
伤口世界
- 星期三, 26 6月 2024
三种植物挥发油的化学成分、酪氨酸酶抑制能力及抗氧化活性的研究---三种天然植物精油对酪氨酸酶的活性抑制研究(三)
3.1 引言
酪氨酸酶是活性中心含有双核金属铜的氧化还原酶,是黑色素生物合成的关键酶[1]。组氨酸残基位于酪氨酸酶的内部,结合的铜离子为酪氨酸酶的活性位点[2.3]酪氨酸酶催化黑色素形成的前两步:L-酪氨酸羟化形成工-二羟苯丙氨酸(L-DOPA)和后续的联苯酚氧化为醌(L-多巴醌)[4-7]在催化反应过程中酪氨酸酶可以分为三种形态[8-10]:脱氧态(Edeoxy)、氧化态(Eoxy)和还原态(Emet)。还原型酶只具有二酚酶活性,氧化型酶同时具有酪氨酸羟化酶活性(即单酚酶活性)和多巴氧化酶活性(即二酚酶活性),而脱氧型酶能够结合氧分子。在酶促反应过程中,氧化型酶和还原型酶作用于底物的同时自身被还原成脱氧型,脱氧型酶能够结合一分子氧回到氧化状态,完成一个循环。酪酸酶二酚酶的活力就是酪氨酸酶在黑色素生成的第二步中表现出的活力。还原态的酶与L-DOPA 非共价结合形成醒,而还原态酶转化为脱态的酶的过程[11-12]。酪氨酸酶单酚酶活力通常被认为是酪氨酸酶在黑色素生成过程中第一步表现出来的活力,即 L-酪氨酸氧化成为L-DOPA 过程中表现出来的催化活性。但是实际上这·活力与酪氨酸酶氧化L-DOPA为醌的活力是同时表现的,所以研究学者通常将酪氨酸酶催化L-酪氨酸为L-DOPA,进一步催化为多巴醌的过程表现出来的酶活力称为单酚酶活力[11,13]。
在化妆品工业,越来越注重使用酪氨酸酶抑制剂来阻止黑色素的异常形成。酪氨酸酶抑制剂能够减少黑色素的合成,被用到化妆品中防止黑色素过度沉着,包括雀斑的形成。但是,只有极少数的美白剂被使用,典型的如曲酸和熊果苷,是目前商业上可以获得的。此外,有些美白剂的对细胞的高毒性、对氧和水的低稳定性导致其被限制使用。
在食品工业,胺类、氨基酸、肽类和蛋白质与醌(酶性褐变)之间的反应让食品在储藏或加工过程中容易变质。必须氨基酸的破坏、可消化性降低、蛋白水解酶和糖酵解酶的抑制是食品营养流失的主要原因。抗营养物质和毒性物质的产生会进一步降低食品的营养价值和安全性[14]。因此,建立多种阻止酶性褐变的方法至关重要。目前常用的防止褐变的方法有高压灭菌和短暂蒸煮的方法,这种传统的方法不可避免的造成营养物质的损失[15]。也有用微波技术来处理食品的方法,但是运用微波加热技术的最大限制因素是在使用微波的过程中会产生温度阶差[16]。酶的灭活需要高温处理,而低温是无法让酶完全失活。因此单纯使用微波加热技术无法让食物表面的酶完全失活。综合运用微波热水处理法能够在最终营养价值、食品重量、加工时间上有改进[17]。目前已经发现一些能够通过干扰酪氨酸酶介导的反应或者通过将醌类物质还原成酚来抑制食品的酶性褐变的化合物[18-20]。但是,因为这些化合物的气味、毒性和经济可行性使得真正能够在食品中运用的很少[21]。亚硫酸盐类物质曾经被广泛用于农业和海产品领域来防止酶性褐变,但由于其安全性问题被食品药品监督管理局禁用[22]。而食品工业中最多被运用的是维生素℃和柠酸[20,23]。但是他们防褐变的能力没有亚硫酸盐强,因为在还原酪氨酸酶形成的醌类物质的过程中维生素C会很快被消耗。4-已基间苯二酚在食品中的使用被认为是安全的,并且能够有效的防止新鲜的水果和水果干的褐变。但是,作为食品工业中使用的抑制剂,安全性是首要考虑的问题。因此,不断寻找天然来源的没有副作用的抑制剂意义重大。
综上所述,开发出一系列安全性高、能够广泛应用于食品及化妆品领域的酪氨酸酶抑制剂具有重要意义。本章以山苍子油、香茅油、丁香花蕾油为目标,研究其对酪氨酸酶的抑制活性,并对每种挥发油的主要成分做进一步酪氨酸酶抑制试验,确定挥发油中的活性成分。
3.2材料与方法
3.2.1试剂与仪器
3.2.1.1主要试剂
蘑菇酪氨酸酶、L-DOPA、曲酸: .上海华蓝试剂有限公司;柠檬醛、柠檬烯、芳樟醇、β-月桂烯、a-松油醇、a-蒎烯、β-蒎烯、丁香酚、乙酸丁香酯、香茅醛、香叶醇、香茅醇:阿拉丁T试剂公司; L -酪氨酸:国药集团化学试剂有限公二甲亚砜(DMSO)及其它化学试剂均为分析纯。试验用纯水均为18.2M9纯水。
3.2.1.2主要试验仪器设备
Milli-Q Synthesis超纯水系统:美国Millipore 公司;RT-6000酶标仪:深圳雷杜生命科学股份有限公司。
3.2.2酪氨酸酶抑制试验
首先将山苍子油、香茅油、丁香花蕾油和标准品(柠檬醛、柠檬烯、芳樟醇、β-月桂烯、a.-松油醇、a.-蒎烯、β-蒎烯、丁香酚、乙酸丁香酯、香茅醛、香叶醇、香茅醇)分别溶于DMSO,随后用磷酸盐缓冲溶液稀释至适当的浓度作为测试样品。
酪氨酸酶二酚酶活性的测定:按照之前文献报道的方法[24-28]并做适当的修改。L-DOPA作为酪氨酸酶活性测定的底物。500 μL pH 6.8的磷酸盐缓冲溶液,150 μL2.5mM L-DOPA,50 μL不同浓度的受试样品混合均匀,25°C孵育10分钟。然后加入25 μL蘑菇酪氨酸酶(1380U/mL)。25°C孵育10分钟后,立即测其在475nm处的吸光度值。曲酸作为阳性对照。试验重复3次,数据取平均值。
单酚酶活力的测定:先将300 μuL 3mmol/L的L-酪氨酸溶液与100 μuL磷酸盐缓冲液(pH6.8) 充分混匀,50 μL不同浓度的受试样品混合均匀,于30°C 水浴中温浴10 min后,加入100 μL蘑菇酪氨酸酶( 1380U/ mL)。25°C孵育10分钟后,立即在475 nm处测定吸光度值。曲酸作为阳性对照。试验重复3次,数据取平均值。
酪氨酸酶抑制率的计算:
Inhibition (%) = (Arest smple - Abank)/ Acontrol x 100
其中Acotol为混合液添加了酪氨酸酶而没有加入受试样品的吸光度值; Ablank为混合液加入受试样品但是没有加入酪氨酸酶的吸光度值; Atest sample是混合液加入了受试样品和酪氨酸酶后的吸光度值。
3.2.3柠檬醛抑制类型的测定
实验方法参照之前文献报道的方法并作适当修改[29, 30],不同浓度的L-DOPA(0.25 mM,0.333 mM,0.5 mM,1.0mM, 4.0 mM)作为底物, 825μL 磷酸盐缓冲溶液(pH6.8)加入75μL实验样品(0,0.1 mM, 0.5 mM),37.5μL 酪氨酸酶。用紫外分光光度计测475 nm处吸光值每分钟的增加量。酪氨酸酶活性的米氏常数Km和最大速度通过Lineweaver- _Burk plot来决定。
3.3实验结果
3.3.1丁香花蕾油与酪氨酸酶活性之间的关系
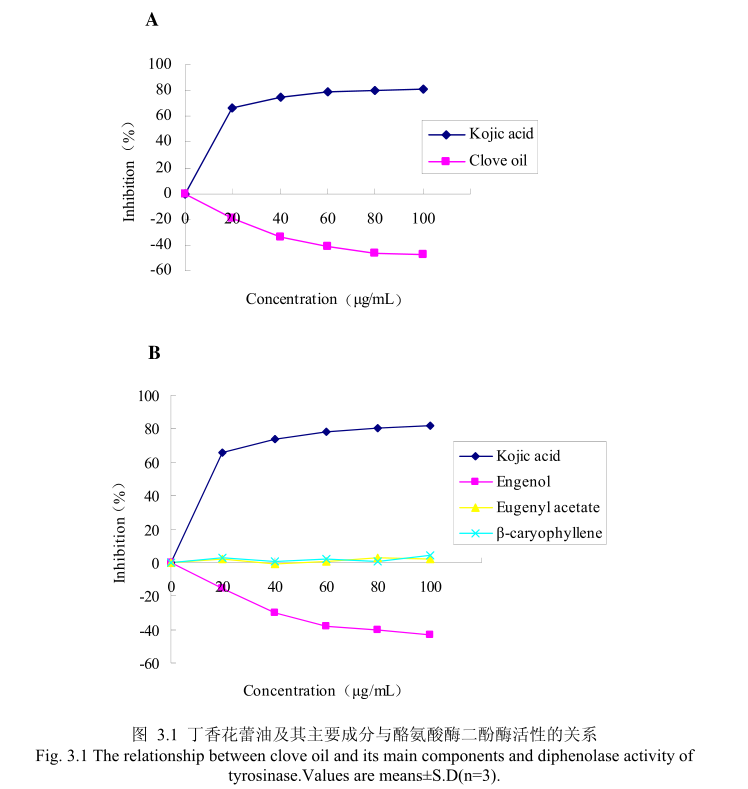
丁香花蕾油浓度与酪氨酸酶二酚酶活性之间的关系如图3.1A所示。我们选择具有强抑制酪氨酸酶活的曲酸为阳性对照,从图3.1A 我们可以看出,在曲酸浓度为0-20μg/m 时,随着曲酸浓度的增加,对酪氨酸酶二酚酶的活性有明显的抑制作用,抑制率达到 65.3%:当随着曲酸的浓度依次增高时,对酪氨酸酶二酚酶的抑制效率呈逐渐提升趋势,但增加的趋势较为缓慢,当曲酸浓度为100g/mL时,其对酪氨酸酶二酚酶的抑制率达到 76.1%。但丁香花蕾油对酪氨酸酶二酚酶的抑制率随其浓度的增加,抑制率呈负增长,表明丁香花蕾油对酪氨酸酶二酚酶没有明显的抑制作用。
为了进一步研究丁香花蕾油中的主要成分是否有抑制酪氨酸酶二酚酶酶活的能力,我们选取了丁香花蕾油中的三种主要成分,丁香酚、乙酸丁香酯和B-石竹烯,分别研究了他们的浓度和酪氨酸酶二酚酶抑制率之间的关系(图3.1B)。从图3.1B 中可以看出,丁香花蕾油主要成分丁香酚、乙酸丁香酯、B-石竹烯对酪氨酸酶二酚酶都没有明显的抑制能力。
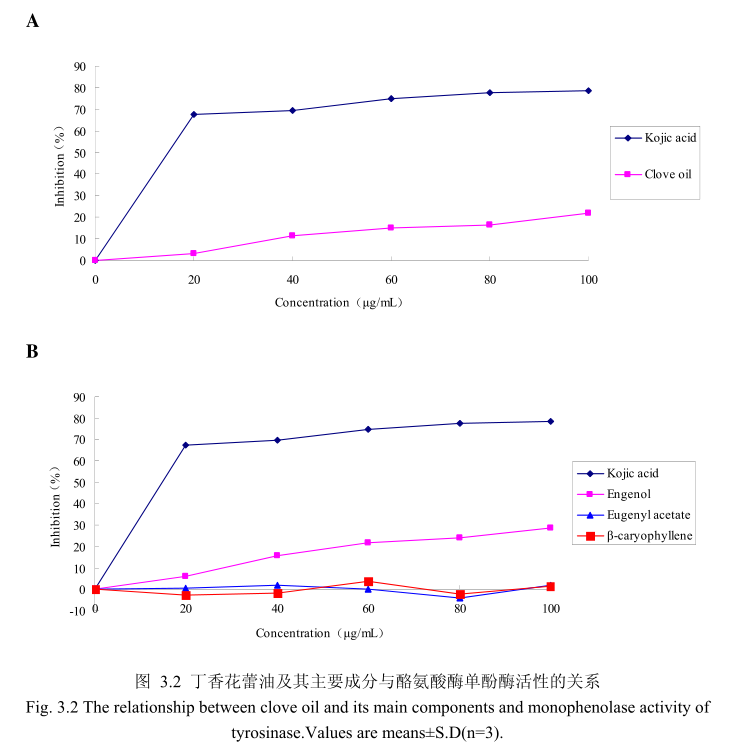
丁香花蕾油浓度与酪氨酸酶单酚酶活性之间的关系如图3.2A所示。我们选择具有强抑制酪氨酸酶活的曲酸为阳性对照,从图3.2A可以看出,在曲酸浓度为0-20μg/m 时,随着曲酸浓度的增加,对酪氨酸酶单酚酶活性有明显的抑制作用抑制率达到 70%;当随着曲酸的浓度依次增高时,对酪氨酸酶单酚酶的抑制率呈逐渐提升趋势,但增加的趋势较为缓慢,当曲酸浓度为100g/m时,其对酪氨酸酶单酚酶的抑制率达到 78.6%。丁香花蕾油对酪氨酸酶单酚酶的抑制率随其浓度的增加而增加,但是增加较为缓慢,当丁香花蕾油的浓度为100g/mL时,抑制率为 21.9%,表明丁香花蕾油对酪氨酸酶单酚酶活性有一定的抑制作用,但是曲酸对酪氨酸酶单酚酶活性的抑制作用强于丁香花蕾油。
为了进一步研究丁香花蕾油中的主要成分是否有抑制酪氨酸单酚酶的能力,我们选取了丁香花蕾油中的三种主要成分,丁香酚、乙酸丁香酯和B-石竹烯,分别研究了他们的浓度和酪氨酸酶单酚酶抑制率之间的关系(图3.2B)。从图3.2B中可以看出,丁香花蕾油主要成分丁香酚具有一定的抑制酪氨酸酶单酚酶活性的能力,当丁香酚的浓度为40μg/m 时,对酪氨酸酶单酚酶抑制率为16%,随着丁香酚的浓度逐渐增加,丁香酚对酪氨酸酶单酚酶的活性抑制作用逐渐增强,当丁香酚的浓度为 100g/m 时,丁香酚对酪氨酸酶单酚酶的活性的抑制率为28.6%。抑制作用比同样浓度下丁香花蕾油略强,但是比曲酸的的抑制作用弱。而丁香花蕾油的主要成分乙酸丁香酯、B-石竹烯对酪氨酸酶单酚酶都没有明显的抑制能力。
3.3.2 山苍子油与酪氨酸酶之间的关系
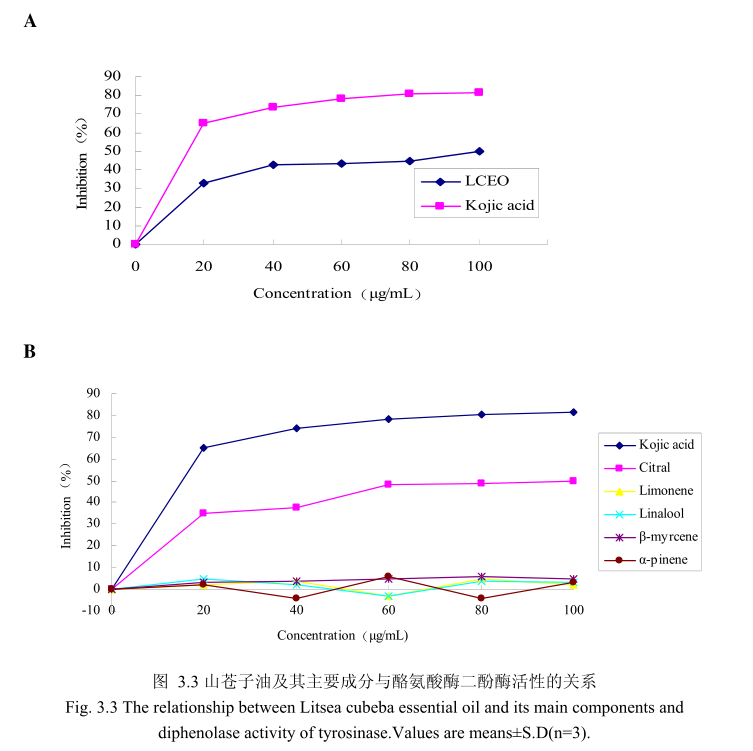
山苍子油浓度与酪氨酸酶二酚酶活性之间的关系如图3.3A 所示。我们选择具有强抑制酪氨酸酶活的曲酸为阳性对照,从图3.3A可以看出,在曲酸浓度为0-20Hg/m 时,随着曲酸浓度的增加,对酪氨酸酶二酚酶的活性有明显的抑制作用,抑制率达到 65.3%;当随着曲酸的浓度依次增高时,对酪氨酸酶二酚酶的抑制效率呈逐渐提升趋势,但增加的趋势较为缓慢,当曲酸浓度为100g/m时,其对酪氨酸酶二酚酶的抑制率达到 76.1%。山苍子油对酪氨酸酶二酚酶活性亦有明显的抑制作用,当浓度为0-20μg/m时,随着山苍子油浓度的增加,对酪氨酸酶二酚酶活性有明显的抑制作用,抑制率达到32%;当随着山苍子油的浓度依次增高时,对酪氨酸酶二酚酶活性的抑制率呈逐渐提升的趋势,但增加趋势较为缓慢,当山苍子油的浓度为100g/m 时,其对酪氨酸酶二酚酶的抑制率达到50%。因此,对照样品曲酸和山苍子油都对酪氨酸酶二酚酶的活性有较好的抑制作用,但是曲酸对酪氨酸酶二酚酶的抑制作用强于山苍子油。
为进一步研究山苍子油中的主要成分是否具有抑制酪氨酸酶二酚酶活性的能力,我们选取了山苍子油中的五种主要成分柠檬醛、柠檬烯、芳樟醇、月桂烯、松油醇,分别研究了他们的浓度和酪氨酸酶二酚酶抑制率之间的关系(图3.3B)。从图3.3B中可以看出,山苍子油主要成分柠醛对酪氨酸酶二酚酶活性具有较好的抑制能力,柠檬醛的浓度为 100μg/m 时,对酪氨酸酶二酚酶的抑制率达到 48%。而柠檬烯、芳樟醇、月桂烯、松油醇并没有表现出明显的对酪氨酸酶二酚酶的抑制作用。
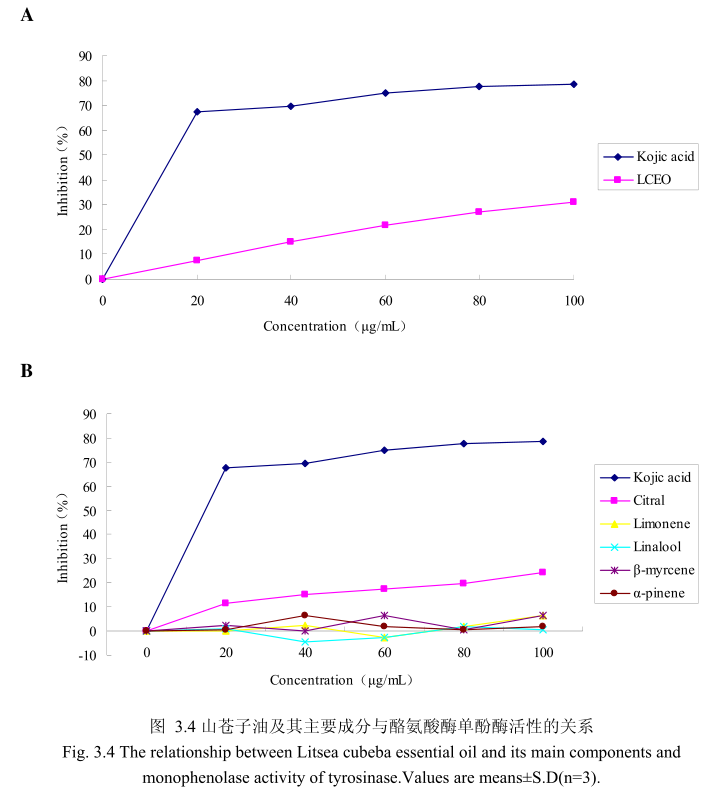
山苍子油浓度与酪氨酸酶单酚酶活性之间的关系如图3.4A所示。选择具有强抑制酪氨酸酶活性的曲酸为阳性对照。从图3.4A可以看出,在曲酸浓度为0-20μg/m 时,随着曲酸浓度的增加,对酪氨酸酶单酚酶的活性有明显的抑制作用,抑制率达到 67.4%;当随着曲酸的浓度依次增高时,对酪氨酸酶单酚酶的抑制率呈逐渐提升趋势,但增加的趋势较为缓慢,当曲酸浓度为100g/m时,其对酪氨酸酶单酚酶的抑制率达到 78.6%。山苍子油对酪氨酸酶单酚酶活性亦有一定的抑制作用,当浓度为0-20μg/mL 时,随着山苍子油浓度的增加,对酪氨酸酶单酚酶活性有一定的抑制作用,抑制率为7.6%;当随着山苍子油的浓度依次增高时,对酪氨酸酶单酚酶的抑制率呈逐渐提升的趋势,但增加趋势较为缓慢,当山苍子油的浓度为100g/m 时,其对酪氨酸酶单酚酶的抑制率达到31%。因此,对照样品曲酸对酪氨酸酶单酚酶的活性有较好的抑制作用,山苍子油对酪氨酸酶单酚酶具有一定的抑制作用。
为进一步研究山苍子油中的主要成分是否具有抑制酪氨酸酶单酚酶的能力,我们选取了山苍子油中的五种主要成分柠檬醛、柠檬烯、芳樟醇、月桂烯、松油醇,分别研究了他们的浓度和酪氨酸酶单酚酶抑制率之间的关系(图3.4B)。从图3.4B中可以看出,山苍子油主要成分柠檬醛对酪氨酸酶单酚酶活性具有一定的抑制能力,柠檬醛的浓度为100μg/m 时,对酪氨酸酶的抑制率达到 24.1%。而柠檬烯、芳樟醇、月桂烯、松油醇并没有表现出明显的对酪氨酸酶单酚酶的抑制作用。
3.3.3 柠檬醛抑制类型的测定
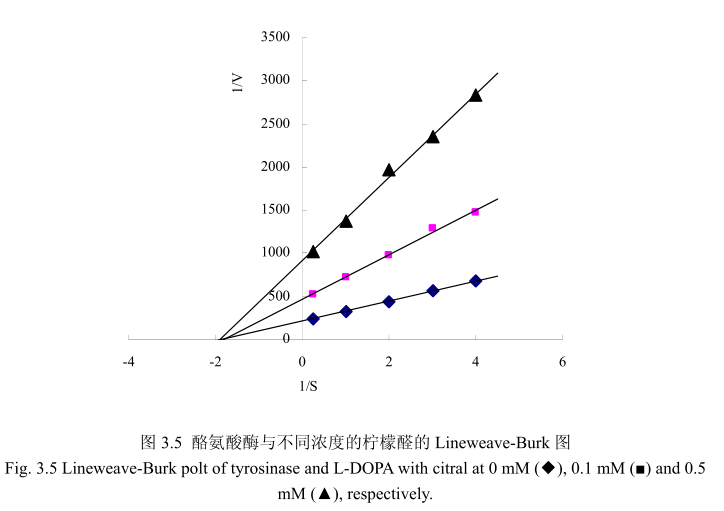
