丽君#*(温州医科大学附属眼视光医院)、沈玺*(上海交通大学医学院附属瑞金医院眼科)、宋艳萍#*(解放军中部战区总医院眼科)、宋宗明#(河南省立眼科医院)、孙大卫#(哈尔滨医科大学附属第二医院眼科)、孙旭芳*(华中科技大学同济医学院附属同济医院眼科)、万光明*(郑州大学第一附属医院眼科)、王方*(同济大学附属第十人民医院眼科)、王鲜#(贵州医科大学附属医院眼科)、王兴荣#(山东中医药大学附属眼科医院)、王艳玲*(首都医科大学附属北京友谊医院眼科)、魏勇*(温州医科大学附属眼视光医院)、文峰*(中山大学中山眼科中心)、肖云*(解放军第四七四医院眼科)、徐国兴#(福建医科大学附属第一医院眼科)、徐海峰#*(山东第一医科大学附属眼科研究所)、俞素勤*(上海交通大学医学院附属第一人民医院眼科)、喻晓兵*(北京医院眼科)、于旭辉#(哈尔滨医科大学附属第一医院眼科)、袁容娣#(解放军陆军军医大学第二附属医院眼科)、张风*(首都医科大学附属北京同仁医院北京同仁眼科中心)、张明#*(四川大学华西医院眼科)、张国明*(深圳市眼科医院)、张红兵*(西北大学第一附属医院眼科)、张美霞*(四川大学华西医院眼科)、张少冲*(深圳市眼科医院)、张喜梅*(山西省眼科医院)、张新媛#(首都医科大学附属北京同仁医院北京同仁眼科中心)、张学东#(重庆医科大学第一附属医院眼科)、赵博军*(山东第一医科大学附属省立医院眼科)、周琼*(南昌大学第一附属医院眼科)、朱丹#(内蒙古医科大学附属医院眼科)
指南学术秘书组
苏莉(上海交通大学医学院附属第一人民医院眼科,辅助执笔)、陈翀(上海交通大学医学院附属第一人民医院眼科)、杨晓璐(上海交通大学医学院附属第一人民医院眼科)、沈胤忱(上海交通大学医学院附属第一人民医院眼科)
指南证据评价组
齐方(上海道田循证科技有限公司)、苏莉(上海交通大学医学院附属第一人民医院眼科)、陈翀(上海交通大学医学院附属第一人民医院眼科,辅助执笔)、杨晓璐(上海交通大学医学院附属第一人民医院眼科)、沈胤忱(上海交通大学医学院附属第一人民医院眼科)、张阳(上海道田循证科技有限公司)、刘昭远(上海道田循证科技有限公司)、张文洁(上海道田循证科技有限公司)

- 星期四, 27 6月 2024
三种植物挥发油的化学成分、酪氨酸酶抑制能力及抗氧化活性的研究---三种植物精油抗氧化及蛋白质硝化作用的研究(四)
4.1 引言
皮肤是人体的主要器官之一。它覆盖全身,与人体其它器官密切相连,起着保护人体不受外部刺激或伤害的作用。人的皮肤从表面上来看是薄薄的一层,但如果把它放在显微镜下面仔细观察,就会清楚的看到皮肤由外及里共分为三层:皮肤的最外层叫表皮:中间一层叫真皮:最里面的一层叫皮下组织。表皮是皮肤的最外层包含各种大小不同的鳞片状上皮细胞,由基层发育而成。此基层位于真皮之上,在发育过程中不断的产生新细胞。表皮细胞还能够进一步细分为基底层、棘层、颗粒层、透明层和角质层。表皮细胞之间排列非常紧密,能够对一些化学物质和水分有屏障作用,因此能够保护真皮和皮下组织[1]。皮肤衰老的主要原因发生在真皮,真皮是皮肤的主要构成部分。真皮由弹力纤维、胶原纤维和网状纤维组成的结缔组织与纤维束间的无定型基质构成,真皮的厚度随身体部位功能的不同而异。皮肤衰老或者长期过度日晒会使皮肤产生皱纹、弹性松弛,是胶原纤维及弹力纤维变性或断裂的结果。
人体会在内源性或外源性因素的诱导下产生活性氧(ROS)和活性氨(RNS)。与此同时,人体自身防御系统能够清除细胞中的自由基。但是,随着年龄的增长和外界刺激如环境污染、紫外光照射和炎症条件下,自由基的产生会增加数倍[2]。自由基的产生和通过人体自身抗氧化系统的清除导致氧化应激[3],氧化应激会损伤很多生物分子,因而导致多种疾病的形成[4]。在这种情况下,通过外源性补充抗氧化剂来清除体内自由基就显得尤为重要[3]。在食品和化妆品领域,由于众多合成的抗氧化剂存在潜在的致癌性而让人们对天然的抗氧化剂的研究与应用越来越重视[6]。芳香植物,尤其是其挥发油是很好的天然抗氧化剂[7]。如今,人们致力于研究天然植物的挥发油,因为其相对安全、容易被消费者接受、在化妆品、食品、药品等领域应用广泛、容易获得并且相对廉价[8]。
紫外照射是黑色素形成的一一个关键因素[9],之前有研究证明了紫外照射诱导的ROS和RNS过量产生会使黑色素增多[10]。使用防晒霜是目前最流行的减少紫外线对皮肤损伤的方法[11]。纳米二氧化钛广泛应用于防晒产品中[12]。但是,最近有研究表明纳米二氧化钛促进含水环境中颗粒表面光诱导产生活性氧[13,14]。另一方面,在正常的阳光照射环境下,汗水的蒸发能够提高皮肤表面亚硝酸盐的量[15-17]。因此,由于紫外光的照射,纳米二氧化钛和亚硝酸盐会导致蛋白质氧化和酪氨酸硝化。蛋白质酪氨酸硝化不仅会引起蛋白质结构和功能的改变,而且会额外增加光引起的氧化损伤。因此,蛋白质氧化和酪氨酸硝化可以认为是纳米二氧化钛对皮肤的损伤。
本章通过三种不同抗氧化试验来研究三种挥发油的抗氧化活性,同时研究三种挥发油对UV-TiO2-NO2 诱导的蛋白质氧化和硝化的保护作用。
4.2材料与方法
4.2.1试剂与仪器
4.2.1.1主要试剂
2,4-二硝基苯肼(DNPH).牛血清蛋白( BSA)、二叔丁基对甲酚( Butylated hydroxytoluene, BHT)、兔多克隆抗二硝基苯酚抗体、兔多克隆抗3-硝基酪氨酸抗体:美国Sigma 公司;超氧阴离子自由基试剂盒:南京建成生物研究所;三羟甲基氨基甲烷(Tris)、2,4-二硝基苯肼( 2,4-dinitrophenylhydrazine, DNPH)、考马斯亮蓝R-250、十二烷基硫酸钠(SDS)、 吐温(Tween-20)、 考马斯亮蓝G-250、丽春红:美国Amersco公司;ECL发光试剂、辣根过氧化物酶标记的羊抗兔IG(H+L): 美国Pierce 公司;甲叉双丙烯酰胺、溴酚蓝、丙烯酰胺:瑞典Pharmacia公司;硝酸纤维素膜:美国Millipore 公司。
4.2.1.2主要仪器
SPECTR Amax PULS384型酶标仪:美国Sunnyvale公司;
DYCP-40C型电泳槽:北京六一-仪器厂;
Milli-Q Synthesis超纯水系统:国美Millipore 公司;
SSQ-H型不锈钢恒温水浴锅:上海三 申医疗器械有限公司;
DYY-7C型电泳仪:北京六一仪器厂;
UV7500型紫外-可见分光光度计:.上海 天美科学仪器有限公司;
X型胶片及感光暗盒:美国Kodak 公司;
4.2.1.3溶液的配置:
SDS-聚丙烯酰胺凝胶溶液的配制
电泳工作液:
①30%(w/v)丙烯酰胺单体储存液: 29.2 g丙烯酰胺,0.8 g双丙烯酰胺,溶于100 mL二次水中,储藏于棕色瓶中4C保存备用;
②1.5 M Tris-HCl (pH= >8.8):将36.34g Tris碱溶于150 mL二次水中,用浓盐酸调节pH值至8.8, 最后加二次水到总体积为200 mL,4C保存;
③1.0 M Tris-HCl (pH=6.8): 12.10g Tris 碱溶于50 mL二次水中,用浓盐酸调节pH值至6.8,最后加二次水到总体积为100mL,4C保存;
④10%过硫酸胺:使用小管分装,于-20°C 保存;
⑤5x电泳缓冲液: 15.1 gTris碱,94g甘氨酸,5g SDS 溶于1000 mL二次水中,室温条件下保存;
1x样品缓冲液(10 mL): 1.0mL甘油,1.25 mL Tris-HCl(0.5M,pH=6.8), 1.5mL 20% SDS(w/v), 0.5mLβ_巯基乙醇,2.0mL 0.1%溴酚蓝,3.75 mL二次水,4'C保存;
考马斯亮蓝染色液: 0.25g 考马斯亮蓝R-250, 112.5mL 甲醇,25 mL冰醋酸,然后加二次水定容至总体积1000 mL;
考马斯亮蓝脱色液:甲醇50 mL,冰醋酸50 mL,二次水400 mL。
Western blot所用溶液的配制:
半干转移缓冲液: 5.8g Tris碱,2.9g 甘氨酸,200 mL甲醇,0.37 gSDS,然后加二次水至总体积1000 mL;
TBS-T:8.77g氯化钠,3.15 g Tris-HCl溶于950 mL二次水中,然后用1M氢氧化钠溶液调节pH值至7.4, 最后加入0.5 mL Tween-20并补加二次水至总体积为1000mL, 4C保存;
封闭液: 5%脱脂奶粉( TBS-T溶解);
丽春红染色液: 3%三氯乙酸(w/v),0.2% 丽春红(w/v),3%磺基水杨酸(w/v);
4.2.2超氧阴离子清除实验
运用超氧阴离子自由基试剂盒检测样品对超氧阴离子自由基的清除能力。溶液的配置和样品的检测方法按照试剂盒说明书操作。槲皮素作为阳性对照。超氧阴离子清除率的计算方法:
抑制率%= (Ablamk -Asample)/AblankX 100 Aplamk和Asample 分别表示不添加实验样品和添加实验样品时的吸光度。
4.2.3 ABTS阳离子(ABTS*)清除实验
ABTS阳离子清除实验参照Re等[18] 和Gao等[19的方法。ABTS 溶解于蒸馏水,浓度为7mM。溶液中加入MnO2粉末并在黑暗环境下室温保存超过24小时,用注射器式过滤器过滤并在黑暗环境中放置6小时后使用。获得的ABTS 阳离子以这种形式在黑暗环境中室温保存超过2天。含有ABTS阳离子的母液用乙醇稀释至其吸光度值在734 nm波长下为0.70 (+0.02)。每种样品稀释至适当的浓度。100μL稀释的样品与1.2mL稀释的ABTS阳离子溶液反应,从反应开始到2分钟,记录分光光度计在734nm波长处的吸光度值。
自由基清除率% = (Ablank -Asample)AblankXx 100
其中Ablank代表没有添加实验样品时的吸光度值,Asample代表添加实验样品时的吸光度值。槲皮素作为阳性对照。
4.2.4脂质过氧化的测定
实验方法参照Mihara and Uchiyamal20]和Hermes-Lima等[21。 亚油酸作为抗脂质过氧化的底物。将0.2804g 的亚油酸、0.2840g 的吐温20、 50 mL磷酸缓冲溶液(pH7.0)混合为均匀的乳浊液。乳浊液现用现配,不可存储。200 μL样品溶解于DMSO,加入2mL亚油酸乳状液,然后加入氯化亚铁(100 μL,0.6 mmol/L, 溶剂为3.5%的盐酸)和过氧化氢(400 μL,25 mmol/L);对照组为2500 μL磷酸缓冲溶液和200 uL样品溶液。剧烈震荡后,反应混合液在37°C 静置60分钟;加入2.0mL 1%的TAB溶液(含有0.002% BHT, 0.8% TCA, 0.8% SDS)在95°C反应30分钟。过氧化值通过分光光度计在550nm波长处的吸光度值来体现。Trolox作为阳性对照。
脂质过氧化的抑制率% = (Ablank-Asample)/ AblankX 100
其中Ablank表示未添加实验样品的吸光度值,Asample表示添加了实验样品的吸光度值。
4.2.5纳米TiO2- NO2 -UV诱导的蛋白质氧化和酪氨酸硝化测定
实验方法参照本实验室之前的方法[21并做略微修改。BSA(1.0mg/mL),NaNO2 (1.0 mmol/L)和悬浮的TiO2(50μg/mL) 与pH7.0的0.1 mol/L PBS充分混合(总体积3 mL)。混合液移入24孔板直接暴露在光源下。365 nm波长的紫外光照射时反应开始。365 nm波长紫外光照射4小时,10000 转/分钟离心15 分钟去除TiO2,上清液备用。
4.2.5.1蛋白质氧化测定
取处理好的.上清液100 μL,加入100μL含3%SDS的10 mmol/L DNPH,室温下反应45分钟(每隔几分钟使用漩涡仪充分混匀),冰浴下加入200 μL的中和液(2 mol/L Tris, 30%甘油)终止反应。然后样品与280μL的2x.上样缓冲液,混匀后于-20 C储存备用。进行10% SDS-PAGE。电泳完毕后,运用半干转移法将蛋白质转移到硝酸纤维素膜上,在室温条件下将印迹膜放入封闭液(5%脱脂奶粉)中搅动孵育1.5 小时。孵育完毕后,用TBS-T漂洗4次,每次10分钟。然后用兔多克隆抗3-DNP抗体(1: 4000 )孵育印迹膜(4 C,1.5 小时),接着继续用TBS-T漂洗4次,每次10分钟;然后室温下用辣根过氧化物酶标记的羊抗兔IgG (二抗,1: 4000) 孵育印迹膜1小时,再用TBS-T溶液漂洗5次,每次10分钟。最后采用化学发光法检测。
4.2.5.2蛋白质硝化的测定
150 μL.上清液与150 ul 2x.上样缓冲液混匀后于100 °C沸水中反应3分钟,进行10% SDS-PAGE。
SDS-聚丙烯酞胺凝胶电泳:在12% SDS -聚丙烯酰胺凝胶电泳中进行分离。
蛋白印迹:电泳完成以后,利用半干转移法将蛋白质转移到硝酸纤维素膜上,在室温条件下将印迹膜放入封闭液(5%脱脂奶粉)中孵育1.5 小时。孵育完毕后, TBS-T溶液漂洗4次,每次10分钟。然后用兔多克隆抗3-硝基酪氨酸抗体(一抗,1:800) 室温条件下孵育印迹膜1.5 小时,TBS-T溶液漂洗4次,每次10分钟;然后用辣根过氧化物酶标记的羊抗兔IgG( 二抗,1:3000) 室温条件下孵育印迹膜1小时,然后再用TBS-T溶液漂洗4次,每次10分钟。最后用化学发光法检测。
4.2.6数据统计
所有实验结果均至少重复3次,实验结果以X士SD来表示,差异显著性分析采用组间t检验法。p<0.05, 认为两组数据间有显著差异; p<0.01, 认为两组数据间有非常显著性差异。
4.3试验结果
4.3.1山苍子油及其活性成分对ABTS*的清除能力测定
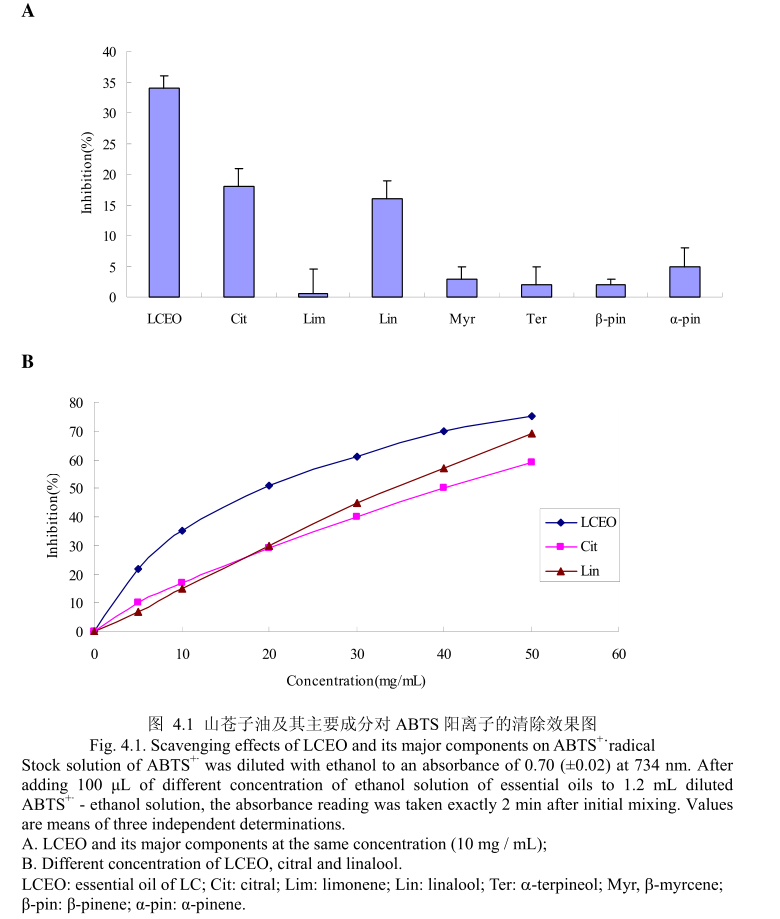