酶的抑制作用的研究主要是研究酶的催化机制、酶的结构和功能以及阐明酶的代谢途径的基本手段,同时也可以为新药物的设计、开发以及相关新产品研发提供一定的理论依据。因此,对酶的抑制作用及类型的研究具有重要的价值和理论意义如果抑制剂对酶的抑制作用是可逆的,即抑制剂与酶以非共价键的形式结合而引起酶的活力降低甚至是丧失,能够通过物理方法将抑制剂除去而让酶恢复活性,我们称之为可逆抑制;如果抑制剂对酶的抑制作用是不可逆的,即抑制剂与酶的必须基团以共价键的形式结合而引起酶失活,运用透析、超滤等物理方法不能将抑制剂去除而引起的酶活力丧失,我将其称之为不可逆抑制。可逆抑制作用可以根据抑制剂、底物和酶之间的关系而分为非竞争性抑制、反竞争性抑制和竞争性抑制。在非竞争性抑制过程中,抑制剂和底物能够同时和酶结合,两者之间没有竞争作用。酶与底物结合后还可以与抑制剂结合,同时酶与抑制剂结合后也可以与底物结合。但是这种由酶、抑制剂、底物结合而成的三元复合物不能够进一步分解为产物,因此会导致酶的活力降低。这种类型的抑制剂与酶的活性部位以外的基团相结合,其结构与底物没有相同的地方,这种类型的抑制作用不能通过增加底物浓度来解除抑制,所以称之为非竞争性抑制。在结构上,大多数的竞争性抑制剂与底物具有相似性,因此能够与酶的活性位点结合,与酶能够形成可逆的复合物,但是这种复合物不能够分解为产物,导致酶的反应速度下降。竞争性抑制剂的抑制程度取决于底物及抑制剂的相对浓度,这种抑制作用可以通过增加底物浓度而解除31。本节通过Lineweaver-Burk polts 分析抑制动力学,从而判断柠檬醛对酪氨酸酶抑制 L-DOPA氧化的机制。从图3.5可以看出,三条线分别代表不同浓度(0mM(◆),0.1mM(■),0.5 mM(▲))的柠檬醛,并且在 1/S 轴上相交于一点。结果表明柠檬醛是非竞争性抑制。结果与相关文献23报道一致。抑制剂柠檬醛与游离酶和酶底物复合物耦合醛类化合物如柠檬醛是蛋白质反应化合物,能够与生物学上重要的亲核基团基氨基或羟基反应。醛类能够与酪氨酸酶上的氨基形成席夫碱。不同醛类物质对酪氨酸酶的抑制活性的强弱取决于酪氨酸酶与醛类物质之间形成的席夫碱的稳定性。因此,可以认为酪氨酸酶抑制活性是由于柠檬醛与酪氨酸酶活性部位周围的亲核基团之间形成了席夫碱,形成了空间位阻阻碍酶与底物的结合,从而降低酶的活性。
3.3.4 香茅油与酪氨酸酶之间的关系
香茅油与酪氨酸酶二酚酶之间的关系如图3.6A所示。我们选择具有强抑制酪氨酸酶活性的曲酸为阳性对照。从图3.6A中可以看出,在曲酸浓度为0-20mg/mI时,随着曲酸浓度的增加,对酪氨酸酶二酚酶的活性有明显的抑制作用,抑制率达到 65.3%;当随着曲酸的浓度依次增高时,对酪氨酸酶二酚酶的抑制率呈逐渐提升趋势,但增加的趋势较为缓慢,当曲酸浓度为100g/m时,其对酪氨酸酶二酚酶的抑制率达到 76.1%。但是香茅油对酪氨酸酶二酚酶的抑制率随其浓度的增加,抑制率呈负增长,表明香茅油对酪氨酸酶二酚酶活性没有明显的抑制作用。
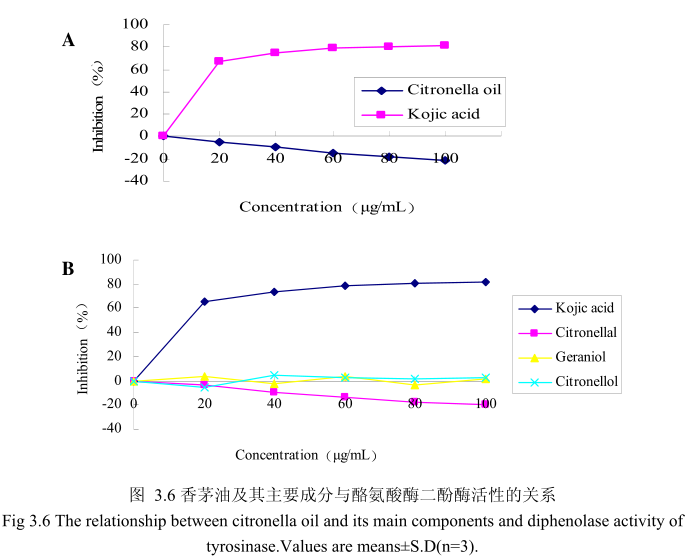
为了进一步研究香茅油中的主要成分是否有抑制酪氨酸酶二酚酶活性的能力,我们选取了香茅油中的三种主要成分,香茅醛、香叶醇和香茅醇,分别研究了他们的浓度和酪氨酸酶二酚酶抑制率之间的关系(图3.6B)。从图3.6B 中可以看出,香茅油主要成分香茅醛、香叶醇和香茅醇对酪氨酸酶二酚酶都没有明显的抑制能力。
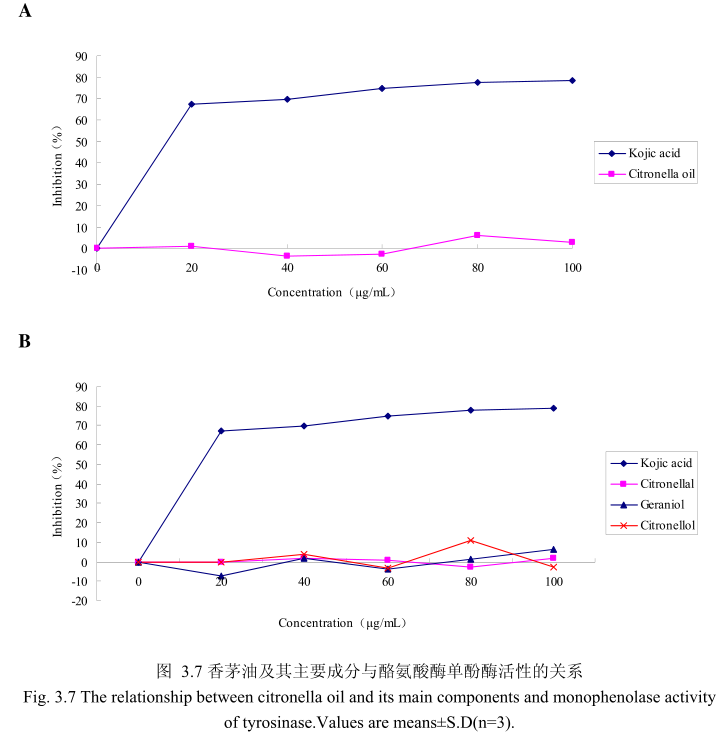
香茅油与酪氨酸酶单酚酶之间的关系如图3.7A所示。我们选择具有强抑制酪氨酸酶活的曲酸为阳性对照。从图3.7A中可以看出,在曲酸浓度为0-20g/mL时,随着曲酸浓度的增加,对酪氨酸酶单酚酶的活性有明显的抑制作用,抑制率达到 67.4%;当随着曲酸的浓度依次增高时,对酪氨酸酶单酚酶的抑制效率呈逐渐提升趋势,但增加的趋势较为缓慢,当曲酸浓度为100g/m时,其对酪氨酸酶单酚酶的抑制率达到 78.6%。但是香茅油对酪氨酸酶单酚酶活性的抑制率随其浓度的增加并没有明显的变化,表明香茅油对酪氨酸酶单酚酶活性没有明显的抑制作用。
为了进一步研究香茅油中的主要成分是否有抑制酪氨酸酶单酚酶活性的能力,我们选取了香茅油中的三种主要成分,香茅醛、香叶醇和香茅醇,分别研究了他们的浓度和酪氨酸酶抑制率之间的关系(图3.7B)。从图3.7B中可以看出,香茅油主要成分香茅醛、香叶醇和香茅醇对酪氨酸酶单酚酶都没有明显的抑制能力。
3.4 讨论
本章实验的主要目的是研究山苍子油、丁香花蕾油、香茅油对酪氨酸酶的抑制作用,并进一步探讨抑制机制。酪氨酸酶与人密切相关,是一种含有铜离子的酶通过两种不同的途径催化黑色素合成:通过酪氨酸酶羟化酪氨酸和氧化L-DOPA 为多巴配[32-34]。酪氨酸酶广泛存在于植物和动物中,参与黑色素的形成[35-37]。在食品工业,酪氨酸酶在控制食品和水果蔬菜的质量方面非常重要[36-38]。酪氨酸酶催化酚类物质氧化为对应的醌类,是水果和蔬菜酶性褐变的关键酶。此外,酶性褐变引起醌类物质与蛋白质上的氨基和巯基发生不可逆的反应,从而产生让人讨厌的颜色和气味。醌类物质与蛋白质的反应降低了蛋白质的可溶性和必须氨基酸的生物活性,包括赖氨酸和半胱氨酸。人类皮肤和头发的颜色取决于很多因素,最重要的就是黑色素的分布[39]。黑色素能够通过吸收紫外线和清除活性氧保护皮肤,但是黑色素的过度沉着如黑斑病、老年斑、雀斑常常影响美观。
挥发油通常具有明显的香气,常常用于香精的调配,广泛应用于食品和日化品中。同时,因为挥发油普遍具有抑制微生物生长的作用,能够作为天然防腐剂应用于食品及日化品中。而挥发油在养生保健方面,常常与植物油脂混合后直接用于皮肤按摩,不仅能够放松神经,更能起到养颜美容的功效。因此,如果挥发油能够作为酪氨酸酶抑制剂使用,将具有其它抑制剂所不具有的众多优势。
有相关文献报道丁香甲醇萃取物能够抑制B16黑素细胞中黑色素的形成[40]。丁香甲醇萃取物的主要活性物质为丁香酚和丁香乙酸酯,当浓度为100 μg/mL和200ug/mL时,对B16黑色素细胞中黑素的抑制率达到60%和40%。而丁香花蕾油同样含有丁香酚和丁香乙酸酯,当浓度为100μg/mL 和200 μg/mL时,对B16黑色素细胞中黑素的抑制率达到50%和80%。而本章实验中丁香花蕾油的主要成分为丁香酚和乙酸丁香酯,当其浓度均为100 μg/ mL时均没有表现出酪氨酸酶二酚酶抑制活性。丁香花蕾油对酪氨酸酶单酚酶的抑制率随其浓度的增加而增加,但是增加较为缓慢,当丁香花蕾油的浓度为100 ug / mL时,抑制率为219%,表明丁香花蕾油对酪氨酸酶单酚酶活性有一定的抑制作用。丁香花蕾油主要成分丁香酚具有一定的抑制酪氨酸酶单酚酶活性的能力,当丁香酚的浓度为40μg/ mL时,酪氨酸酶单酚酶抑制率为16%, 随着丁香酚的浓度逐渐增加,丁香酚对酪氨酸酶单酚酶的活性抑制作用逐渐增强,当丁香酚的浓度为100 μg/mL时,丁香酚对酪氨酸酶单酚酶活性的抑制率为28.6%。抑制作用比同样浓度下丁香花蕾油略强,但是比曲酸的抑制作用弱。而丁香花蕾油的其他主要成分如乙酸丁香酯、β-石竹烯对酪氨酸酶单酚酶都没有明显的抑制能力。体外实验与文献报道的细胞实验有一定的差异,可能是由于丁香花蕾油的酪氨酸酶抑制活性在体外实验环境和细胞实验环境中本身就存在差异。同时,由于体外实验环境是水溶性环境,丁 香花蕾油在水中的溶解度有限,如果当丁香花蕾油的浓度进--步增大,则表现出更强的酪氨酸酶抑制能力。
本实验中证明山苍子油及其主要成分柠檬醛对酪氨酸酶单酚酶和二酚酶活性均有抑制作用,与之前有文献报道柠檬油及其主要成分柠檬醛有酪氨酸酶抑制活性一致[29]。醛类是已知的与具有生物活性的亲核基团(如巯基、氨基、羟基)反应的重要基团,所以它的抑制活性是由于醛基可以与酪氨酸酶活性中心周围的氨基反应形成席夫碱,产生的空间位阻阻碍酶与底物的结合,从而酶活性降低。
鉴于试验中发现山苍子油的抑制效果要高于同等含量的柠檬醛,所以我们研究了山苍子油中主要成分对酪氨酸酶的抑制效果。从图3.3和3.4中可以看出,山苍子油对酪氨酸酶抑制的作用主要来自于柠檬醛,柠檬烯的作用很小,其他成分芳樟醇、松油醇、月桂烯在同等浓度下没有表现出对酪氨酸酶的抑制作用。可以推断,山苍子油所表现出对酪氨酸酶的抑制活性强于柠檬醛可能由于其他未知成分引起,也可能是由于在某种组分的协同作用下,使柠檬醛的抑制活性增强。
本章实验表明,香茅油及其主要成分香茅醛并没有表现出酪氨酸酶单酚酶和二酚酶的抑制活性。而香茅醛与柠檬醛有着相似的结构,并且醛类物质也可能与酪氨酸酶上的氨基形成席夫碱。但是香茅醛并没有表现出酪氨酸酶抑制活性,可能是由于香茅醛与酪氨酸酶.上的氨基形成的希夫碱稳定性比柠檬醛与酪氨酸酶上的氨基形成的席夫碱要弱。
3.5本章小结
本章主要探讨丁香花蕾油、山苍子油、香茅油对酪氨酸酶的抑制作用。通过实验发现,丁香花蕾油对酪氨酸酶二酚酶没有抑制作用,对酪氨酸酶单酚酶具有--定的抑制作用,当浓度为100 μg/mL时,抑制率为219%。丁香花蕾油的主要成分丁香酚、乙酸丁香酯、β-石竹烯对酪氨酸酶二酚酶没有抑制作用,但是J香酚对酪氨酸酶单酚酶具有- -定的抑制作用,当丁香酚的浓度为100 ug/mL时,丁香酚对酪氨酸酶单酚酶活性的抑制率为28.6%, 而乙酸丁香酯、β -石竹烯对酪氨酸酶单酚酶也没有表现出抑制作用。香茅油及其主要成分香茅醛、香叶醇、香茅醇对酪氨酸酶单酚酶和二酚酶均没有抑制作用。山苍子油对酪氨酸酶二酚酶有较好的抑制作用,当浓度为100 ug/ mL时对酪氨酸酶二酚酶活性的抑制率达到50%。山苍子油中的主要成分柠檬醛对酪氨酸酶二酚酶有抑制作用,当浓度为105μg/mL时对酪氨酸酶的活性抑制率达到50%,山苍子油中的其他主要成分柠檬烯、芳樟醇、月桂烯、松油醇并没有表现出明显的对酪氨酸酶__.酚酶的抑制作用。山苍子油对酪氨酸酶单酚酶活性亦有一定的抑制作用,当山苍子油的浓度为100 ug/mL时,其对酪氨酸酶单酚酶的抑制率达到31%。山苍子油中的主要成分柠檬醛对酪氨酸酶单酚酶活性具有一定的抑制能力,当柠檬醛的浓度为100 ug/ mL时,对酪氨酸酶单酚酶的抑制率达到24.1%。 而其他主要成分柠檬烯、芳樟醇、月桂烯、松油醇并没有表现出明显的对酪氨酸酶单酚酶的抑制作用。通过Lineweaver-Burk polts进一步分析柠檬醛的抑制类型,结果表明柠檬醛为非竞争性抑制。
3.6参考文献
[1] Kwon BS, Haq AK, Pomerantz SH, et al. Isolation and sequence of a cDNA clone for human tyrosinase that maps at the mouse c-albino locus. Proceedings of the National Academy of Sciences of the United States of America, 1987,84(21):7473- -7477
[2] Hearing VJ, Jimenez M. Mammalian tyrosinase - the critical regulatory control point in melanocyte pigmentation. International Journal of Biochemistry, 1987, 19(12):1141-1147
[3] Ito S, Wakamatsu K. Quantitative analysis of eumelanin and pheomelanin in humans, mice, and other animals: a comparative review. Pigment Cell Research, 2003, 16(5):523-531
[4] Prota G. The role of peroxidase in melanogenesis revisited. Pigment Cell Research, 1990,3:25-31
[5] Hearing V. Unraveling the melanocyte. American Journal of Human Genetics, 1993, 52(1):1-7
[6] Ito S, Fujita K, Takahashi H, et al. Characterization of melanogenesis in mouse and guinea pig hair by chemical analysis of melanins and of free and bound dopa and 5-S-cysteinyldopa. Journal of Investigative Dermatology, 1984, 83(1):12-14
[7] Strothkamp K, Jolley R, Mason H. Quaternary structure of mushroom tyrosinase. Biochemical and Biophysical Research Communications, 1976, 70(2):519-524
[8] 王芳.桑叶中酪氨酸酶抑制成分的研究.浙江工商大学博士学位论文.2008.
[9] Fenol LG, Rodriguez-Lopez JN, Garcia Sevilla F, et al. Analysis and interpretation of the action mechanism of mushroom tyrosinase on the monophenols and diphenols generating highly unstable O-quinones. Biochimica et Biophysica Acta(BBA)-Protein Structure and Molecular Enzymology, 2001,1548:1-22
[10] Decker H, Terwilliger N. Cops and robbers:putative evolution of copper oxygen-binding proteins. The Journal of Experimental Biology, 2000, 203:1777-1782
[11]林敏, 抑制剂对蘑菇酪氨酸酶与马铃薯多酚氧化酶抑制效应的比较研究.厦门大学硕士学位论文.2007.
[12] Naish-Byfield S, Riley PA. Oxidation of monohydric phenol substrates by tyrosinase. Biochemistry, 1992, 288:63-67
[13] Espin JC. Kinetic characterization of the substrate specificity and mechanism of mushroom tyrosinase. Biochemistry, 2000, 267:1270-1279
[14] Bos C, Gandichon C, Tome D. Nutritional and physiological criteria in the assessment of milk protein quality for humans. Journal of the American College of Nutrition, 2000,19(2): 191-205
[15] Konanayakam M, Sastry S. Kinetics of shrinkage of mushrooms during blanching. Journal of Food Science, 1988, 53(5): 1406-1411
[16] Maskan M. Drying, shrinkage and rehydration charateristics of kiwifruits during hot air and microwave drying. Journal of Food Engineering , 2001 ,48(2):177-182
[17] Devece C, Rodriguez-Lopez JN, Fenoll LG, et al. Enzyme inactivation analysis for industrial blanching applications: comparison of microwave, conventional, and combination heat treatments on mushroom polyphenoloxidase activity. Journal of Agricultural and Food Chemistry, 1999, 47(11):4506-4511
[18] Langdon T. Preventing of browning in fresh prepared potatoes without the use of sulfiting agents. Food Technology, 1987, 41(5):64-67
[19] Dudley ED, Hotchkiss JH. Cysteine as an inhibitor of polyphenol oxidase.Journal of Food Biochemistry, 1989, 13( 1):65-75
[20] Santerre CR, Cash J, Vannorman D. Ascorbic acid/citric acid combinations in the processing of frozen apple slices. Journal of Food Science, 1988, 53(6): 1713-1716
[21] Kim YJ, Uyama H. Tyrosinase inhibitors from natural and synthetic source:structure, inhibitor mechanism and perspective for the future. Cellular and Molecular Life Sciences, 2005,62:1707-1723
[22] Chalom s, Elrezzi E, Pena P, et al. Composition of sulfited potatoes: comparision with fresh and frozen potatoes. Plant Foods for Human Nutrition, 1995,47:133-138
[23] Hsu A, Shieh J, Bills D, et al. Inhibition of mushroom polyphenoloxidase by ascorbic acid derivatives. Journal of Food Science, 1988, 53(3):765-767
[24] Yu LL, Hu WC, Ding G, et al. Gusanlungionosides A-D, Potential Tyrosinase Inhibitors from Arcangelisia gusanlung. Jourmal of Natural Products, 2011,74(5): 1009-1014
[25] Kubo I, Kinst-Hori I. Tyrosinase inhibitors from cumin. Journal of Agricultural and Food Chemistry, 1998, 46( 12):5338-5341
[26] Kubo I, Kinst-Hori I, Chaudhuri SK, et al. Flavonols from Heterotheca inuloides: tyrosinase inhibitory activity and structural criteria. Bioorganic & Medicinal Chemistry, 2000, 8(7):1749- 1755
[27] Kubo I, Kinst-Hori I. Tyrosinase inhibitory activity of the olive oil flavor compounds. Journal of Agricultural and Food Chemistry, 1999,47(11):4574-4578
[28] Kubo I, Kinst: Hori I. Tyrosinase inhibitors from anise oil. Journal of Agricultural and Food Chemistry, 1998, 46(4):1268-1271
[29] Matsuura R, Ukeda H, Sawamura M. Tyrosinase inhibitory activity of citrus essential oils. Journal of Agricultural and Food Chemistry, 2006, 54(6):2309-2313
[30] Ha YM, Chung SW, Song S, et al. 4-(6-Hydroxy-2-naphthyl)-1, 3-bezendiol: apotent, new tyrosinase inhibitor. Biological and Pharmaceutical Bulletin, 2007,
30(9):1711-1715
[31] 王镜岩,朱圣庚,徐长法.生物化学.第三版.高等教育出版社,2002.368-369
[32] Canovas FG, Garcia-Carmona F, Sanchez JV, et al. The role of pH in the melanin biosynthesis pathway. Journal of Biological Chemistry, 1982, 257(15):8738-8744
[33] Neptuno Rodriguez-Lopez J, Tudela J, Varon R, et al. Kinetic study on the effect of pH on the melanin biosynthesis pathway. Biochimica et Biophysica Acta (BBA)-Protein Structure and Molecular Enzymology, 1991, 1076(3):379-386
[34] Cooksey CJ, Garratt PJ, Land EJ, et al. Evidence of the indirect formation of the catecholic intermediate substrate responsible for the autoactivation kinetics of tyrosinase. Jourmal of Biological Chemistry, 1997,272(42):26226-26235
[35] Pawelek JM, Korner AM. The Biosynthesis of Mammalian Melanin: The regulation of pigment formation, the key to disorders such as albinism and piebaldism, may also offer some clues for the treatment of melanoma. American Scientist, 1982, 70(2):136-145
[36] Mayer AM. Polyphenol oxidases in plants -recent progress. Phytochemistry, 1986, 26(1):11-20
[37] Kocher A, Choct M, Hughes RJ, et al. Effect of food enzymes on utilisation of lupin carbohydrates by broilers. British Poultry Science, 2000,41(1):75-82
[38] Friedman M. Food browning and its prevention: an overview. Journal of Agricultural and Food Chemistry, 1996, 44(3):631-653
[39] Passeron T, Mantoux F, Ortonne JP. Genetic disorders of pigmentation. Clinics in Dermatology, 2005,23(1):56-67
[40] Arung ET, Matsubara E, Kusuma IW, et al. Inhibitory components from the buds of clove (Syzygium aromaticum) on melanin formation in B 16 melanoma cells. Fitoterapia, 2011, 82(2):198-202
未完待续……
- 星期一, 24 6月 2024
三种植物挥发油的化学成分、酪氨酸酶抑制能力及抗氧化活性的研究---三种天然植物挥发油的提取和成分分析(二)
2.1 引言
挥发油是芳香植物中次生代谢形成的具有挥发性的天然混合物,具有强烈的香气。挥发油最初在中世纪由阿拉伯人通过水蒸气蒸馏获得。由于其具有杀菌、抗病毒、抑制微生物繁殖的特性,被用于食品保存、抗微生物、止痛、镇静、抗炎、解痉挛和局部麻醉。直至今天,这些性质并没有很大变化,只是在作用机制方面的研究更加深入,尤其是在抗微生物领域的研究。
在自然界,挥发油在保护植物方面有着重要的作用,如抗微生物、抗病毒、抗真菌、杀虫、降低食草动物的食欲。
挥发油为传统药典中的一个重要部分,外观为澄清液体,具有挥发性,通常密度小于水。所有的植物器官都能提取挥发油,如花蕾、花、叶、茎、小分支、种子果实、根、树干或树皮。提取挥发油的方法有多种,如超临界流体取、微波辅助萃取、水蒸气蒸馏、有机溶剂萃取。由于挥发油具有抗微生物和杀灭真菌的活性能够取代化学杀菌剂而在制药和食品领域得到越来越广泛的应用。在这种情况下,水蒸气蒸馏法和压榨法常被使用,如柑橘挥发油的提取。在香精领域,常常运用超临界流体萃取和水蒸气蒸馏法提取挥发油。提取的挥发油会因为植物的生长气候、土壤环境、植物器官、生长年龄和周期的不同而在挥发油含量、质量和化学成分上存在差异[1-2]。因此,为了获得成分基本一致的挥发油,通常选择植物的相同部位进行提取,且这些植物的土壤环境一样、生长气候一样、采摘季节一样。许多商品化的挥发油都要用气相色谱和质谱联用来分析成分。通过分析报告来保证挥发油的质量[3]