ROS在调节角蛋白细胞和黑素细胞增殖方面有重要作用,同时在调节黑素细胞生成黑色素方面也有重要作用。而能够清除ROS和抑制ROS产生的物质如抗氧化剂,能够减少色素沉着或者阻止紫外线诱导的黑素生成[23,24]。为了测定LCEO和其主要成分是否具有抗氧化活性,通过清除ABTS+来测定。LCEO和其主要成分对ABTS+的清除能力如图4.1 (A)。 LCEO在浓度为10mg/mL时被证明具有很强的抑制ABTS+产生的能力,柠檬醛和芳樟醇在相同浓度下表现出一定的抑制能力,柠檬烯、β-月桂烯、a-松油醇、β-蒎烯、a-蒎烯在该浓度下表现出的抑制活性可以忽略不计。结果表明柠檬醛和芳樟醇是LCEO中清除ABTS+的活性成分。如图4.1 (B),进一步测定了不同浓度下的LCEO和其活性成分对ABTS+的清除能力。从图中可以看出,ABTS+的清除能力与使用剂量相关。各种成分的ICso 的值按照逐渐递减的顺序为:柠檬醛>芳樟醇>
LCEO。从而证明LCEO比另外两种活性成分有着更强的清除ABTS+ 的能力。 将LCEO对ABTS+ 的清除能力与槲皮素比较,LCEO的半抑制浓度为17.75+0.89mg/ mL,低于槲皮素的半抑制浓度为4.5+0.9 ug / mL。
4.3.2 山苍子油及其活性成分对 0-·的清除能力测定

山苍子油及其活性成分对〇的清除能力测定如图4.2(A)所示,在浓度为5mg/mL 的情况下,柠檬醛和LCEO对O的抑制率分别为37%和 28%,而其它组分在相同的浓度下表现出的抑制能力在5%-15%之间。证明LCEO 具有一定的清除 O,的能力,其主要活性成分为柠檬醛。如图4.2(B)所示,当LCEO 和柠檬醛的浓度从 2.5mg/mL增加到20mg/mL 时,LCEO 和柠檬醛对 O的清除活性增加。而且,LCEO 和柠醛表现出相似的清除能力。将LCEO的抗氧化能力与槲皮素作比较,LCEO对0的半抑制浓度为10.2+0.12mg/m,而皮素的半抑制浓度为 10.3+0.4μg/m。结果表明皮素的抗氧化能力强于 LCEO。
4.3.3 LCEO 和柠檬醛对 UV-TiO,-NO,催化的蛋白质氧化损伤的保护
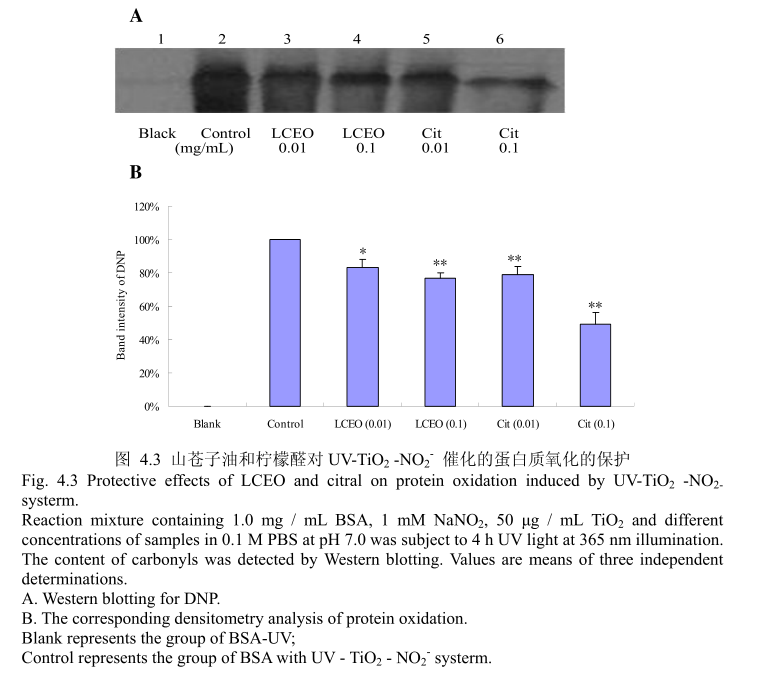
蛋白质氧化是对蛋白质的氧化修饰,改变了蛋白质的结构和功能。蛋白质的氧化常常存在于生理和病理状态下。因此,蛋白质氧化可能存在于纳米TO,对皮肤的毒性过程中。实验使用牛血清蛋白(BSA)作为模型蛋白,然后用SDS-PAGE和蛋白质印迹法检测。如图4.3(A)和(B),蛋白质氧化通过添加0.01mg/mL(最低浓度)的LCEO或柠檬醛被抑制。与此同时,所有的样品都具有较强的保护作用,并且明显呈剂量相关性。当LCEO或柠醛的浓度达到0.1mg/m时,表现出的抑制蛋白质氧化的能力更强。此外,在相同的浓度条件下,柠檬醛比LCEO 表现出更强的抑制蛋白质氧化的能力。
4.3.4LCEO 和柠檬醛对 UV-TiOz-NO,催化的蛋白质硝化损伤的保护
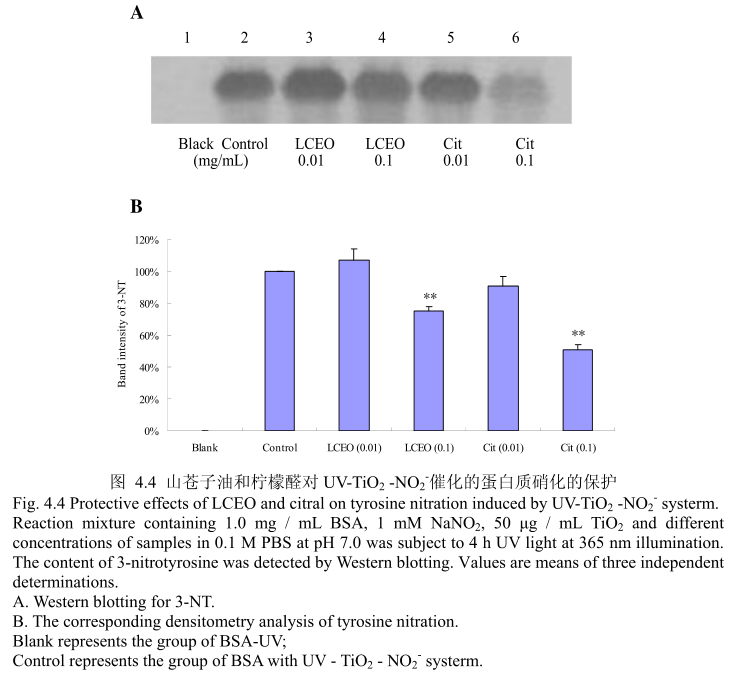
蛋白质硝化是机体在氮氧化物存在的条件下氧化损伤的特殊形式,主要是指蛋白质中含有的酪氨酸残基被硝化成3-硝基酪氨酸(3-Nitro-Tytosine, 3~NT),即一个硝基(-NO2)添加在酪氨酸残基的羟基邻位上。蛋白质硝化在病理状态下常伴随着活性氮和活性氧的增加而产生。目前,蛋白质酪氨酸硝化已经被确认为是一-种重要的蛋白质翻译后的修饰,并且与炎症和神经退行性疾病、心血管疾病等多种病症密切相关,其产物3-硝基酪氨酸(3-NT) 作为NO、ONOO~等活性氮的衍生物,可以被认为是许多生理和病理状态下的生物标志物(Biomarker)[5]126。将3-硝基酪氨酸作为酪氨酸硝化的检测指标,LCEO和柠檬醛对蛋白质硝化的抑制效果如图4.4 (A)和(B)。当LCEO或柠檬醛的的浓度为0.01 mg/mL时,并没有表现出较强的抑制蛋白质硝化的能力,当LCEO 或柠檬醛的浓度达到0.1 mg/ mL时,才能表现出较强的蛋白质硝化的抑制活性。
4.3.5丁香花蕾油及其主要成分对O2的清除能力测定
超氧阴离子作为更多活性氧的前体对细胞结构有着很大的损伤,导致组织损伤和不同的疾病[26]。
丁香花蕾油和其主要成分丁香酚对O2” 的清除活性如图4.5。结果表明丁香花蕾油的比丁香酚表现出更强的清除O2”的能力。丁香花蕾油的浓度分别为10ug/mL、30 ug/mL、60μg/mL时,超氧阴离子的清除能力为29.8%, 41.5%,50.5%,而对于相同浓度的丁香酚,其对超氧阴离子的清除能力分别为20.4%, 25.3%,30.8%。当丁香酚或丁香花蕾油的量增加时,抑制能力并没有明显的变化。这可能是由于其在水中的溶解性较低的缘故,当溶解到一定量时,增加的量并不能溶解于测试溶剂,从而不能发挥抑制作用。丁香花蕾油的对超氧阴离子的半抑制浓度为58ug/mL,低于槲皮素的半抑制浓度为10.3 ug / mL。

4.3.6 丁香花蕾油及其主要成分对 ABTS*的清除能力测定
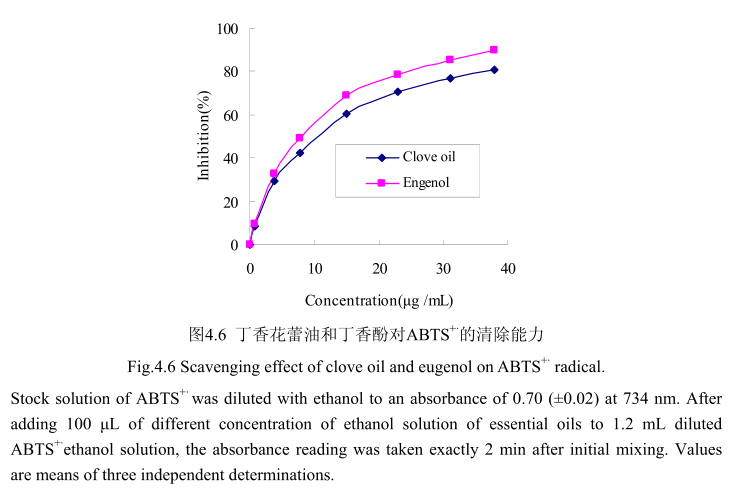
丁香花蕾油和其主要成分丁香酚对ABTS+的清除活性如图4.6 所示。丁香花蕾油和丁香酚都表现出较高的清除活性。当丁香花蕾油的浓度为0.8-38μg/mL时,其清除活性为8.7%-80.9%, 在相同浓度范围内,丁香酚的清除率为9.7%-89.6%。当丁香花蕾油的浓度从0μg/mL逐渐增加到15μg/mL时,对ABTS+的清除率急剧增加(从0增加到70%左右);当丁香酚的浓度从0μg/mL逐渐增加到15μg/ mL时,对ABTS+的清除率亦明显增加(从0增加到60%左右)。当丁香花蕾油的浓度从15 ug/mL逐渐增加到40 ug/mL时,对ABTS+的清除率增加量逐渐变缓(从70%增加到89.6%);当J香酚的浓度从15 ug/ mL逐渐增加到40μg/mL时,对ABTS+的清除率从60%增加到79%。丁香花蕾油和丁香酚的半抑制率分别为8.5 μug/ mL和7.7 ug/ mL,与槲皮素的半抑制浓度4.5 ug/ mL相比差别不大。
4.3.7香茅油及其主要成分对O2-.的清除能力测定
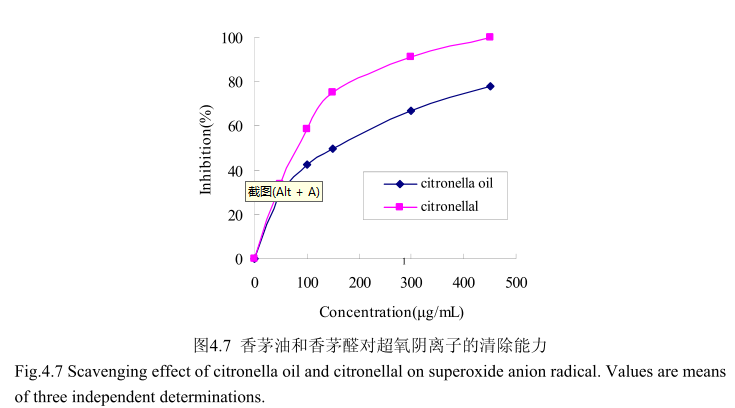
香茅油及其主要成分香茅醛对超氧阴离子的清除活性如图4.7所示。香茅油的半抑制浓度(ICso:150μg/mL)大于香茅醛的半抑制浓度(ICso:90μg/mL),说明香茅油对超氧阴离子的抑制活性弱于香茅醛。当香茅醛的浓度为450mg/m时,其对超氧阴离子的清除活性达到100%,而香茅油在该浓度下的清除活性仅为78%。香茅油对超氧阴离子的半抑制浓度为150mg/mL,说明其对超氧阴离子的清除能力弱于槲皮素(10.3μg/mL)。当香茅油的浓度从0g/m增加到50μg/m时,对超氧阴离子的抑制能力显著增加,随着香茅油的浓度逐渐增大,对超氧阴离子的清除能力的增加量逐渐变缓。当香茅醛的浓度0mg/m增加到150mg/m时,对超氧阴离子的清除能力显著增加(从0增加到78%左右),而当香茅醛的浓度从150g/m增加到500μg/m 时,清除能力增加的较为缓慢(从78%增加到 100%)。