本章采用提取挥发油最常用的水蒸气蒸馏法,提取丁香花蕾油、香茅油、山苍子油,并用GC、GC-MS分析每种挥发油的成分,确定各种油的主要成分的相对含量。
2.2 材料和方法
2.2.1 主要原料及试剂
丁香花蕾:2009年采摘于中国广东,室温条件下自然风干;香茅:2009年采摘于中国广东,室温条件下自然风干;山苍子果实:2009年采摘于中国广东,室温条件下自然风干;无水硫酸钠(国药集团化学试剂有限公司);正构烷烃C8~C40(北京百灵威科技有限公司)。
2.2.2 主要仪器
气质联用仪(ThermoTrace GC/Ultra-DSQI );油水分离器(武汉大学科教仪器厂);气相色谱仪(Thermo Trace GC ULTRA);密度折光联用仪(Antonpaar股份有限公司);电热套(巩义市予华仪器有限公司)。
2.2.3 挥发油提取的单因素条件实验
山苍子挥发油提取单因素条件实验:选择优质的山苍子,提取的粒径选择未粉碎、粉碎至20目、粉碎至40目、粉碎至60目、粉碎至80目五个水平;浸泡时间分别采用0小时、2 小时、4 小时、6 小时、8 小时、10 小时和 12小时七个水平;料液比 1:4、1:6、1:8、1:10、1:12、1:14六个水平;提取时间为2小时、4小时、6 小时、8小时、10小时五个水平。分别进行单因素实验
丁香花蕾挥发油提取单因素条件实验:选择优质的丁香花蕾,提取的粒径选择未粉碎、粉碎至 20目、粉碎至40目、粉碎至60目、粉碎至80目五个水平;浸泡时间采用0小时、2 小时、4 小时、6 小时、8 小时、10 小时、12 小时七个水平;料液比 1:4、1:6、1:8、1:10、1:12、1:14 六个水平;提取时间为 2小时、4 小时、6 小时、8 小时、10 小时五个水平。分别进行单因素实验。
香茅叶挥发油提取单因素条件实验:选择优质的香茅叶,提取的粒径选择整叶、剪碎、粉碎至20目、粉碎至40目、粉碎至60目5个水平;浸泡时间采用0小时、2 小时、4 小时、6 小时、8 小时五个水平;料液比 1:4、1:6、1:8、1:10、1:12、1:14 六个水平;提取时间为 2 小时、4 小时、6 小时、8 小时、10小时五个水平。分别进行单因素实验。
挥发油得率(%)=挥发油质量(g)/提取原料质量(g)x100%
2.2.4 最优条件下水蒸气蒸馏法提取挥发油
三种植物挥发油的提取如文献报道[4.5],只做了少量的修改,具体如下所述:山苍子油:取山苍子果300克粉碎,过筛,放入挥发油提取装置,加入10倍质量的1%的氯化钠溶液,浸泡8小时后,水中蒸馏6小时,油水分离器中收集山苍子油。向山苍子油中加入适量的无水硫酸钠,静置2小时,过滤,得到的挥发油称重,然后在 4℃ 冷藏柜中密封避光保存待用。
丁香花蕾油:取丁香花蕾300克粉碎,过,放入挥发油提取装置,加入12倍质量的1%的氯化钠溶液,浸泡6小时后,水中蒸馏6小时,油水分离器中收集丁香花蕾油。向丁香花蕾油中加入适量的无水硫酸钠,静置2小时,过滤,得到的挥发油称重,然后在4℃冷藏柜中密封避光保存待用。
香茅油:取香茅叶300克粉碎,过,放入挥发油提取装置,加入8倍质量的1%的氯化钠溶液,浸泡4小时后,水中蒸馏4小时,油水分离器中收集香茅油。向香茅油中加入适量的无水硫酸钠,静置2小时,过滤,得到的挥发油称重,然后在4℃冷藏柜中密封避光保存待用。
2.2.5 挥发油成分分析
GC-MS 分析条件:
毛细管柱:HP5-MS(30mx0.25mmi.d.x0.25 um d.f);进样口温度:250℃;升温程序:起始柱温50℃ ,保持2min,5℃min 升温至250℃,保持15min;载气:He,流速 1.0mL/min;样品用无水乙醇稀释100倍;进样量:1μL,分流比 50:1;质谱接口温度:250℃:电离方式:EI:电离能量:70eV:离子源温度:250℃:质量扫描范围:41-350amu。采用Wiley和Nist谱检索、人工图谱解析以及查对质谱相关文献进行定性。正构烷烃C~C的混合标样用相同的分析条件分析来计算保留指数。
GC-FID 分析条件:
GC-FID分析条件与GC-MS相似,但是载气为氮气。挥发油各组分的相对含量在没有使用矫正因子的条件下通过GC-FID峰面积计算而来。
2.3 实验结果
2.3.1 水蒸气蒸馏法提取挥发油工艺优化
2.3.1.1 水蒸气蒸馏法提取山苍子挥发油工艺优化
2.3.1.1.1 不同提取粒径对山苍子挥发油得率的影响
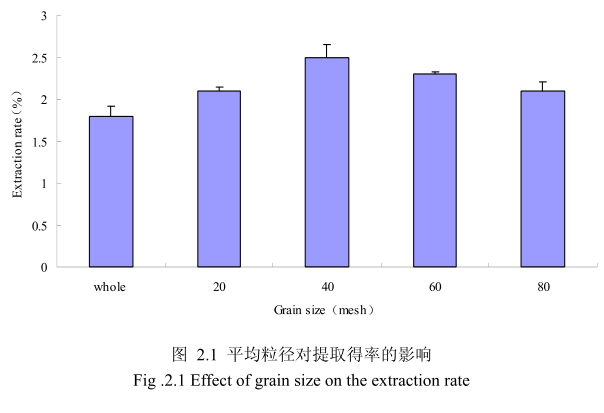
选择提取浸泡时间6小时、料液比1:8(质量比)、提取时间6小时、提取的粉碎粒径为未粉碎、粉碎至20目、粉碎至40目、粉碎至60目、粉碎至80目进行提取实验,实验结果如图2.1所示。从图中可以看出,当山苍子的提取粒径从未粉碎、粉碎至20目到粉碎至40目的过程中,山苍子油的得率随着粉碎粒径的变细而增大,当粉碎粒径为40目时,挥发油的得率最高。该过程中由于山苍子粉碎的越细,比表面积就越大,越有利于挥发油的浸出,所以挥发油的得率随着粉碎粒径的变小而增大。但是,当山苍子的粉碎粒径变为60目和80目时,山苍子油的得率反而下降。这可能是由于粉碎粒径的变小让颗粒比表面积增大的同时,颗粒自身的表面吸附作用增加,从而抑制了挥发油的扩散。同时,挥发油具有较强的挥发性,当粉碎粒径过细时,粉碎过程中会有少量的挥发油挥发损失掉,从而降低了挥发油的最终得率。因此,从本实验可以看出,山苍子的提取平均粒径控制在40目时挥发油的得率最高。
2.3.1.1.2 不同浸泡时间对山苍子挥发油得率的影响
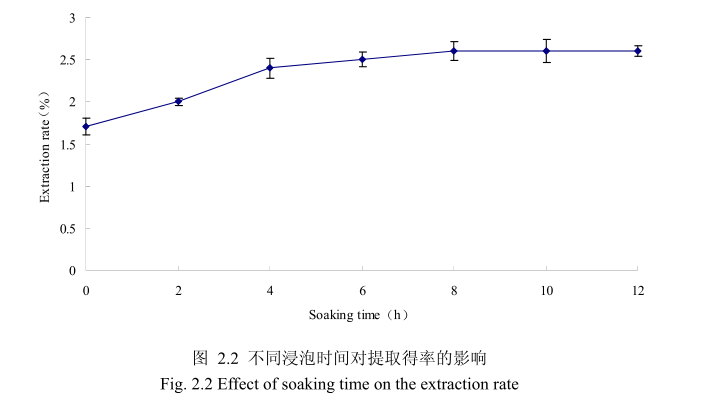
选择提取粒径为40目、料液比1:8(质量比)、提取时间6小时、提取的浸泡时间为0小时、2 小时、4 小时、6 小时、8 小时、10 小时、12 小时进行提取实验,从上图2.2可以看出,浸泡时间在0到8小时时间范围内,山苍子挥发油提取率随着浸泡时间的延长而增大。当浸泡时间为8小时,挥发油的得率达到较大值,随着浸泡时间的进一步延长,挥发油的得率几乎没有变化。造成这种现象的原因可能是由于浸泡过程可以使植物的细胞间隙增大,细胞组织充分膨胀,从而加速细胞内外的液体交换与平衡。由于山苍子质地较为坚硬,吸水性较差,因此需要浸泡较长时间才能让细胞组织充分膨胀。但是当浸泡达到一定时间后,细胞内外液体交换已经达到平衡,所以浸泡时间的进一步延长并不能改变精油的提取率。因此,选择浸泡时间为8小时时提取效率最高。
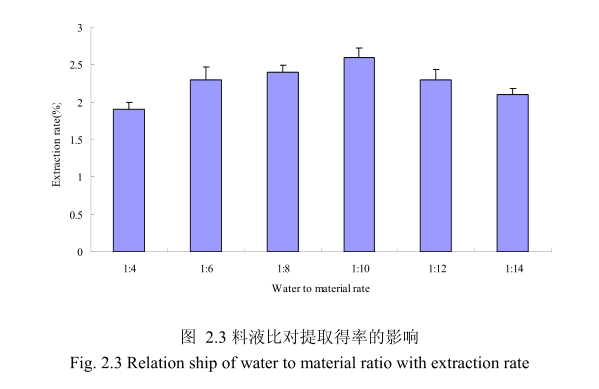
2.3.1.1.3 不同料液比对山苍子挥发油得率的影响
选择提取粒径40目,浸泡时间8小时,提取时间6小时,料液比为 1:4、1:6、1:8、1:10、1:12、1:14进行单因素实验。实验结果如图 2.3 所示,从图中可以发现,料液比从 1:4变化到1:10的过程中山苍子油的得率逐渐增加,料液比为1:10时山苍子油的得率最大。得率增加的原因可能是由于水的增多使山苍子中的山苍子油与水接触面处的浓度差变大,有利于山苍子油从组织中扩散出来。但当料液比从1:10 变化到 1:14 的过程中山苍子油的得率反而逐渐减少。可能由于水的增加,造成挥发油在水中的损耗增加,但是水量增加到一定程度对丁香花蕾油的扩散作用的影响已经不大,所以挥发油的得率降低。因此,当料液比为1:10时山苍子油的得率最高。
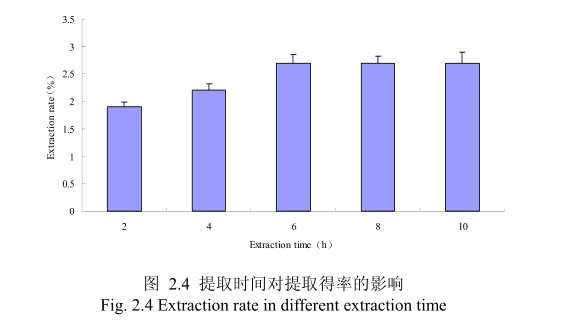
2.3.1.1.4 不同提取时间对山苍子挥发油得率的影响
选择提取粒径为40目、料液比1:10(质量比)、浸泡时间8小时、提取时间为2小时、4 小时、6 小时、8小时、10小时进行提取实验,从图 2.4 中可以看出随着提取时间的不断延长,山苍子油的得率显著提高,当提取时间达到6小时时,山苍子油的得率达到较大值,随着提取时间的进一步延长,山苍子油的得率并没有显著的变化。所以可以推测,当山苍子提取到6小时时,体系的渗透压达到平衡,提取率趋于恒定,随着加热时间的延长,挥发油的提取效率并不能提高。
2.3.1.2 水蒸气蒸馏法提取丁香花蕾挥发油工艺优化
2.3.1.2.1 不同提取粒径对丁香花蕾挥发油得率的影响
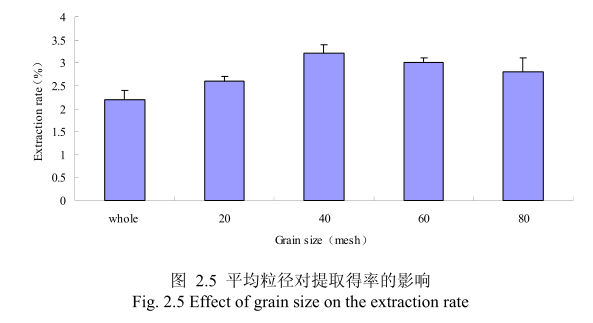
选择提取浸泡时间6小时、料液比1:8(质量比)、提取时间6小时、丁香花蕾的粉碎粒径分别为未粉碎、20目、40目、60目、80 目时进行提取实验,实验结果如图2.5所示。从图中可以看出,当丁香花蕾的提取粒径从未粉碎、粉碎至20目到粉碎至40目的过程中,丁香花蕾油的得率随着粒径的变细而增大,当粉碎粒径为 40目时,挥发油的得率最高。该过程中由于丁香花蕾粉碎的越细,比表面积就越大,越有利于挥发油的浸出,所以挥发油的得率随着粉碎粒径的变小而增大。但是,当丁香花蕾的粉碎粒径变为60目和80目时,丁香花蕾挥发油的得率反而下降。这可能是由于粉碎粒径的变小让颗粒比表面积增大的同时,颗粒自身的表面吸附作用增加,从而抑制了挥发油的扩散。同时,挥发油具有较强的挥发性当粉碎粒径过细时,粉碎过程中会有少量的挥发油挥发损失掉,从而降低了挥发油的最终得率。因此,从本实验可以看出,丁香花蕾的提取平均粒径控制在40目时挥发油的得率最高。
2.3.1.2.2 不同浸泡时间对丁香花蕾挥发油得率的影响
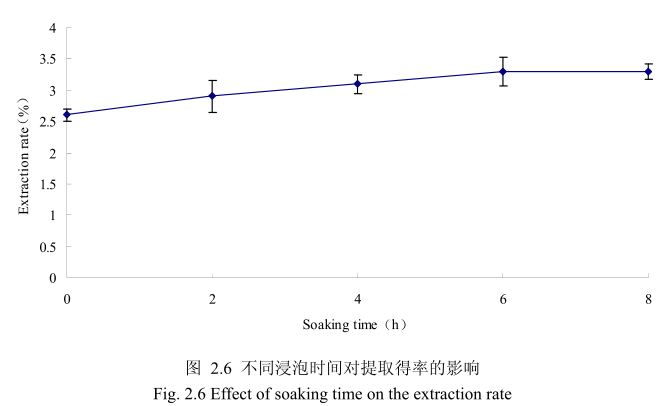
选择丁香花蕾粒径为40目、料液比1:8(质量比)、提取时间6小时。提取的浸泡时间分别为0小时、2小时、4 小时、6小时、8 小时进行提取实验,从图 2.6可以看出,浸泡时间在0到6小时时间范围内,丁香花蕾挥发油提取率随着浸泡时间的延长而增大。当浸泡时间为6小时时,挥发油的得率达到较大值,随着浸泡时间的进一步延长,挥发油的得率几乎没有变化。造成这种现象的原因可能是由于浸泡过程可以使植物的细胞间隙增大,细胞组织充分膨胀,从而加速细胞内外的液体交换与平衡。但是当浸泡达到一定时间后,细胞内外液体交换已经达到平衡,所以浸泡时间的进一步延长并不能改变挥发油的提取率。因此,选择浸泡时间为6小时时提取效率最高。
2.3.1.2.3 不同料液比对丁香花蕾挥发油得率的影响
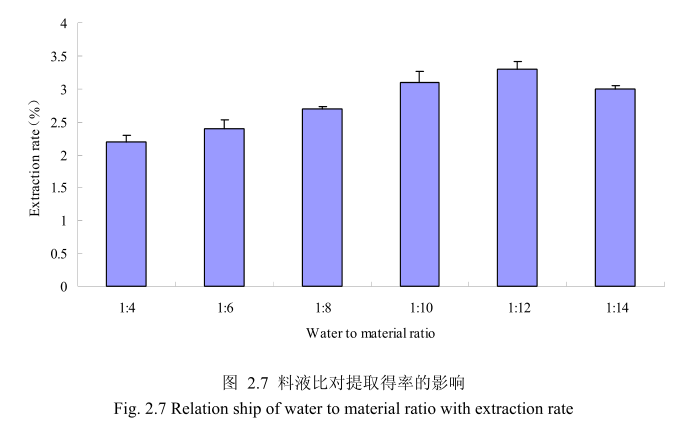
选择丁香花蕾粒径40目,浸泡时间6小时,提取时间6小时,料液比为1:4、1:6、1:8、1:10、1:12、1:14进行单因素实验。实验结果如图 2.7 所示,从图中可以发现,料液比从1:4变化到1:12的过程中丁香花蕾油的得率逐渐增加,料液比为1:12时丁香花蕾油的得率最大。得率增加的原因可能是由于水的增多使丁香花蕾中的丁香花蕾油与水接触面处的浓度差变大,有利于丁香花蕾油从组织中扩散出来。但当料液比从1:12变化到1:14的过程中,丁香花蕾油的得率反而逐渐减少。可能由于水的增加,造成挥发油在水中的损耗增加,但是水量增加到一定程度对了香花蕾油的扩散作用的影响已经不大,所以挥发油的得率降低。因此,当料液比为1:12时丁香花蕾油的得率最高。
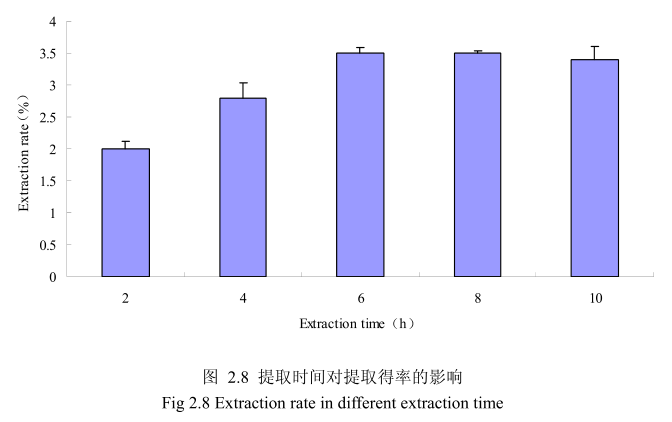
2.3.1.2.4 不同提取时间对丁香花蕾挥发油得率的影响
选择丁香花蕾粒径为40目、料液比1:12(质量比)、浸泡时间6小时、提取时间为2小时、4 小时、6小时、8小时、10 小时进行提取实验,从图2.8中可以看出随着提取时间的不断延长,丁香花蕾挥发油的得率显著提高,当提取时间达到6小时时,丁香花蕾挥发油的得率达到较大值,随着提取时间的进一步延长,丁香花蕾挥发油的得率并没有显著的变化。所以可以推测,当丁香花蕾提取到6时时体系的渗透压达到平衡,提取率趋于恒定,随着加热时间的延长,挥发油的提取效率并不能提高。
2.3.1.3 水蒸气蒸馏法提取香茅叶挥发油工艺优化
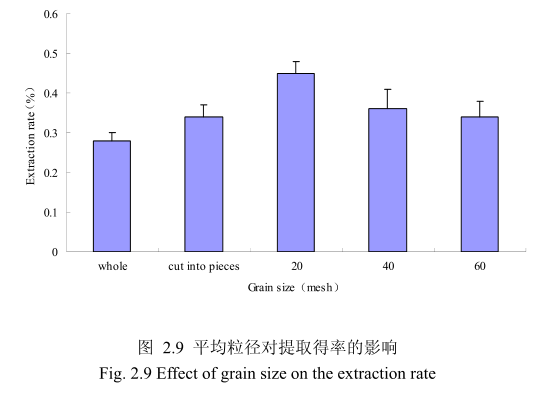
2.3.1.3.1 不同提取粒径对香茅叶挥发油得率的影响
不同提取粒径对香茅叶挥发油的提取得率有一定的影响。选择提取浸泡时间6小时、料液比 1:10(质量比)、提取时间6小时、提取的粉碎粒径为整叶、剪碎、粉碎至20目、粉碎至40目、粉碎至60目进行提取实验,实验结果如图2.9所示。从图中可以看出,当香茅叶的提取粒径从整叶、剪碎到粉碎至 20目的过程中,香茅油的得率随着粉碎粒径的变细而增大,当粉碎粒径为20目时,挥发油的得率最高。该过程中由于香茅叶粉碎的越细,比表面积就越大,越有利于挥发油的浸出,所以挥发油的得率随着粉碎粒径的变小而增大。但是,当香茅叶的粉碎粒径变为40目和60目时,香茅挥发油的得率反而下降。这可能是由于粉碎粒径的变小让颗粒比表面积增大的同时,颗粒自身的表面吸附作用增加,从而抑制了挥发油的扩散。同时,挥发油具有较强的挥发性,当粉碎粒径过细时,粉碎过程中会有少量的挥发油挥发损失掉,从而降低了挥发油的最终得率。因此,从本实验可以看出,香茅叶提取平均粒径控制在20目时挥发油的得率最高。
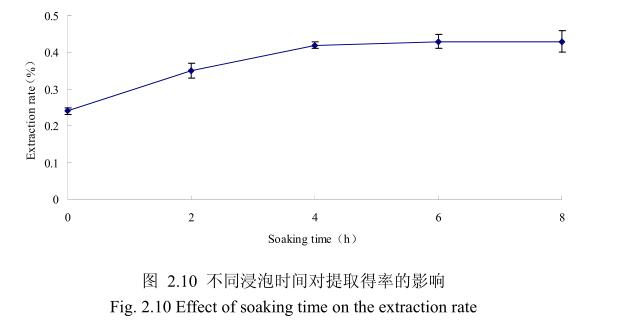
2.3.1.3.2 不同浸泡时间对香茅叶挥发油得率的影响
选择香茅叶粒径为20目、料液比1:10(质量比)、提取时间6小时、提取的浸泡时间分别为0小时、2小时、4 小时、6 小时、8 小时进行提取实验。从图2.10可以看出,在0到4时时间范围内,香茅叶挥发油提取率随着浸泡时间的延长而增大,在4小时时,挥发油的得率达到较大值,随着浸泡时间的进步延长,挥发油的得率几乎没有变化。造成这种现象的原因可能是由于浸泡过程可以使植物的细胞间隙增大,细胞组织充分膨胀,从而加速细胞内外的液体交换与平衡。但是当浸泡达到一定时间后,细胞内外液体交换已经达到平衡,所以浸泡时间的进一步延长并不能明显改变挥发油的提取率。因此,选择浸泡时间为4小时,此时提取效率最高。
2.3.1.3.3 不同料液比对香茅叶挥发油得率的影响
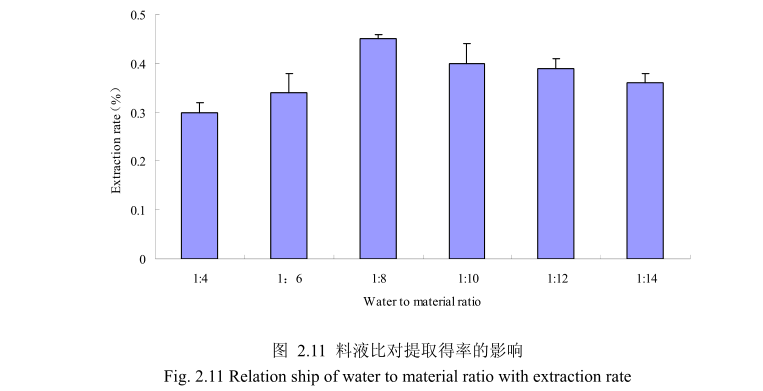
选择香茅叶粒径20目,浸泡时间4小时,提取时间6小时,料液比为1:4、1:6、1:8、1:10、1:12、1:14进行单因素实验。实验结果如图,从图中可以发现,料液比从1:4变化到1:8的过程中香茅叶油的得率逐渐增加,料液比为1:8时香茅叶油的得率最大。得率增加的原因可能是由于水的增多使香茅叶中的香茅油与水接触面处的浓度差变大,有利于香茅油的从叶片中扩散出来。但当料液比从1:8变化到1:14的过程中香茅油的得率反而逐渐减少。可能由于水的增加,造成挥发油在水中的损耗增加,但是水量增加到一定程度对香茅油的扩散作用的影响已经不大,所以挥发油的得率降低。因此,当料液比为1:8时香茅油的得率最高。
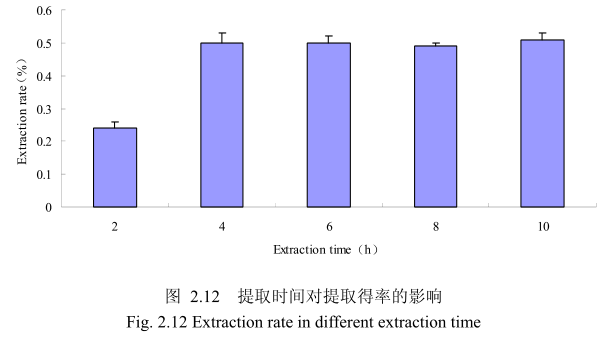
2.3.1.3.4 不同提取时间对香茅叶挥发油得率的影响
选择香茅叶粒径为20目、料液比1:8(质量比)、浸泡时间4小时、提取时间分别为 2小时、4 小时、6 小时、8 小时、10 小时进行提取实验,从图 2.12中可以看出随着提取时间的不断延长,香茅叶油的得率不断提高,当提取时间达到4小时时,香茅叶油的得率达到较大值,随着提取时间的进一步延长,香茅油的得率并没有显著的变化。所以可以推测,当香茅叶提取到4小时时,体系的渗透压达到平衡,提取率趋于恒定,随着加热时间的延长,挥发油的提取效率并不能提高。因此,当提取时间为4小时时,香茅油得率最高。
2.3.2 三种植物挥发油的物理指标
(1)丁香花蕾油:得率3.5%,澄清淡黄色液体,辛香及丁香酚的特征香气;相对密度 1.045(20/20℃);折光指数 1.5290(20℃)。
(2)山苍子油:得率2.7%,澄清淡黄色液体;感官特征:具有清鲜、甜的果香,类似柠檬油的香气;相对密度0.889(20/20℃);折光指数1.482(20℃)。
(3)香茅油:得率0.5%,澄清淡黄色液体;感官特征:具有轻快、新鲜的清甜果香,有成熟柠檬果皮的香气;相对密度0.889(20/20℃);折光指数 1.486(20℃)。
2.3.3 三种植物挥发油化学成分分析
2.3.3.1 山苍子油的化学成分
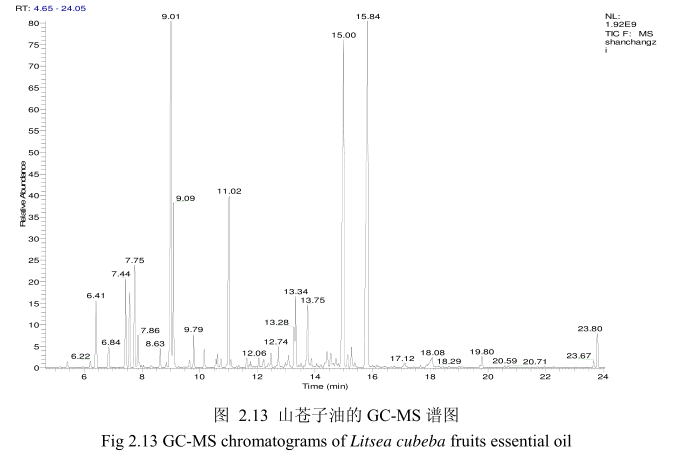
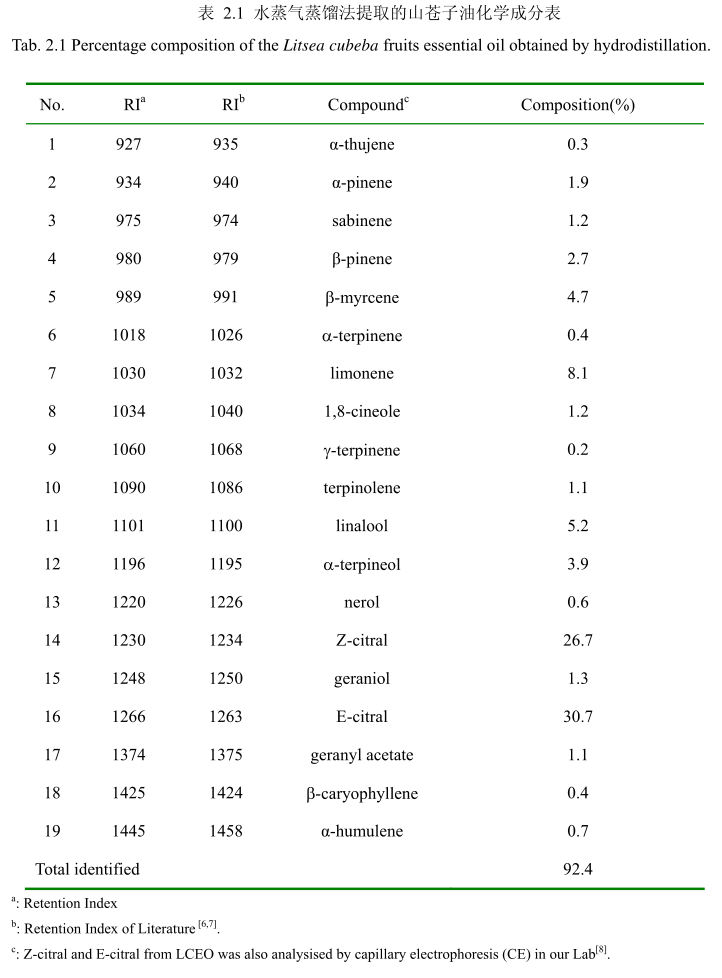
将最优提取条件下提取的山苍子油进行GC-MS分析。图2.13是山苍子油的GC-MS 图谱。从图2.13可以看出,山苍子油的化学成分较多,其中大多成分集中在保留时间5.0-25分钟之间。通过和标准品或质谱数据库数据比对,鉴定出19种化学成分,占总油含量的92.4%。表2.1为山苍子油成分和含量统计表。从表2.1可看出,广东产的山苍子果挥发油中相对含量较高的成分有E-柠醛(30.7%);Z-柠檬醛(26.7%);柠檬烯(8.1%);芳樟醇(5.2%);B-月桂烯(4.7%);a-松油醇(3.9%);B-蒎烯(2.7%);a-蒎烯(1.9%);香叶醇(1.3%);1.8-桉叶素(1.2%)等。
2.3.3.2 丁香花蕾油的化学成分
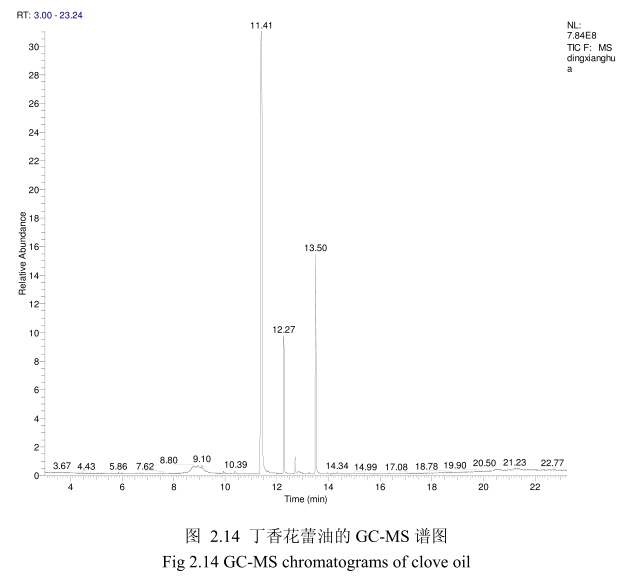
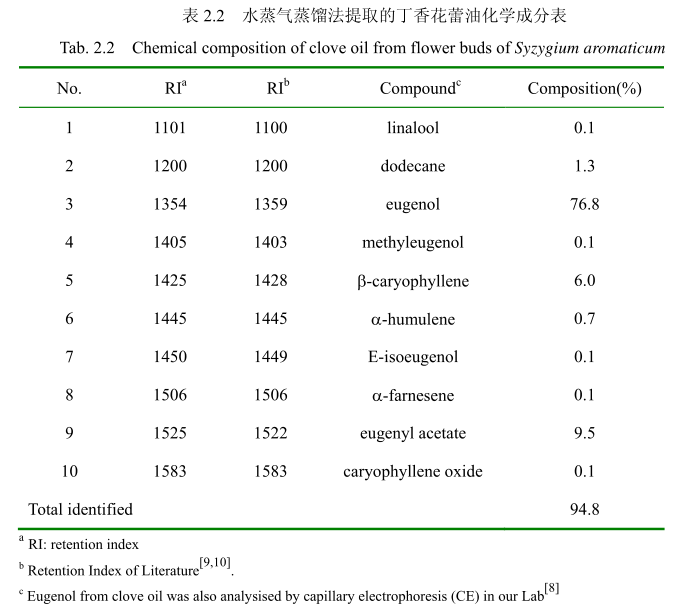
将最优提取条件下提取的丁香花蕾油通过GC-MS分析。图2.14是丁香花蕾油的GC-MS 图谱。从图2.14可以看出,丁香花蕾油的化学成分大多集中在保留时间 3.5-25分钟之间。通过和标准品或质谱数据库数据比对,鉴定出10种化学成分,占总油含量的94.8%。表2.2为鉴定出的丁香花蕾油成分和含量。从表2.2可看出,广东产的丁香花蕾油中相对含量较高的成分有丁香酚(76.8%)、乙酸丁香酯 (9.5%)、B-石竹烯(6.0%)、E-3-十二烯(1.9%)、2-1-十二烯(1.3%)等。
2.3.3.3.香茅油化学成分
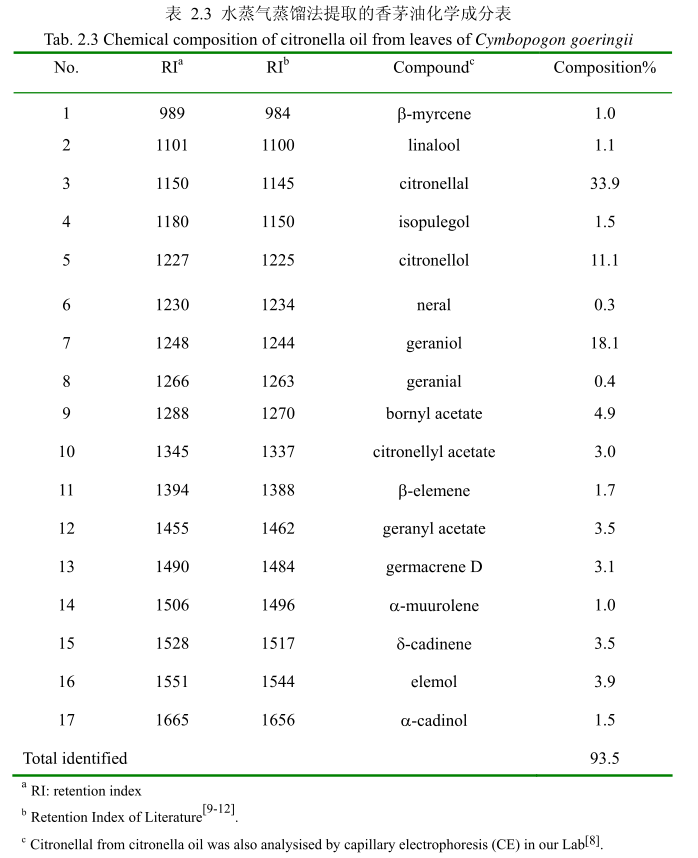
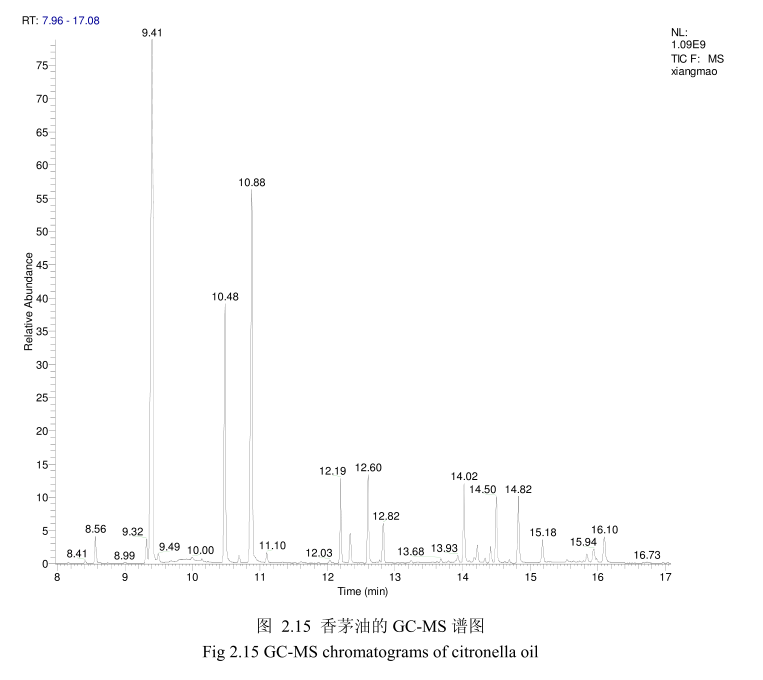
将最优提取条件下提取的香茅油通过GC-MS分析。图2.15是香茅油GC-MS图谱。从图2.15可以看出,香茅油的化学成分大多集中在保留时间6.0-17分钟之间。通过和标准品或质谱数据库数据比对,鉴定出17种化学成分,占总油含量的93.5%。表2.3为鉴定出的香茅油成分及含量。从表2.3可看出,其相对含量较高的成分为香茅醛(33.9%)、香叶醇(18.1%)和香茅醇(11.1%)等。
2.4 讨论
挥发油是一种成分非常复杂的天然混合物,通常含有20-60种成分,并且其含量差异很大。挥发油通常含有两种或三种主要特征成分,每种的含量可达20%-70%,而有些成分的含量非常少。通常情况下,挥发油的主要成分决定了挥发油的生物活性。挥发油的成分包含两类[13-16]。其中主要的一类由萜烯类和萜类化合物组成,另外一类由芳香族和脂肪族化合物组成,都属于小分子化合物。
萜类化合物是植物次生代谢产物,在自然界分布广泛,由异戊二烯单元组成的化合物及其衍生物,按照碳原子的数目可以分为单萜、倍半萜、二萜、三萜和多萜等。由于萜类化合物分子中具有不同的碳环数,因此又可分为链萜、单环萜、双环萜和三环萜等[17]。单萜由两个异戊二烯单元组成,是挥发油中最有代表性的分子,占挥发油组分的 90%,包含:桂叶烯、罗勒、萜品烯、水芹烯、香叶醇、芳樟醇香茅醇,、熏衣草醇、香橙醇、薄荷醇、松油醇、龙脑、小茴香醇、香叶醛、橙花醛香茅醛、薄荷酮、香芹酮、薄荷酮、胡椒酮、乙酸芳樟酯、乙酸异冰片酯、桉油素麝香草酚、香芹酚等。当分子具有旋光性,两种对映异构体常常存在于不同的植物中。
芳香化合物衍生于苯基丙烷,其种类少于萜类。萜类和芳香化合物在植物中合成路径是分开的,但在某些植物中是共用一条合成路径。芳香类化合物包括:桂皮醛、肉桂醇、丁香酚、茴香脑、肉豆蔻醚等
挥发油是一种混合物,其化学成分会因为植物物种、生长的地理环境、提取方法、采收时间等因素的差异而不同[18,19]。本章运用水蒸气蒸馏法提取的自然晾干的山苍子果实的挥发油呈淡黄色。GC-MS分析水蒸气蒸馏法提取的山苍子油鉴定出19种化学成分,占总油的92.4%。其主要成分柠檬醛的相对含量占57.4%,柠檬烯的含量占 8.1%,芳樟醇的含量为5.2%,B-月桂烯的相对含量为4.7%,a-松油醇的相对含量为3.9%,β-烯的相对含量为2.7%,α-蒎烯的相对含量为1.9%。本章运用 GC-MS 分析的山苍子油的主要化学成分与其它相关文献报道的山苍子油的主要化学成分基本一致[20,21],但是比例不同,从而证明天然挥发油含量的差异性[22]。例如,同一种类的山苍子油,其产地为美国,主要成分柠醛的相对含量为 85.7%,柠檬烯的相对含量为2.9%,芳樟醇的相对含量为1.7%。Wang等[23]研究的山苍子油中柠檬醛的含量为63.75%,柠檬烯的相对含量为7.38%,甲庚酮的相对含量为 3.54%,烯的相对含量为2.87%,4-伞花烃的含量为2.14%。
同样用GC-MS 分析产于中国广东的丁香花蕾油,鉴定出10种物质,占总油的 94.8%。主要成分丁香酚的相对含量为76.8%,乙酸丁香酯的相对含量为 9.5%,B-石竹烯的相对含量为6.0%。尽管其主要成分与其它文献报道的一致,但是其含量不一致。如产地为意大利的丁香花蕾油中丁香酚的相对含量为70.8%,B-石竹烯的相对含量为 24.9%,乙酸丁香酯的含量为4.2%。Moon 等[24]报道的丁香花蕾油中丁香酚的相对含量为76.8%,B-石竹烯的相对含量为17.4%,乙酸丁香酯的相对含量为 1.2%。
用GC-MS分析的香茅叶的挥发油鉴定出17种成分,占总油的93.5%。其中主要成分香茅醛的相对含量为33.9%、香叶醇的相对含量为18.1%、香茅醇的相对含量为11.1%。其主要成分与相关文献报道的香茅油的主要化学成分一致,但是其比例有一点差异。如中国云南产的香茅挥发油中主要成分香茅醛的含量为36.055%,香叶醇的含量为21.33%。
从本章分析的三种天然挥发油与其相关文献报道的结果相比较可以看出,尽管其主要化学成分一致,但是其含量有一定差异。而挥发油的化学成分及其含量决定了其生物活性,因此其挥发油的生物活性也可能存在较大差异。
2.5 本章小结
本章运用水蒸气蒸馏法萃取了产地中国广东的山苍子果实、丁香花蕾、香茅叶,获得挥发油的理化指标如下:
(1)山苍子油得率2.7%,澄清淡黄色液体;感官特征:具有清鲜、甜的果香,类似柠檬油的香气;相对密度0.889(20/20℃);折光指数1.482(20℃)。通过单因素实验,山苍子挥发油最佳提取工艺参数为山苍子粉碎至40目,浸泡时间8小时,料液比1:10,提取时间6小时。GC-MS分析山苍子油鉴定出19种化学成分,占总油的92.4%。其主要成分柠檬醛的相对含量占57.4%,柠烯的含量占8.1%,芳樟醇的含量为5.2%,B-月桂烯的相对含量为4.7%,a-松油醇的相对含量为3.9%,B-烯的相对含量为2.7%,a-的相对含量为1.9%。
(2)丁香花蕾油,得率3.5%,澄清淡黄色液体,辛香及丁香酚的特征香气;相对密度 1.045(20/20℃);折光指数15290(20℃)。通过单因素实验,丁香花蕾挥发油最佳提取工艺参数为丁香花蕾粉碎至40目,浸泡时间6小时,料液比1:12,提取时间6小时。用GC-MS 分析丁香花蕾油,鉴定出10种物质,占总油的94.8%。主要成分丁香酚的相对含量为76.8%,乙酸丁香酯的相对含量为9.5%,B-石竹烯的相对含量为6.0%。
(3)香茅油得率0.5%,澄清淡黄色液体;感官特征:具有轻快、新鲜的清甜果香,有成熟柠檬果皮的香气;相对密度0.889(20/20℃);折光指数 1.486(20℃)通过单因素实验,香茅叶挥发油最佳提取工艺参数为香茅粉碎至20目,浸泡时间4小时,料液比1:8,提取时间4小时。GC-MS 分析的香茅叶的挥发油鉴定出 17种成分,占总油的93.5%。其中主要成分香茅醛的相对含量为33.9%、香叶醇的相对含量为 18.1%、香茅醇的相对含量为11.1%。
2.6参考文献
[1] Masotti V, Juteau F, Bessie 're JM. Seasonal and phenological variations of the essential oil from the narrow endemic species Artemisia molinieri and its biological activities. Journal of Agricultural and Food Chemistry, 2003, 51:7115- -7121
[2] Jirovetz L, Buchbauer G, Stoilova I, et al. Chemical composition and antioxidant properties of clove leaf essential oil. Journal of Agricultural and Food Chemistry, 2006, 54(17):6303-6307
[3] Smith R, Cohen S, Doull J, et al. A procedure for the safety evaluation of natural flavor complexes used as ingredients in food: essential oils. Food and Chemical Toxicology, 2005, 43(3):345-363
[4]Huang B, Ban X, He J, et al. Comparative analysis of essential oil components and antioxidant activity of extracts of Nelumbo nucifera from various areas of China. Journal of Agricultural and Food Chemistry, 2009, 58(1):441-448
[5]Wang Q, Yang Y, Zhao X, et al. Chemical variation in the essential oil of Ephedra sinica from Northeastern China. Food Chemistry, 2006, 98( 1):52-58
[6] Wang HW, Liu YQ. Chemical composition and antibacterial activity of essential oils from different parts of Litsea cubeba. Chemistry & Biodiversity, 2010,7:229-235.