4.3.8 香茅油及其主要成分对 ABTS*的清除能力测定
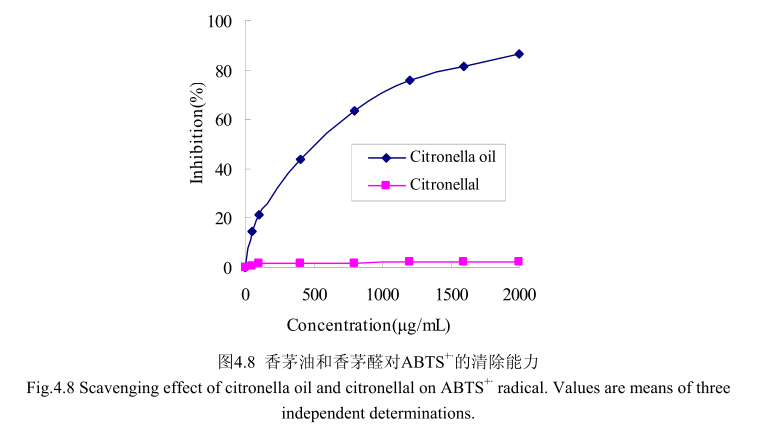
如图4.8所示,当香茅油的浓度范围在50-2000g/m时,其对 ABTS”的清除率为 14.5%-86.4%。尽管香茅油在低浓度时100g/m 时的抑制率仅为20%,但是香茅油的浓度从0g/m增加到100gm时,对ABTS*的清除能力显著增加;随着香茅油的浓度从100g/mL增加到2000g/mL时,对ABTS*的清除能力缓慢增加,且增加趋势逐渐变缓。而香茅油的主要成分香茅醛在相同的浓度条件下并没有表现出清除能力。而香茅油半抑制浓度为500g/m,远远大于皮素 4.5μg/m,从而说明香茅油的抗氧化活性较弱,
4.3.9丁香花蕾油和香茅油对脂质过氧化的保护作用
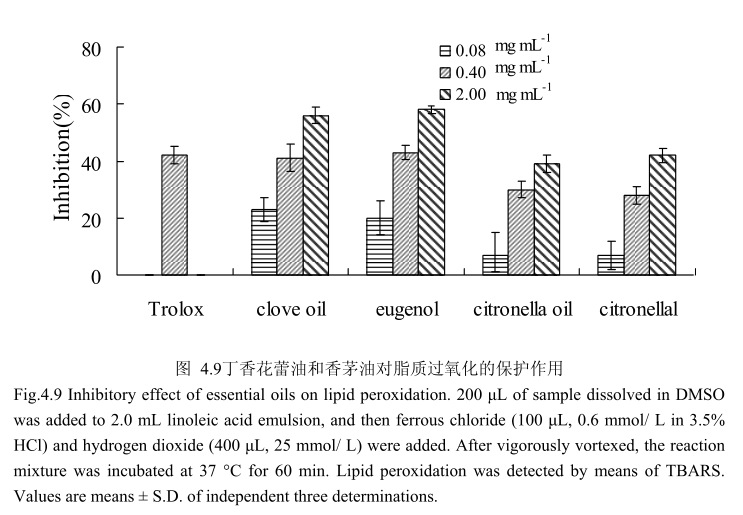
丁香花蕾油和香茅油及其主要成分对脂质过氧化的抑制作用如图4.9所示,丁香花蕾油、香茅油、丁香酚、香茅醛都具有抗脂质过氧化的作用,并且随着剂量的增加,抗氧化活性逐渐增强。在相同的浓度条件下,丁香花蕾油和丁香酚的抗氧化能力强于香茅油和香茅醛。当浓度为0.4mg/m时,丁香花蕾油和丁香酚抗脂质过氧化的能力与 Trolox(阳性对照)相似。
4.3.10 丁香花蕾油和香茅油对 UV-TiO,-NO,催化的蛋白质氧化损伤的保护
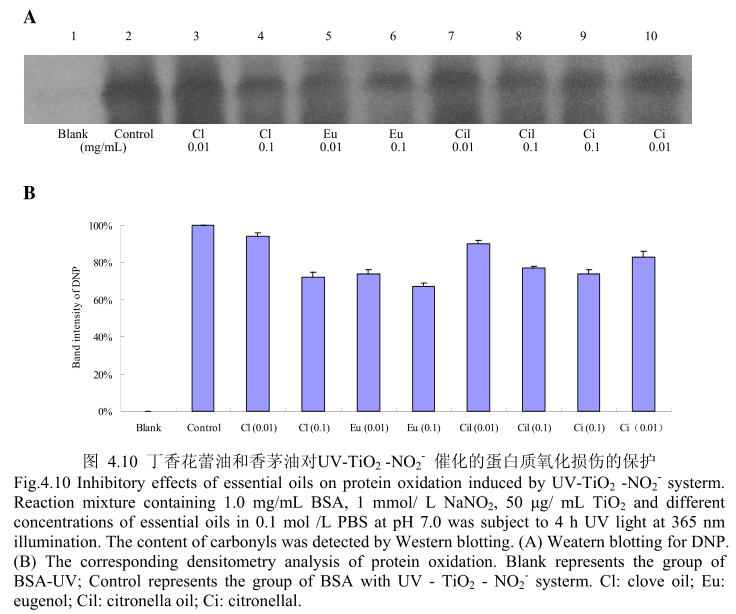
丁香花蕾油和香茅油对 UV-TiO2 -NO,催化的蛋白质氧化的抑制作用如图4.10A 和 B所示,当丁香花蕾油、丁香酚、香茅油、香茅醛以最低浓度0.01mg/ml 进行加样时,都具有抑制蛋白质氧化的能力。在该浓度下,丁香花蕾油和香茅油表现出相似的抑制蛋白质氧化的能力,丁香酚的抑制蛋白质氧化的能力强于丁香花蕾油,香茅醛的抑制蛋白质氧化的能力强于香茅油,丁香酚的抑制蛋白质氧化的能力强于香茅醛。当加样浓度增加到0.1mg/m 时,丁香花蕾油、丁香酚、香茅油、香茅醛均具有较好的抗氧化能力。在该浓度下,丁香花蕾油、香茅油、香茅醛表现出相似的抑制蛋白质氧化的能力,但在该浓度下其抗氧化活性弱于丁香酚。
4.3.11 丁香花蕾油和香茅油对 UV-TiO,-NO,催化的蛋白质硝化损伤的保护
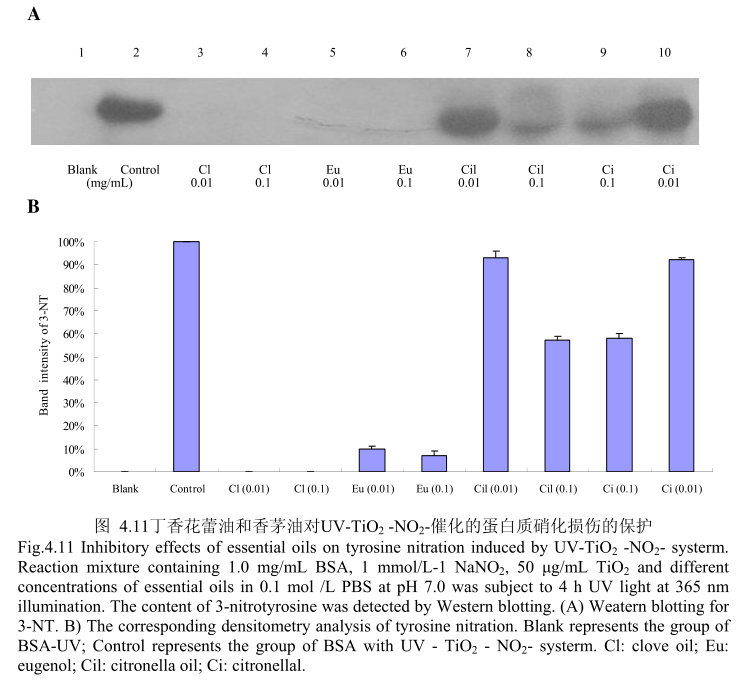
丁香花蕾油和香茅油对UV-TiO2-NO,催化的蛋白质硝化的抑制作用如图4.11,当丁香花蕾油的浓度为0.01mg/m和0.1mg/m 时,均能够完全抑制硝化的产生。而香茅油和其主要成分香茅醛在浓度为0.01mg/m时,几乎没有抑制蛋白质硝化的能力,当香茅油和香茅醛的浓度为0.1mg/mL时,表现出一定的抑制蛋白质硝化的能力。
4.4讨论
挥发油是芳香植物的次生代谢产物,有着明显的气味,是具有挥发性的混合物。在自然界,挥发油在保护植物方面有着重要作用,如抗病毒、抗细菌、杀灭昆虫和减少昆虫食用植物的欲望。目前已经发现大约3000 种挥发油,而其中有300种具有重要的商业价值,被用于制药、农业、食品、卫生、化妆品和香料领域。很多挥发油同时也是天然的抗氧化剂,如薄荷油[27-29]、迷迭香油[30-33]、鼠尾草油[34]、芫荽子油[27,29]、小茴香油[35]、百里香油[36]等。挥发油能够作为香精的原料加入到化妆品中,同时也可以作为天然防腐剂或者活性成分用于化妆中。此外,挥发油常常与其它植物油脂按照适当的比例调配后直接涂抹于皮肤,不仅能够放松神经,还能发挥挥发油特有的功效。因此,研究出一-些具有特殊功效的挥发油具有重要意义。
皮肤是人体抵御损伤的屏障,是将人体与外界环境隔开的重要屏障。持续的暴露在紫外光下会导致皮肤损伤相关的众多并发症,当紫外光引起的损伤超过人体黑.色素提供的保护能力时就会形成晒斑[37,38]。系外线诱导皮肤光损伤,导致皮肤的细胞基质发生改变,引起皱纹、皮肤松弛、粗糙、色素沉着、表皮增厚和结缔组织变化[39,40]。结缔组织各组分( 包括胶原、蛋白聚糖类、糖蛋白类)之间的平衡被打破
会导致不利影响,如表皮成纤维细胞光老化。皮肤自身具有抗氧化防御能力,能够清除包含自由基在内的活性氧,但是如果紫外光达到一定的强度时会超出这些防御系统的清除能力,从而导致自由基损伤细胞的组分,如蛋白质、脂类和DNA[41.42]。活性氧诱导的氧化应激能够最终导致细胞凋亡或细胞坏死[43]。活性氧在人体内的积累,在人体皮肤内源性损伤和光老化方面起着决定性作用,同时与皮肤炎症和皮肤癌有着密切的关系[44,45]。本章通过体外实验研究了丁香花蕾油、山苍子油、香茅油对自由基的清除能力。通过实验发现,LCEO在浓度为10 mg 1 mL时被证明具有很强的抑制ABTS阳离子产生的能力,柠檬醛和芳樟醇在相同浓度下表现出一定的抑制能力,柠檬烯、β-月桂烯、a-松油醇、β-蒎烯、a-蒎烯在该浓度下表现出的抑制活性可以忽略不计。LCEO对ABTS阳离子的半抑制浓度为17.75+0.89mg/ mL。在浓度为5mg/mL 的情况下,柠檬醛和LCEO对O2~ 的抑制率分别为37%和28%,而其他组分在相同的浓度下表现出的抑制能力在5%-15%之间。
LCEO对02”的半抑制浓度为10.2+0.12mg1mL。当香茅油的浓度范围在50-2000 μg / mL时,其对ABTS+的清除率为14.5%-86.4%。 从而说明香茅油对ABTS+的清除能力较弱。香茅油对超氧阴离子的半抑制浓度为150 ug/mL。丁香花蕾油和丁香酚都表现出较高的清除活性。当丁香花蕾油的浓度为0.8-38μg/mL时,其清除活性为8.7%-80.9%, 在相同浓度范围内,丁香酚的清除率为9.7%-89.6%。丁香花蕾油和丁香酚的半抑制率分别为8.5 μg/mL和7.7 μg/ mL。丁香花蕾油的浓度为10 ug/mL、30 μg/mL、60 μg/ mL时,超氧阴离子的清除能力为29.8%, 41.5%, 50.5%, 而对于相同浓度的丁香酚,其对超氧阴离子的清除能力分别为20.4%, 25.3%, 30.8%。丁香花蕾油的对超氧阴离子的半抑制浓度为58 ug. / mL。三种挥发油中丁香花蕾油对ABTS阳离子的清除能力最强,而其主要成分丁香酚对ABTS阳离子的清除能力更强,从而说明丁香花蕾油及其主要成分丁香酚有较强的抗氧化能力,与相关文献报道一致[46,47]。 而山苍子油对超氧阴离子的清除能力最强,说明山苍子油也具有较强的抗氧化能力。在脂质过氧化的抑制作用方面,丁香花蕾油、香茅油、丁香酚、香茅醛都具有抗脂质过氧化的作用,并且随着剂量的增加,抗氧化活性逐渐增强。丁香花蕾油和丁香酚的抗氧化能力强于香茅油和香茅醛。而山苍子油几乎没有抗脂质过氧化的能力。