[7]Mockute D, Bernotiene G. The main citral-geraniol and carvacrol chemotypes of the essential oil of Thymus Pulegioides L. growing wild in Vilnius District (Lithuania). Journal of Agricultural and Food Chemistry,1999, 47: 3787-3790
[8]Huang XW, Yi L,Gao ZH, et al. Determination of seven active ingredients in three plant essential oils by using micellar electrokinetic chromatography. Analytical Letters, 2012,45, 2014-2015
[9]Jirovetz L, Buchbauer G, Stoilova I, et al. Chemical composition and antioxidant properties of clove leaf essential oil. Journal of Agricultural and Food Chemistry, 2006, 54, 6303-6307
[10] Kiran SR, Reddy AS, Devi PS,et al. Reddy, Insecticidal, antifeedant and oviposition deterrent effects of the essential oil and individual compounds from leaves of Chloroxylon swietenia DC. Pest Management Science, 2006, 62:1116-1121
[11] Lota ML, Serra DD, Tomi F,et al. Volatile components of peel and leaf oils of Lemon and Lime Species. Journal of Agricultural and Food Chemistry, 2002, 50:796-805
[12] Rajeswara R, Bhattacharya AK, Mallavarapu GR,et al. Yellowing and crinkling disease and its impact on the yield and composition of the essential oil of citronella (Cymbopogon winterianus Jowitt). Flavour Fragrance Jourmal, 2004, 19:344-350
[13]Da Silva EB, Matsuo AL, Figueiredo CR, et al. Chemical constituents and cytotoxic evaluation of essential oils from leaves of Porcelia macrocarpa(Annonaceae). Natural Product Communications, 2013, 8(2):277-279
[14]Betts TJ. Chemical characterisation of the different types of volatile oil constituents by various solute retention ratios with the use of conventional and novel commercial gas chromatographic stationary phases. Journal ofChromatography A, 2001, 936(1):33-46
[15]Setzer WN. Essential oils and anxiolytic aromatherapy. Natural Product Communications,2009,4(9): 1305-1316.
[16] Pichersky E, Noel JP, Dudareva N. Biosynthesis of plant voltiles: nature's diversity and ingenuity. Science Signaling, 2006, 311(5762):808-811
[17] 张长波,孙红霞,巩中军.植物萜类化合物的天然合成途径及其相关合酶.植物生理学通讯,2007,43(4) :779-785
[18] Lota ML, De Rocca Serra D, Tomi F, et al. Volatile components of peel and leaf oils of lemon and lime species. Journal of Agricultural and Food Chemitry, 2002, 50(4):796-805
[19] Lalko J, Api A. Investigation of the dermal sensitization potential of various essential oils in the local lymph node assay. Food and Chemical Toxicology, 2006, 44(5):739-746
[20] Gao Z, Xu H, Chen X, et al. Antioxidant status and mineral contents in tissues of rutin and baicalin fed rats. Life Sciences, 2003, 73(12):1599-1607
[21] Ho CL, Jie-Pinge O, Liu YC, et al. Compositions and in vitro anticancer activities of the leaf and fruit oils of Litsea cubeba from Taiwan. Natural Product
Communications, 2010, 5(4):617-620
[22] Liu ZL, Liu QR, Chu SS, et al. Insecticidal activity and chemical composition of the essential oils of Artemisia lavandulae folia and Artemisia sieversiana from China. Chemistry & Biodiversity, 2010, 7(8):2040-2045
[23] Wang H, Liu Y. Chemical composition and antibacterial activity of essential oils from different parts of Litsea cubeba. Chemistry & Biodiversity, 2010,
7(1):229-235
[24] Moon SE, Kim HY, Cha JD. Synergistic effect between clove oil and its major compounds and antibiotics against oral bacteria. Archives of Oral Biology, 2011 ,56(9):907-916
未完待续……
- 星期五, 21 6月 2024
三种植物挥发油的化学成分、酪氨酸酶抑制能 力及抗氧化活性的研究---绪论(一)
摘 要
随着大气层中臭氧的逐渐减少,地球表面的紫外线强度不断增加。高强度的紫外照射会引起皮肤色素的过度沉着和皮肤功能的紊乱。因此研发有效的祛斑、美白护肤品一直是化妆品领域的热门之一。近年来,出于安全性方面的考虑,人们更愿意接受源自天然中草药的美白护肤产品。中国是一个植物物种多样的国家,有许多药食同源的植物挥发油在民间被广泛地应用于护肤品,但其是否具有祛斑、美白的功能,却鲜有研究。本论文选取了三种各具独特功能的本土植物挥发油(丁香花蕾油、香茅油和山苍子油),通过系列实验,为判断其是否具有成为美白护肤品成分的潜能提供科学依据。
主要内容包含以下几个方面:
1、优化了提取山苍子油、丁香花蕾油和香茅油的提取工艺,并用气质联用技术鉴定了三种挥发油的主要成分。鉴定出山苍子油中的19种化学成分,占整个挥发油组分的 92.4%。主要成分有柠檬醛(57.4%),柠檬烯(8.1%),芳樟醇(5.2%),B-月桂烯(4.7%),α-松油醇(3.9%),β-蒎烯(2.7%)和a-蒎烯(1.9%);鉴定出丁香花蕾油中的 10种成分,占整个挥发油的94.8%。主要成分有丁香酚(76.8%),乙酸丁香酯(9.5%)和B-石竹烯(6.0%);鉴定出香茅油中的 17 种成分,占整个挥发油的 93.5%。主要成分有香茅醛(33.9%),香叶醇(18.1%),和香茅醇(11.1%)。
2、通过酪氨酸酶抑制试验来评价三种挥发油及其主要成分对酪氨酸酶的抑制效果。结果表明山苍子油和其主要成分柠檬醛对酪氨酸酶单酚酶和二酚酶活性有抑制能力,对酪氨酸酶二酚酶的抑制能力强于酪氨酸酶单酚酶,且动力学结果表明柠檬醛对酪氨酸酶是非竞争性抑制作用。丁香花蕾油和丁香酚对酪氨酸酶单酚酶具有一定的抑制作用,但是对酪氨酸酶二酚酶没有表现出任何抑制作用。而香茅油及其主要成分对酪氨酸酶没有抑制作用。
3、分别研究了山苍子油、香茅油、丁香花蕾油和其主要成分的抗氧化活性。
结果表明丁香花蕾油具有最强的自由基清除能力(超阴离子的ICo值为58g/mL;ABTS的ICso值为8.5μg/mL)和强的抑制脂质过氧化的能力;香茅油的自由基清除能力和抑制脂质过氧化的能力低于丁香花蕾油(超氧阴离子的ICso值为150 μg/mL;ABTS*的ICso值为 500μg/mL)。山苍子油的自由基清除能力最低(超氧阴离子的ICso值为10.2mg/mL;ABTS 的ICso值为 17.75 mg/mL)。
4、为了探讨山苍子油、丁香花蕾油和香茅油分别对 UV-TiO2-NO,体系导致的蛋白质氧化和酪氨酸硝化损伤的抑制作用,将牛血清蛋白作为模型蛋白进行体外试验,采用免疫印迹法测定牛血清白蛋白的氧化和酪氨酸硝化。结果表明丁香花蕾油、香茅油和山苍子油对UV-TiO,-NO,-催化的蛋白质氧化和酪氨酸硝化都有较强的抑制效果且呈剂量依耐性。
关键词:挥发油,酪氨酸酶,抗氧化,纳米二氧化钛,蛋白质氧化,蛋白质酪氨酸硝化
Abstract
Ultraviolet (UV) radiation on the surface of the earth is certainly increasing as a result of the depletion of stratospheric ozone. High-intensity or accumulated UV radiation provokes many hyperpigmentation disorders, which are of particular concern to women as well as men, In recent years, the study of traditional herbal medicines for skin-protecting and skin-lighting has become a hot spot in the cosmetics field, due to various safety concerns and interesting largely unexplored sources. In this dissertation. the main objective was to investigate the potential usage of clove oil , citronella oil and Litsea cubeba oil as natural sources of tyrosinase inhibitor, antioxidant, and protectionprotein against UVTiO,-NO2- induced protein oxidation and tyrosine nitration in jury The main results are as follows:
1. The clove oil, citronella oil and Litsea cubeba oil extracted by hydrodistillation, showed light yellow in color. The total of 10 compounds was identified by GC-MS in the clove oil, accounting for 94.8% of the total oil. The main components were eugenol(76.8%), followed by eugenyl acetate (9.5%) and β-caryophyllene (6.0%). Essential oil from Cymbopogon goeringii leaves was also analyzed by GC-MS, resulted in the identification of 17 compounds representing 93.5% of the oil. Citronellal (33.9%),geraniol (18.1%), and citronellol (11.1%) were the main compounds. GC-MS analyses of Litsea cubeba oil led to identification of 19 different compounds, accounting for 92.4%of the total oil. The main components were citral representing 57.4% of the total amount of oil extracted, follow by limonene(8.1%),linalool (5.2%),β-myrcene (4.7%),a-terpineol (3.9%),β-pinene(2.7%) and a-pinene(1.9%%).
2. Tyrosinase inhibitory assay was used to evaluate whether the three essential oilsand their main components possessed potential inhibitory effect on tyrosinase. The results show that Litsea cubeba oil and citral exhibited inhibitory effect on monophenolase and diphenolase activity of tyrosinase. The inhibitory effect of Litseacubeba oil and citral on diphenolase activity was stronger than monophenolase activity oftyrosinase. The inhibition pattern of mushroom tyrosinase by citral was determined byLineweaver-Burk polt analysis. The results demonstrated that citral was anoncompetition tyrosinase inhibitor, Clove oil and eugenol exhibited some inhibitoryeffect on monophenolase activity of` tyrosinase, but not show any inhibitory effect on diphenolase activity of tyrisinase. Citronella oil and their main components didn'texhibited any inhibitory effect.
3. In order to determine whether the three essential oils and their main components had antioxidant activity, ABTS cation radical scavenging assay, superoxide anion radicalscavenging assay and lipid peroxidation assay were carried out. Clove oil exhibited prominent radical scavenging activities (ICso: 58 μg/ mL for O2 and 8.5 ug/ mL for ABTS*) and strong inhibitory effect on lipid peroxidation, whilst citronella oil showedweaker antioxidative activities (ICso: 150 μg/ mL for O, and 500 μg/ mL for ABTS )and lipid peroxidation inhibitory efficiency. Litsea cubeba oil exhibited the lowest anti-oxidative activities (ICso: 17.75 mg/mL for ABTS , 10.2 mg/mL, for O, ).
4. In order to investigate inhibitory effects of essential oils to UV-TiO,-NOzinduced protein oxidation and protein tyrosine nitration injury, bovine serum albumin(BSA) were used as model protein, inhibition were followed by $DS-PAGE and Western blotting methods. The results showed that clove oil, citronella oil and Litsea cubeba oil exhibited satisfactory protective effects and revealed dose-dependence in protecting BSAagainst UV - TiO, - NO,` induced protein oxidation and tyrosine nitration injury.
Keywords: essential oil, tyrosinase, antioxidant, nano TiO2, protein oxidation, tyrosine nitration
- 星期四, 20 6月 2024
红缨合耳菊防晒成分的提取及其性能
徐春涛1,马飞2,纪红兵2
(1中山职业技术学院信息工程学院,2广东中山528404:中山大学化学与化学工程学院,广东广州510275)
摘要:红缨合耳菊属于西藏特有的菊科植物,其有潜在的美白及防晒效果。本文选择水、正已烷、乙醚和乙醉为溶剂,考察 4种草取溶剂提取液的紫外吸收效果,并结合最佳革取溶剂,考察不同提取工艺对红撄合耳莉防晒成分提取率的影响。结果表明,采用超声波提取工艺,以乙醇为萃取溶剂效果最佳,整体提取率为27%。采用气质联用仪(GC-MS)对红缨合耳菊提取液成分进行分析,研究发现提取物中含有较多的共双体系化合物,这些化合物分别是 3-亚甲基-6-(1-甲基乙基)环已烯、菜烯、环已烯等,带有共轭双键体系的化合物具有较强的紫外吸收效果,将红缨合耳菊提取液制成防晒霜,发现含有质量分数2.5%的红缨合耳菊提取物防晒霜在UVB(290~320nm)段禁外线区具有很好的禁外线防护功能,平均吸光度值为1.95。
关键调:红缨合耳药:防晒剂:防晒霜:提取物:紫外线中图分类号:TO658.2文献标志码:
A文章编号:1000-6613(2017)04-1429-05
DO1:10.16085/.issn.1000-6613.2017.04.037
Sunsereen ingredients of synotis erythopappa(Bur.et Franch)C. Jeffey et Y.L.Chen and its application in sun cream
XU Chuntao1, MA Fei2 . .JI Hongbing2
('College of Information Engineering, Zhongshan Polytechnic, Zhongshan 528404. China: 'School of Chemistry and
Chemical Engineering, Sun Yat-sen University, Guangzhou 510275,Guangdong. China)
Abstract: Synotis erythopappa ( Bur.et Franch) C. Jeffeyet Y. L Chen, as an endemic compositae in Tibete. has potential benifits in whitening and sun blocking. In this paper, four different solvents
(water, hexane, aether and alcohol) were used to extract the plant, respectively. The extraction was investigated by testing actual UV absorbtion value. Using the best extract solvent, different extract
technologies were used to evaluate the effectiveness of the extraction. The results showed thatethanol, as the extract solvent and combing with ultrasonic extraction technology, the exctraction rate was up to 27%. Gas chromatographymass spectrometer (GC-MS ) was used to analyze the sun block components from extract solvent. It was found that 3-methylenc-6-( l-methyl ethyl) cyclohexene, cyclohexene,
pinene, myrcene, with conjugated double bonds could absorb ultraviolet. With the synotis erythopappa(Bur.et Franch)C. Jeffey et Y.L. Chen extract as a sunscreen ingredient, it was found
sunscreen with 2.5% mass fraction of synotis erythopappa (Bur.et Franch) C. Jeffey et YL.Chen had very good UV protection in UVB (290- 320nm) ultraviolet region, and the average absorbance value
was 1.95.
Key words: synotis erythopappa( Bur.et Franch )C. Jeffey ct Y .L. Chen: sunscreen: sunscreen cosmetics; extracts; ultraviolet rays
- 星期三, 19 6月 2024
西藏红缨合耳菊对B16细胞的影响(三)
3.1 前言
皮肤黑色素形成机理:存在于黑色素细胞组织中的酪氨酸在酪氨酸酶等酶的作用下经多巴、多巴醌、多巴色素、二羟基哚等中间体逐步转化为真黑色素,进而黑色素细胞组织将黑色素转移到表皮基底层细胞中,随着细胞的新陈代谢而被带到角质层中,最后随角质化细胞脱落。但是由于受紫外线、遗传、内分泌、炎症介质、饮食不当等因素的影响,黑色素代谢异常,皮肤黑素过快增长和分布不均,就会造成局部皮肤过黑及色素沉着,表现为黄褐斑、雀斑和炎症后色素沉着等。从国外文献来看,评价美白化妆品的功效主要以检测施加美白化妆品有效成分后,是否抑制酪氨酸酶活性为主要手段。目前,随着人们对祛斑美白药物需求的不断增加,越来越多的治疗色素沉着性疾病的药物投人到临床使用,其中不少药物确有良效,但使用中也出现了大量的不良反应导致严重的后果。
而将药物直接加入到细胞中观察药物对细胞的影响,则是一种最为直接的手段。由于黑素瘤细胞具有能够多次传代、生长快和培养条件相对较低等优点,成为筛选美白剂时的首选细胞。20世纪70年代初,Eisinger成功培养出正常黑色素瘤细胞,越来越多地采用人体正常黑色素细胞的体外培养技术。为此,我们基于实验室黑色素细胞培养,选用国内外常用B16黑素瘤细胞作为受试细胞,对红缨合耳菊的疗效和安全性的评价,为临床提供资料。
3.2材料与仪器
3.2.1 材料
红缨合耳菊提取物 自制
RPMI-1640培养基 美国 HyClone 公司
小牛血清 美国 HyClone 公司
胰蛋白酶 美国 HyClone 公司
L-多巴 美国 Sigma公司
Triton X-100 美国 Sigma公司
磷酸氢二钠 广州市化学试剂有限公司
磷酸二氢钾 广州市化学试剂有限公司
氯化钠 广州市化学试剂有限公司
氯化钾 广州市化学试剂有限公司
二甲基亚砜 广州市化学试剂有限公司
熊果苷 美国 Sigma公司
3.2.2 仪器
CJT-12超净工作台 北京昌平长城空气净化公司
DG-5031型酶联免疫检测仪 杭州博特仪器有限公司
CH2-TKC-3倒置显微镜 广东光学仪器有限公司
HZQ-F全温振荡培养 上海苏坤仪器有限公司
灭菌锅 上海苏坤仪器有限公司
3.3 实验方法
3.3.1细胞的培养及接种
无菌条件下,将B16细胞接种于含10%(体积分数)的小牛血清的RPMI1640培养基的培养瓶中,在5%(体积分数)COz培养箱中培养,每3d用0.25%胰酶消化传代一次。待细胞生长到对数期,用PBS洗涤,0.25%酶消化,细胞计数板计数。电镜观察细胞形态变化。调整细胞5X10个/mL。接种于96孔板中,每孔100L,置孵箱中孵育24h后,弃上清液,添加待测药物,每组药物最终质量浓度分别为320mg/L、160 mg/L、80 mg/L、40 mg/L、20 mg儿、10 mg/L、5 mg/L。每一浓度设5个孔,对照组不加药物,代之同量维持液,空白孔不接种细胞。37℃5%的CO,孵箱中孵育 72 h。
3.3.2 倒置显微镜观察
收集对数生长期细胞接种于6孔培养板中,每孔2ml。培养过夜后,加入不同浓度的药液100L,对照组加入同体积的RPMI-1640液。作用不同的时间后,置倒置显微镜下观察,照相并记录实验结果。
3.3.3黑色素细胞增殖抑制率测定
四甲基偶氮唑蓝比色法(MTT法):药物作用72h后,每孔加入5g/LMTT溶液10μL,4h后弃上清液,每孔加入 DMSO 100μL,振荡 10min 左右,在酶标仪上检测各孔吸光度值,以空白孔调零,波长为490nm。

3.4 实验结果与讨论
3.4.1 显微镜观察
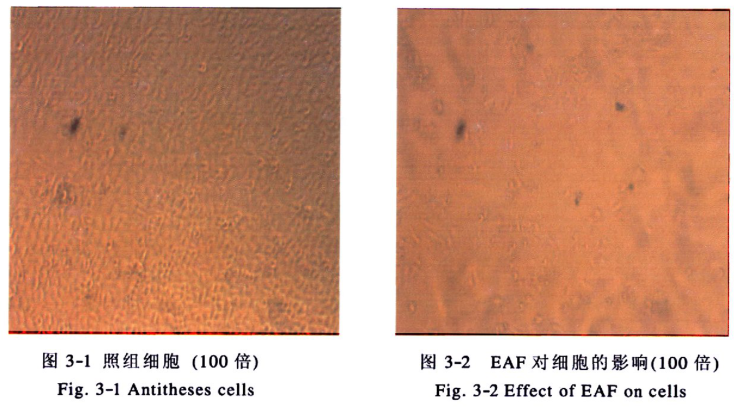
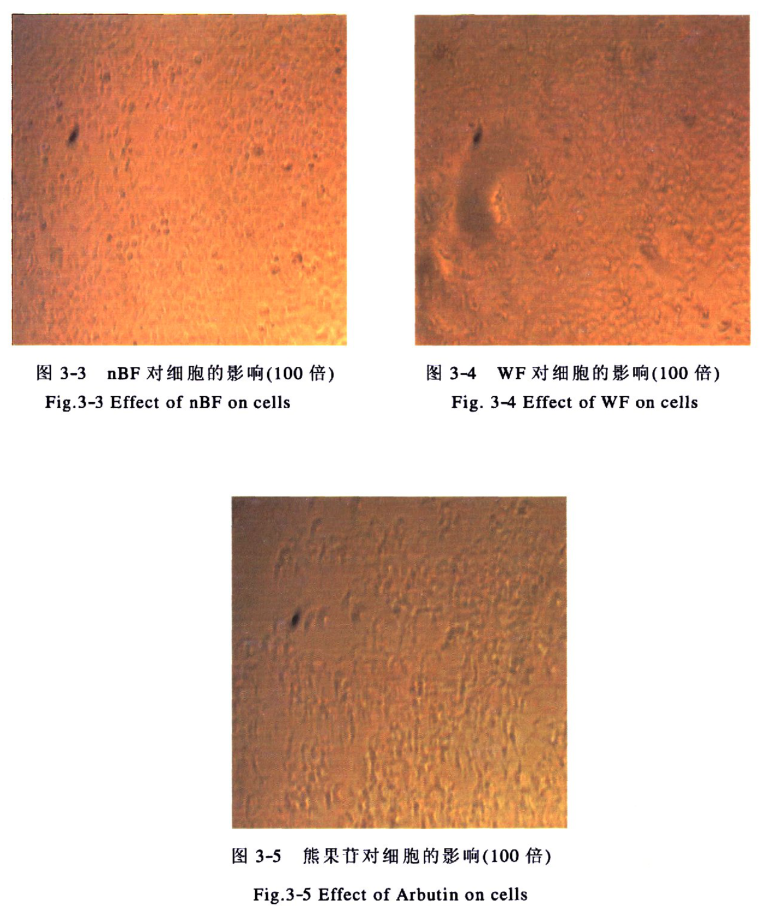
将红缨合耳菊各部分加入培养液(终浓度为320g/mL),作用于细胞后,我们发现细胞的形态明显发生变化。对照组细胞生长良好(见图3-1);加入EAF部分后,细胞树突减,细胞个数减少,变大(见图3-2);加入nBF部分后发现细胞未发生明显的变化,生长良好(见图3-3):加入WF部分后细胞生长状态稍差,不如对照组及nBF部分组(见图3-4):加入熊果苷组后能明显看到细胞树减少,细胞融合在一起(见图3-5)。
3.4.2 黑色素细胞增值率
红缨合耳菊可抑制黑色素细胞的生长,其效果与浓度相关,随着浓度的增加对细胞生长的抑制能力增加,320g/mL的熊果苷、EAF部分、nBF部分、WF部分对细胞生长的抑制率分别可达到42.57%、65.67%、10.24%、9.75%(表 3-1)。
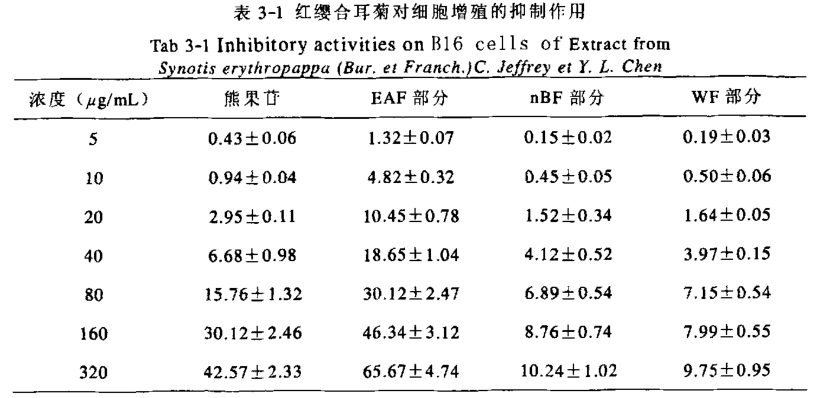
实验结果表明,受试物对黑色素细胞的毒性作用大小依次是:乙酸乙酯萃取部分>熊果苷>正丁醇萃取部分>水溶部分。熊果苷是常用的化妆品美白添加剂,其美白作用明显,人们对其美白作用的重视超过了对其细胞毒性的关注。然而许多研究均已表明熊果苷具有比较强的细胞毒性。我们的实验结果也对其进行了验证,当浓度为320μg/mL时,对细胞增殖的抑制作用可达到42.57%,可见其毒性较高。红缨合耳菊提取物的测试结果表明乙酸乙酯萃取部分对细胞的毒性比较大,而正丁醇萃取部分及水溶部分则对黑色素细胞的增殖抑制作用较小,浓度在320μg/mL时,其对细胞增殖的抑制率在10%左右,即这两部分有很小的细胞毒性。因此从健康方面考虑,在研究开发美白化妆品添加剂时,若使用熊果苷之类具有细胞毒性的物质,一定要在安全剂量范围内使用,而红缨合耳菊的正丁醇及水溶部分则可作为一种新型的天然植物提取物,基本没有剂量方面的限制。
3.5 本章小结
1.通过对细胞形态的观察,我们发现加入红缨合耳菊提取物及熊果苷后,细胞形态均发生变化,其中以EAF部分对细胞的影响最大。
2.测试了红缨合耳菊提取物对细胞生长的抑制率,研究发现,EAF部分对细胞的致死率最大,在320μg/mL时可达到65.67%,而nBF、WF部分分别为10.24、9.
未完待续……
- 星期二, 18 6月 2024
西藏红缨合耳菊对酪氨酸酶抑制作用(二)
2.1 前言
酪氨酸酶(EC1.14.18.1)又称多酚氧化酶,它广泛存在于动植物体和人体内,是生物体合成黑色素的关键酶。酪氨酸酶是一种含铜的金属酶,每一个亚基含两个金属铜离子,两个铜离子分别与蛋白质分子中组氨酸结合,另有一个内源桥基将两个铜离子联系在一起,构成酪氨酸酶催化氧化反应活性中心,能够催化单酚羟化成二酚(单酚酶活性),并把二酚氧化成(二酚酶活性),醌在非酶促条件下形成最终的反应产物黑色素。反应过程如下:
皮肤黑色素细胞组织将黑色素转移到表皮基底层细胞中,随着细胞的新陈代谢而被带到角质层中,最后随角化细胞脱落。若皮肤黑色素过速增长和分布不均时,就会造成局部皮肤过黑及色素沉着,出现皮肤黑色素。皮肤内黑色素是由黑色素细胞生成的,其过程是酪氨酸在酪氨酸酶的作用下生成多巴和多巴醌,多巴再经多巴色素、最终合成黑色素,然后被分泌到周围的角肮细胞中。其中黑色素的形成过程中,酪氨酸酶起了关键酶的作用,黑色素产生的多少与酪氨酸酶的活性有直接的关系。因此,皮肤美白剂就是通过作用于皮肤黑色素生成,代谢过程中,抑制黑色素生成且符合安全规范的物质。由于酪氨酸酶分别作用于酪氨酸转化为和加两个过程,目前的皮肤美白剂就是通过抑制酪氨酸酶活性或者阻断酪氨酸生成黑色素的氧化途径,从而减少黑色素的生成达到美白皮肤的效果,
传统的皮肤美白剂,往往采用化学性物质,如过氧化氢、化氨基汞以及各种酚类衍生化合物。这些化合物能使黑色素组织迅速瓦解,达到快速美白之功效。但因其对皮肤腐蚀性、细胞毒性和过敏性等因素,具有极大的危险性,在许多因家的卫生规范中,已被禁用。目前要求的皮肤美白剂,不但美白效果有效且无毒副作用,一般源自天然植物提取物,如熊果昔、曲酸及其衍生物、维生素及其衍生物、甘草黄酮、以及中草药提取物等。