蛋白质硝化是蛋白质氧化的一一种特殊形式,两者都是非常重要的蛋白质翻译后修饰,它们对蛋白质的功能产生非常重要的影响。而纳米二氧化钛在防晒产品中的广泛应用,紫外线的照射和皮肤表面汗液蒸发产生的亚硝酸盐为蛋白质的氧化和酪氨酸的硝化提供了充足的条件。本章研究了山苍子油、香茅油、丁香花蕾油对UVTiO2 - NO2催化的蛋白质硝化和蛋白质氧化的抑制作用,发现当LCEO或柠檬醛的浓度为0.01mg/mL时能够抑制蛋白质氧化,柠檬醛的抑制蛋白质氧化的能力强于LCEO,并且抑制能力呈剂量相关性。而对于抑制蛋白质的硝化,仅当LCEO和柠檬醛的浓度达到0.1 mg/ mL时才表现出较强的抑制蛋白质硝化的能力。当丁香花蕾油、丁香酚、香茅油、香茅醛以最低浓度0.01 mg / mL进行加样时,都具有抑制蛋白质氧化的能力。当加样浓度增加到0.1 mg/mL时,每种样品均具有较好的抗氧化能力。丁香花蕾油、香茅油、香茅醛表现出相似的保护作用,但在相同浓度下其抗氧化活性弱于丁香酚。对于蛋白质硝化的抑制作用方面,当丁香花蕾油和丁香酚的浓度为0.01mg/m时,能够完全抑制硝化的产生。而香茅油和其主要成分香茅醛仅在高浓度0.1mg/m 时,表现出一定的抑制蛋白质硝化的能力。
4.5 本章小结
在本章中,通过山苍子油、香茅油、丁香花蕾油体外清除ABTS和超氧阴离子实验,研究三种精油的抗氧化能力。我们发现丁香花蕾油及其主要成分丁香酚具有较强的清除ABTS*的能力,山苍子油和其主要成分柠檬醛具有较强的清除超氧阴离子的能力。丁香花蕾油、香茅油、丁香酚、香茅醛都具有抗脂质过氧化的作用,并且随着剂量的增加,抗氧化活性逐渐增强。丁香花蕾油和丁香酚的抗氧化能力强于香茅油和香茅醛。而山苍子油几乎没有抗脂质过氧化的能力。丁香花蕾油、丁香酚、香茅油、香茅醛、山苍子油、柠檬醛均具有较强的抑制蛋白质氧化的能力,其中丁香酚的抑制蛋白质氧化的能力最强。丁香花蕾油和丁香酚具有很强的抑制酪氨酸硝化的能力,山苍子油、柠檬醛、香茅油、香茅醛仅在较高浓度时表现出较强的抑制蛋白质硝化的能力。
4.6参考文献
[1] 涂国荣,张利兴,苏昆.自由基与皮肤衰老的关系及天然抗衰老植物在化妆品中的应用,日用化学品科学,1999,8:82-85
[2] Singh HP, Mittal S, Kaur S, et al. Characterization and antioxidant activity of essential oils from fresh and decaying leaves of Eucalyptus tereticornis. Journal of Agricultural and Food Chemistry, 2009, 57(15):6962-6966
[3] Edris AE. Pharmaceutical and therapeutic potentials of essential oils and their individual volatile constituents: a review. Phytotherapy Research, 2007, 21(4):308-323
[4]LuN,LiX,Li
J. Ntrative and oxidative modifications of enolase are
associated with iron in iron-overload rats and in vitro. Journal of Biological
Inorganic Chemistry, 2011, 16(3):481-490
[5] Aidi Wannes W, Mhamdi B, Sriti J, et al. Antioxidant activities of the essential
oils and methanol extracts from myrtle (Myrtus communis var. italica L.) leaf,
stem and flower. Food and Chemical Toxicology, 2010, 48(5):1362-1370
[6] Kilani S, Ledauphin J, Bouhlel I, et al. Comparative study of Cyperus rotundus essential oil by a modified GC/MS analysis method. Evaluation of its antioxidant, cytotoxic, and apoptotic effects. Chemistry & Biodiversity, 2008, 5(5):729-742
[7] Mechergui K, Coelho JA, Serra MC, et al. Essential oils of Origanum vulgare L. subsp. glandulosum (Desf.) letswaart from Tunisia: chemical composition and antioxidant activity. Journal of the Science of Food and Agriculture, 2010, 90(10):1745-1749
[8] Sutthanont N, Choochote W, Tuetun B. Chemical composition and larvicidal activity of edible plant-derived essential oils against the pyrethroid-susceptible and -resistant strains of Aedes aegypit(Diptera:Culicidae). Journal of Vector Ecology, 2010, 35:106-115
[9] Panich U, Kongtaphan K, Onkoksoong T. Modulation of antioxidant defense by Alpinia galangal and curcuma aromatica extracts correlates with their inhibition of UVA-induced melanogenesis. Cell Biology Toxicology, 2010, 26:103-116
[10] Panich U, Tangsupa a-nan V, Onkoksoong T, et al. Inhibition of UV A -mediated melanogenesis by ascorbic acid through modulation of antioxidant defense and nitric oxide system. Archives of Pharmacal Research, 201 1, 34(5):811-820
[11] Burnett ME, Wang SQ. Current sunscreen controversies: a critical review.
Photodermatology, photoimmunology & photomedicine, 2011, 27(2):58-67
[12] Tyner K, Wokovich A, Godar D, et al. The state of nano-sized titanium dioxide
(TiO2) may affect sunscreen performance. International Journal of Cosmetic Science, 201 1,33(3):234-244
[13] Kiss B, Biro T, Czifra G, et al. Investigation of micronized titanium dioxide penetration in human skin xenografts and its effect on cellular functions of human skin-derived cells. Experimental dermatology, 2008, 17(8):659-667
[14] Shen B, Scaiano,English A. Zeolite encapsulation decreases TiO2-photosensitized ROS generation in cultured human skin fibroblastst. Photochemistry and Photobiology, 2006, 82(1): 5-12
[15] Paunel AN, Dejam A, Thelen S, et al. Enzyme-independent nitric oxide formation during UVA challenge of human skin: characterization, molecular sources, and mechanisms. Free Radical Biology and Medicine, 2005, 38(5):606-615
[16] Oplander C, Cortese M, Korth H. The impact of nitrite and antioxidants on ultraviolet-A-induced cell death of human skin fibroblasts. Free Radical Biology Medicine, 2007, 43(5):8 18-829
[17] Weller R, Pattullo S, Smith L, et al. Nitric oxide is generated on the skin surface by reduction of sweat nitrate. Journal of Investigative Dermatology, 1996, 107(3):327-331.
[18] Re R, Pellegrini N, Proteggente A, et al. Antioxidant activity applying an improved ABTS radical cation decolorization assay. Free Radical Biology Medicine, 1999, 26(9-10):1231-1237
[19] Gao Z, Xu H, Chen X, et al. Antioxidant status and mineral contents in tissues of rutin and baicalin fed rats. Life Sciences, 2003, 73( 12):1599- 1607
[20] Mihara M, Uchiyama M. Determination of malonaldehyde precursor in tissues by thio barbituric acid test. Analytical Biochemistry, 1978, 86(1):271-278
[21] Hermes-Lima M, Willmore WG, Storey K B. Quantification of lipid peroxidation in tissue extracts based on Fe (II) xylenol orange complex formation. Free Radical Biology and Medicine, 1995,19(3):271-280
[22] Lu N, Zhu Z, Zhao X, et al. Nano titanium dioxide photocatalytic protein tyrosine nitration: A potential hazard of TiO2 on skin. Biochemical and Biophysical
Research Communications, 2008, 370(4):675-680
[23] Sapkota K, Park SE, Kim JE, et al. Antioxidant and anti melanogenic properties of chestnut flower extract. Bioscience, Biotechnology, and Biochemistry, 2010,
74(8):1527-1533
[24] Khazaeli P, Goldoozian
R, Shariffar F. An evaluation of extracts of five
traditional medicinal plants from Iran on the inhibition of mushroom tyrosinase
activity and scavenging of free radicals. International Journal of Cosmetic
Science, 2009, 31(5):375-381
[25] Beal MF. Oxidatively modified proteins in aging and disease. Free Radical Biology and Medicine, 2002, 32(9):797-803
[26] Gutteridge J, Richmond R, Halliwell B. Oxygen free-radicals and lipid peroxidation: Inhibition by theprotein caeruloplasmin. FEBS letters, 1980, 112(1): 269-272
[27] Lagouri V, Blekas G, Tsimidou M, et al. Composition and antioxidant activity of essential oils from oregano plants grown wild in Greece. Zeit schrift fir Lebensmitteluntersuchung und Forschung A, 1993, 197(1):20-23
[28] Lagouri V, Boskou D. Screening for antioxidant activity of essential oils obtained from spices. Developments in Food Science, 1995, 37(1):869-879
[29] Baratta MT, Dorman HJD, Deans SG, et al. Chemical composition, antimicrobial and antioxidative activity of laurel, sage, rosemary, oregano and coriander essential oils. Journal of Essential Oil Research, 1998, 10(6):618-627
[30] Farag R, Badei AZMA, Hewedi F, et al. Antioxidant activity of some spice essential oils on linoleic acid oxidation in aqueous media. Journal of the American Oil Chemists' Society, 1989, 66(6):792-799
[31] Maestri DM, Zygadlo JA, Lamarque AL, et al. Effect of some essential oils on oxidative stability of peanut oil. Grasas y aceites, 1996, 47(6):397-400
[32] Dang M, Takacsova M, Nguyen D, et al. Antioxidant activity of essential oils from various spices. Food/Nahrung, 2001, 45(1):64-66
[33] Saricoban C,Ozcan M. Antioxidative activity of rosemary (Rosmarinus officinalis L.) and sage (Salvia fruticosa L.) essential oils in chicken fat. Journal of Essential Oil Bearing Plants, 2004, 7(1):91-95
[34] Tepe B, Daferera D, Sokmen A. Antimicrobial and antioxidant activities of the essential oil and various extracts of Salvia tomentosa Miller (Lamiaceae). Food Chemistry, 2005, 90(3):333- -340
[35] Farag R, Ali M, Taha S. Use of some essential oils as natural preservatives for butter. Journal of the American Oil Chemists Society, 1990, 67(3):188-191
[36] Jukic M, Milos M. Catalytic oxidation and antioxidant properties of thyme essential oils (Thymus vulgare L). Croatica Chemical Acta, 2005,78(1):105-110
[37] Agar NS, Halliday GM, Barnetson RSC, et al. The basal layer in human squamous tumors harbors more UVA than UVB fingerprint mutations: a role for UVA in human skin carcinogenesis. Proceedings of the National Academy of Sciences of the United States of America, 2004, 101(14):4954-4959
[38] Ryu BM, Qian ZJ, Kim MM, et al. Anti-photoaging activity and inhibition of matrix metalloproteinase (MMP) by marine red alga, Corallina pilulifera methanol extract. Radiation Physics and Chemistry, 2009, 78(2):98- 105
[39] Kondo S. The roles of cytokines in photoaging. Jourmal of Dermatological Science, 2000, 23(1):30-36
[40] Rittie L, Fisher GJ. UV-light-induced signal cascades and skin aging. Ageing Research Reviews, 2002, 1(4):705-720
[41] Kehrer JP. Free radicals as mediators of tissue injury and disease. Critical Reviews in Toxicology, 1993, 23(1):21-48
[42] Aruoma O. Nutrition and health aspects of free radicals and antioxidants. Food and Chemical Toxicology, 1994, 32(7):671-683
[43] Fiers W, Beyaert R, Declercq W, et al. More than one way to die: apoptosis, necrosis and reactive oxygen damage. Oncogene, 1999, 18(54):7719-7730
[44] Record IR, Dreosti IE, Konstantinopoulos M, et al. The influence of topical and systemic vitamin E on ultraviolet light-induced skin damage in Hairless Mice. Nutrition and Cancer, 1991,16(3):219-225
[45] Kawaguchi Y, Tanaka H, Okada T, et al. The effects of ultraviolet A and reactive oxygen species on the mRNA expression of 72-kDa type IV collagenase and its tissue inhibitor in cultured human dermal fibroblasts. Archives of Dermatological Research, 1996,288( 1):39-44
[46] Ogata M, Hoshi M, Urano S, et al. Antioxidant activity of eugenol and related monomeric and dimeric compounds. Chemical and Pharmaceutical Bulletin-tokyo, 2000, 48( 10): 1467-1469
[47] Guan W, LiS, Yan R, et al. Comparison of essential oils of clove buds extracted with supercritical carbon dioxide and other three traditional extraction methods. Food Chemistry, 2007, 101(4):1558-1564
5全文总结
挥发油是芳香植物的次生代谢产物,安全性高,生物活性强。本文首先优化了水.蒸气蒸馏法提取山苍子油、丁香花蕾油、香茅油的条件,并在优化条件下,提取了三种挥发油,然后用GC-MS法分析了三种挥发油的成分;探讨了山苍子油、丁香花蕾油、香茅油及其主要成分柠檬醛、柠檬烯、芳樟醇、月桂烯、松油醇、丁香酚、乙酸丁香酯、β -石竹烯、香茅醛、香叶醇、香茅醇与酪氨酸酶活性的关系,并研究了山苍子油的主要成分柠檬醛对酪氨酸酶的抑制类型;测定了山苍子油、丁香花蕾油、香茅油和其主要成分柠檬醛、丁 香酚、香茅醛对ABTS阳离子和超氧阴离子自由基的清除能力,研究了丁香花蕾油、香茅油和其主要成分柠檬醛、丁香酚、香茅醛对脂质过氧化的抑制作用;考查了山苍子油、丁香花蕾油、香茅油和其主要成分柠檬醛、丁香酚、香茅醛对UV - TiO2- NO2引起的蛋白质氧化和硝化抑制作用。
5.1本论文的主要研究成果
(1)运用水蒸气蒸馏法萃取的自然晾干的山苍子果实的挥发油呈淡黄色。GC-MS分析水蒸气蒸馏法提取的山苍子油鉴定出19种化学成分,占总油的92.4%。其主要成分柠檬醛的相对含量占57.4%, 柠檬烯的含量占8.1%, 芳樟醇的含量为5.2%,β- 月桂烯的相对含量为4.7%, a-松油醇的相对含量为3.9%,β- 蒎烯的相对含量为2.7%, a -蒎烯的相对含量为1.9%。 同样用GC-MS分析产于中国广东的丁香花蕾油,鉴定出10 种物质,占总油的94.8%。 主要成分丁香酚的相对含量为76.8%,乙酸丁香酯的相对含量为9.5%,β-石竹烯的相对含量为6.0%。GC_MS分析的香茅叶的挥发油鉴定出17 种成分,占总油的93.5%。 其中
主要成分香茅醛的相对含量为33.9% 、香叶醇的相对含量为18.1% 、香茅醇的相对含量为11.1%
(2)通过酪氨酸酶抑制试验来评价三种挥发油及其主要成分对酪氨酸酶的抑制效果。结果表明山苍子油和其主要成分柠檬醛对酪氨酸酶单酚酶和二酚酶活性有抑制能力,对酪氨酸酶二酚酶的抑制能力强于酪氨酸酶单酚酶,且动力学结果表明,柠檬醛对酪氨酸酶是非竞争性抑制作用。丁香花蕾油和丁香酚对酪氨酸酶单酚酶具有一定的抑制作用,但是对酪氨酸酶二酚酶没有表现出任何抑制作用。而香茅油及其主要成分对酪氨酸酶没有抑制作用。
(3)通过山苍子油、香茅油、丁香花蕾油体外清除ABTS阳离子和超氧阴离子实验,研究三种精油的抗氧化能力。发现丁香花蕾油及其主要成分丁香酚具有较强的清除ABTS阳离子的能力,山苍子油和其主要成分柠檬醛具有较强的清除超氧阴离子的能力。丁香花蕾油、香茅油、丁香酚、香茅醛都具有抗脂质过氧化的作用,并且随着剂量的增加,抗氧化活性逐渐增强。丁香花蕾油和丁香酚的抗氧化能力强于香茅油和香茅醛。而山苍子油几乎没有抗脂质过氧化的能力。丁香花蕾油、丁香酚、香茅油、香茅醛、山苍子油、柠檬醛均具有较强的抑制蛋白质氧化的能力,其中丁香酚的抑制蛋白质氧化的能力最强。丁香花蕾油和丁香酚具有很强的抑制酪氨酸硝化的能力,山苍子油、柠檬醛、香茅油、香茅醛仅在较高浓度时表现出较强的抑制蛋白质硝化的能力。
5.2本论文创新之处
(1)以挥发油这种具有多重生物活性的天然产物为研究对象,结合GC-MS分析结果,从整体上研究挥发油的生物活性,然后深入研究挥发油中起主要的作用的化学成分,从而全面探讨挥发油的活性机理。
(2)同时探讨挥发油对酪氨酸酶的抑制作用和抗氧化作用。发现山苍子油及其主要成分柠檬醛具有较强的酪氨酸酶抑制活性和清除自由基的能力,说明山苍子油在化妆品领域具有皮肤美白和预防皮肤衰老的作用,在食品领域具有防止食品褐变和氧化变质的作用。
(3)选择UV- TiO2- NO2体系作为引起蛋白质氧化和硝化的模型,而这种模型是最为接近因使用化妆品导致的皮肤中蛋白质发生氧化和硝化的模型。通过实验发现,丁香花蕾油、丁香酚、香茅油、香茅醛、山苍子油、柠檬醛均具有较强的抑制蛋白质氧化的能力,其中丁香酚的抑制蛋白质氧化的能力最强。丁香花蕾油和了香酚具有很强的抑制酪氨酸硝化的能力,山苍子油、柠檬醛、香茅油、香茅醛仅在较高浓度时表现出较强的抑制蛋白质硝化的能力。
本文献摘自华中科技大学黄晓伟博士学位论文,如若侵权,请告知删除。

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}