西藏红缨合耳菊(Synotis erythropappa(Bur.et Franch.)C.Jeffrey et Y.L.Chen)为菊科(Composilae)植物,属西藏特有植物。产于西藏东南部,西藏当地女性将红缨合耳菊捣碎、烧成灰等后,敷在皮肤表面用于皮肤保养及紫外线防护。美白剂对酪氨酸酶活性的抑制率大小成为衡量这类物质美白效果的重要依据本文通过研究西藏红缨合耳菊70%乙醇提取物及其石油醚、乙酸乙酯、正丁醇萃取部分及水溶部分对酪氨酸酶的抑制作用,并以常用的美白药物熊果苷作为阳性对照,探讨其是否具有抑制酪氨酸酶的效果,为红缨合耳菊在美白化妆品方面的开发利用提供依据。
2.2 材料与仪器
2.2.1 材料
红缨合耳菊 自採
酪氨酸 美国 Sigma 公司
酪氨酸酶 美国 Sigma 公司
L-多巴 美国 Sigma 公司
磷酸氢二钠 广州市化学试剂有限公司
磷酸二氢钠 广州市化学试剂有限公司
二甲基亚砜 广州市化学试剂有限公司
无水乙醇 广州市化学试剂有限公司
石油醚 广州市化学试剂有限公司
正丁醇 广州市化学试剂有限公司
乙酸乙酯 广州市化学试剂有限公司
熊果苷 美国Sigma公司
2.2.2 仪器
FA2104型电子天平(0.0001g) 日本岛津
TU-1901双光束紫外可见分光光度计 北京普析通用
HWS型智能恒温恒湿箱 上海苏坤仪器有限公司
移液枪 上海大龙精密仪器有限公司
旋转蒸发仪 上海金叶仪器有限公司
PH 计 上海精密仪器
粉碎机 广州仪器有限公司
搅拌器 广州仪器有限公司
2.3 实验方法
2.3.1 提取分离方法
将红缨合耳菊在50℃下烘干后粉碎,用70%的乙醇浸提红缨合耳菊粉末(70%乙醇体积:红缨合耳菊质量=15:1),在机械搅拌器搅拌、室温下浸提一周。浸提后用旋转蒸发仪在50℃下将提取液浓缩至无乙醇后依次用石油醚、乙酸乙酯、正丁醇萃取。所得四部分溶液用旋转蒸发仪在50℃缩得到浸膏,浸在50℃下真空干燥。观察各萃取部分性状并计算各部分提取率。
2.3.2酪氨酸酶活性抑制的测定
参考Y.B.Ryu等及邓湘庆等的方法并略作修改,先加入0.1m含不同浓度的抑制剂于比色杯中,再加进2.8mL预先在30℃恒温水浴保温的底物溶液,然后加入0.1mL酪氨酸酶水溶液,即刻充分混匀,在30℃恒温条件下,测定波长为475nm的光密度值,由其随时间的增长直线的斜率计算出酶的活力,酶抑制实验平行做三次。测定单酚酶活力所用的底物为2mmol/LTyr,酶的终浓度为40μg/mL:二酚酶所用底物为0.5 mmol/L L-DOPA,酶的终浓度为 8 μg/mL。
2.3.3酪氨酸酶抑制类型的测定
参考酪氨酸酶活性抑制的测定,在测活体系中,固定酶的浓度,改变底物L-DOPA的浓度,测定不同浓度提取物对酶活力的影响,以Lineweaver-Burk 双倒数作图,比较酶催化反应的动力学参数,包括表观米氏常数(Km)和最大反应速度(Vm)的变化来判断抑制类型。
2.4 实验结果
2.4.1 红缨合耳菊的提取分离
中草药的有效成分的提取方法很多,常见的有溶剂萃取法、沉淀法、盐析法、透析法、结晶、重结晶和分步结晶法等方法。但最常见的,用得最广的,效果较好的还是溶剂萃取法,溶剂进入药材组织中,溶解其中的化学成分,并将其从组织中逐渐提出的过程。本实验对红缨合耳菊的处理采用溶剂萃取法。
提取时提取液的颜色随浸提时长变深最终为深红褐色,提取物经减压旋转蒸发后得到具有芳香味的粘稠状、深红褐色物质。将其水溶后分别用石油醚、乙酸乙酯、正丁醇进行萃取,初步分离后各萃取部分的提取率及性状见表2-1。
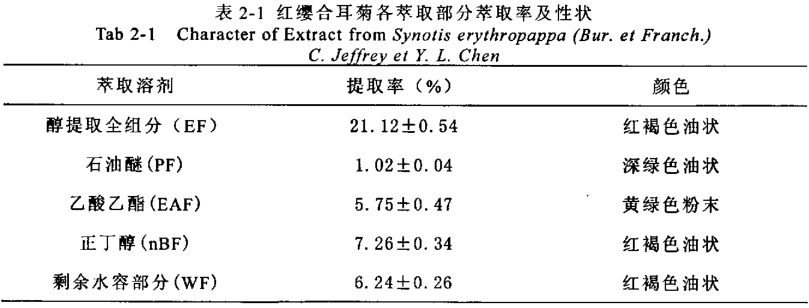
在实验过程中每次的浸提过程中得到的各萃取部分的性状基本一致,但是各部分萃取率稍微有些偏差。在使用旋转蒸发仪浓缩总提取物时一定要蒸到体积小于原加水的体积量为宜,若还有残留的乙醇则在萃取时可能使萃取产生偏差。在浓缩及真空干燥时温度不易超过60℃,温度过高可能会导致一些有效成分发生变化。
2.4.2对酪氨酸酶单酚酶活力的影响
以L-Tyr为底物,测试各部分对酪氨酸酶单酚酶活力的影响,结果见表2-2。
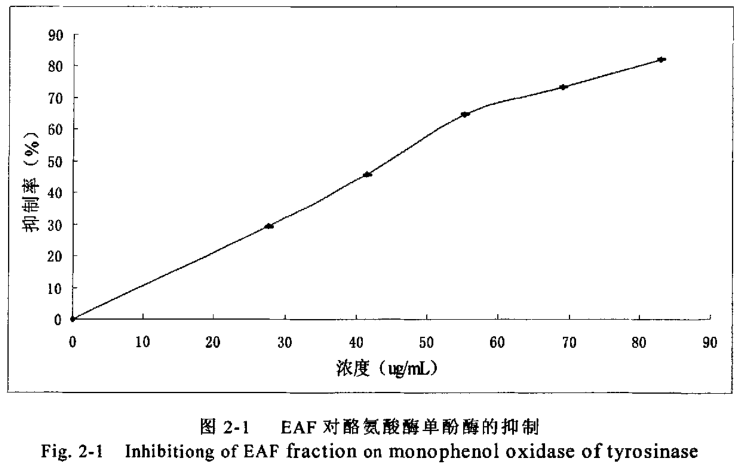
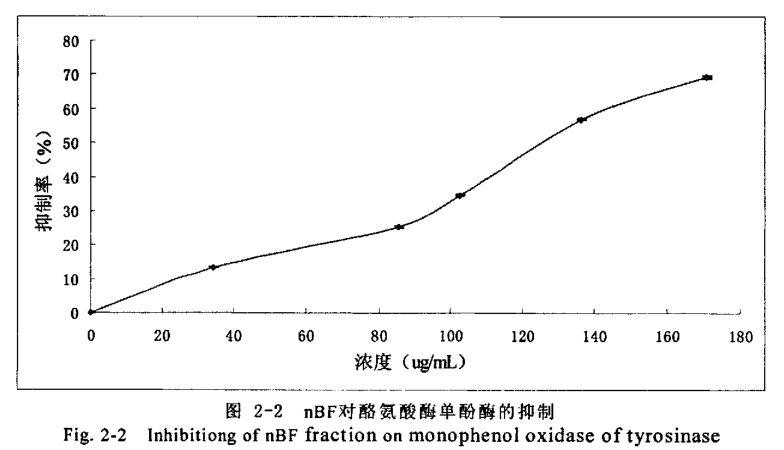
实验中醇提取物及其石油醚、水溶部分ICso均超过150g/mL,而乙酸乙酯正丁醇部分ICso均小于150μg/mL,提示了EAF、nBF部分富集了西藏红缨合耳菊抑制酪氨酸酶单酚酶的主要有效组分。我们进一步分别EAF、nBF部分对酪氨酸酶的抑制作用进行了研究,研究结果(见图2-1、2-2)表明抑制率随提取物的浓度的增加而变大,EAF、nBF部分的IC50分别为57.8、140g/mL。
2.4.3对酪氨酸酶单酚酶活性的迟滞影响
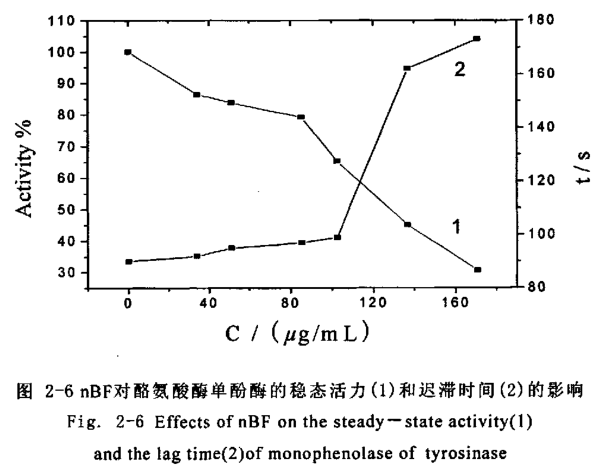
酪氨酸酶单酚酶的催化特征有迟滞过程,催化酪氨酸羟基化过程见图2-3、图2-4,随着抑制剂浓度的增大酪氨酸酶的稳态活力(直线部分的斜率)逐渐下降并伴随着迟滞时间的延长。
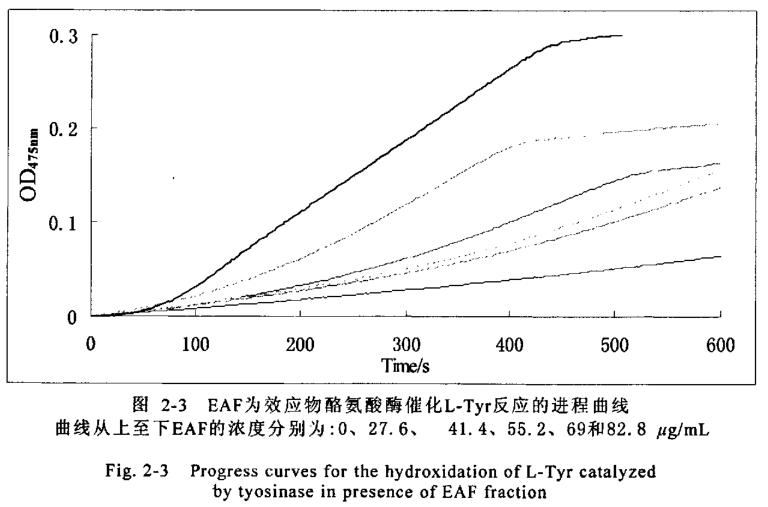
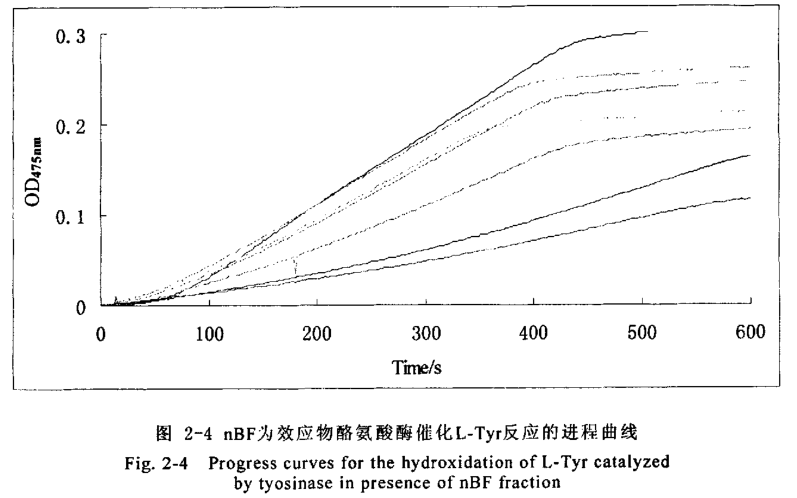
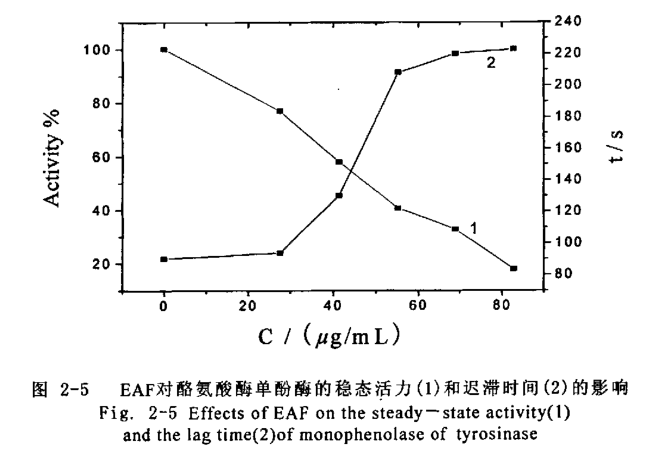
曲线从上至下nBF的浓度分别为:0、34.1、51.2、85.4、102.5、136.6和170.8 g/mL82.8μg/mLEAF部分使得酶的稳态活力下降了
82.1%(图2-5线1)、使迟滞时间从78S延长到223S(图2-5线2);170.8g/mL的nBF部分使得酶的稳态活力下降了69.4%(图2-6线1)、使迟滞时间从78S延长到173S(图2-6线2)。
2.4.4 对酪氨酸酶双酚酶活力的影响
以L-DOPA为底物,测试各部分对酪氨酸酶双酚酶活力的影响,结果见表2-3。
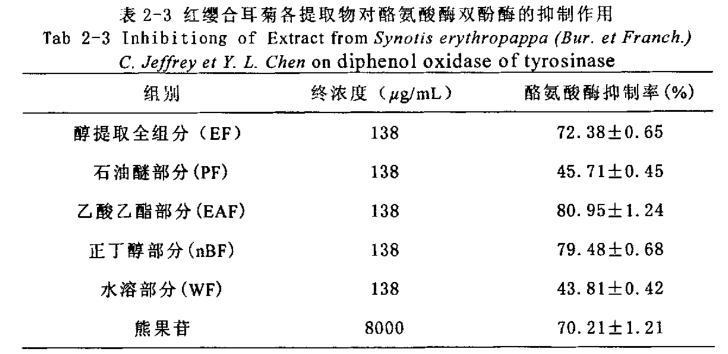
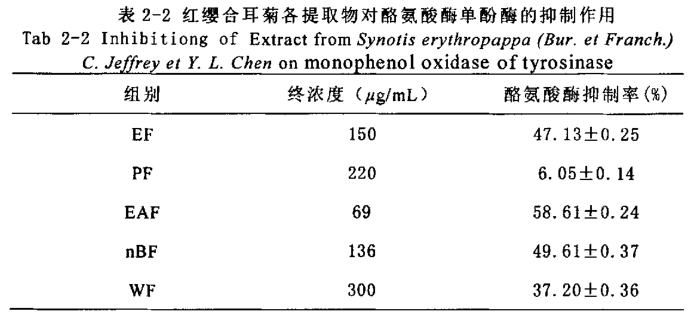
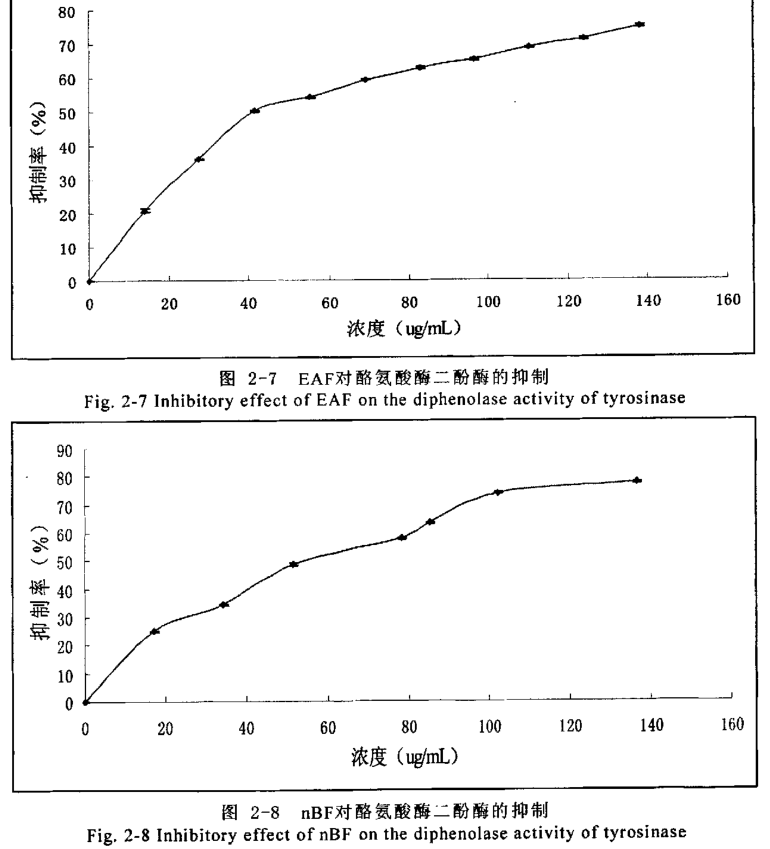
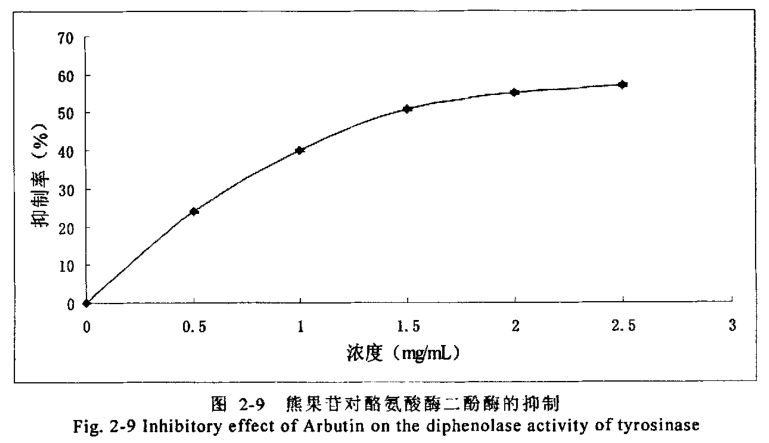
实验中1384g/m醇提取物、乙酸乙酯、正丁醇部分对酪氨酸酶抑制率分别为72.38%、80.95%、79.48%均超过8.0mg/mL 熊果苷的 70.21%,而石油醚及水溶部分对酶的抑制活性较弱,说明西藏红缨合耳菊抑制酪氨酸酶双酚酶的主要有效组分集中在EAF、BF部分。进一步研究EAF、nBF部分对酪氨酸酶双酶活力抑制能力发现抑制率随着提取物浓度的增大而增大,ICS0分别为41.2、59.6μg/mL(见图7、图8)。比熊果苷抑制双酚酶活性的IC5o值 1.44 mg/mL低得多(见图2-9)。
2.4.5对酪氨酸酶抑制类型
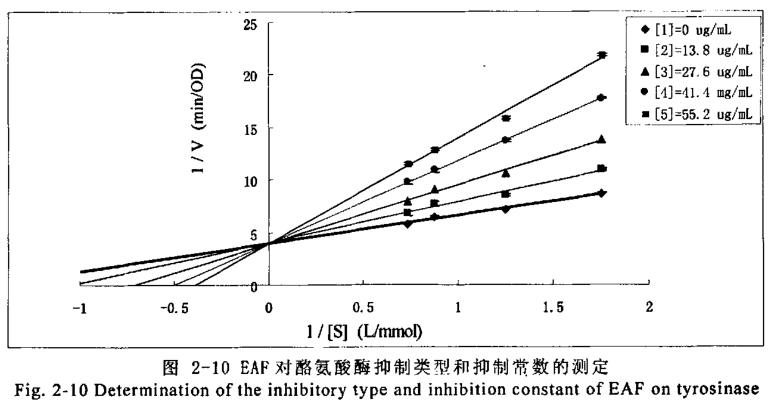
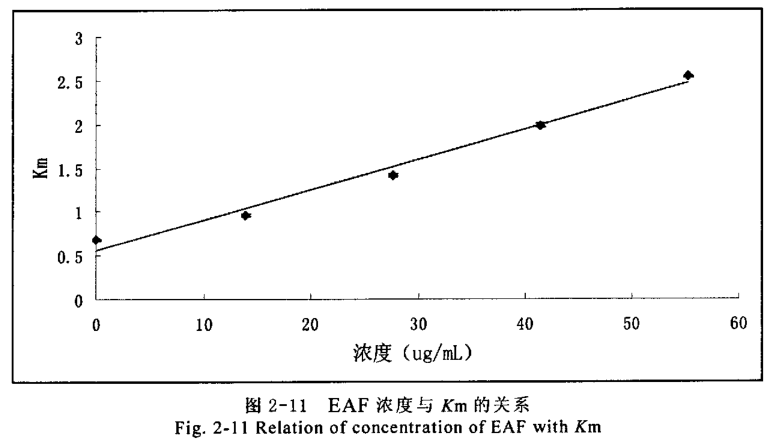
进一步研究EAF、nBF部分对酪氨酸酶二酚酶抑制作用类型,在测活体系中,固定酶的浓度,改变底物L-DOPA的浓度,测定不同浓度效应物对酶活力的影响,以 Lineweaver-Burk双倒数作图判断抑制类型。乙酸乙酯部分双倒数图(见图 2-10)得到一组纵轴截距不变的直线,表明其抑制类型为竞争性类型。以不同浓度乙酸乙酯部分测定的Km对抑制剂浓度作图可得一条直线(见图2-11),从直线的斜率求得抑制常数(K;)为19.7 g/mL。
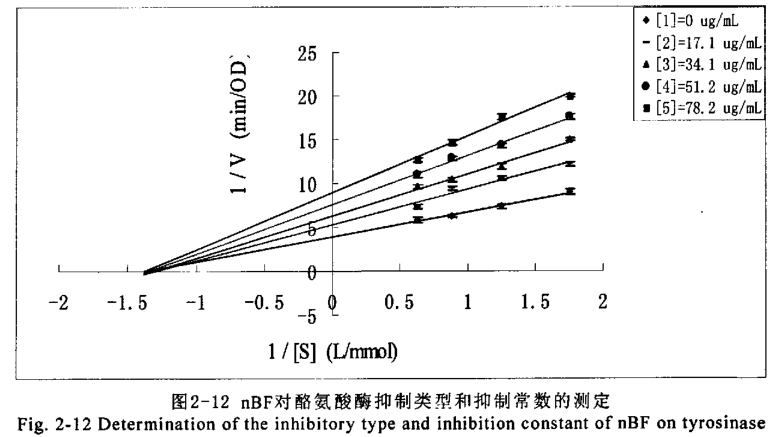
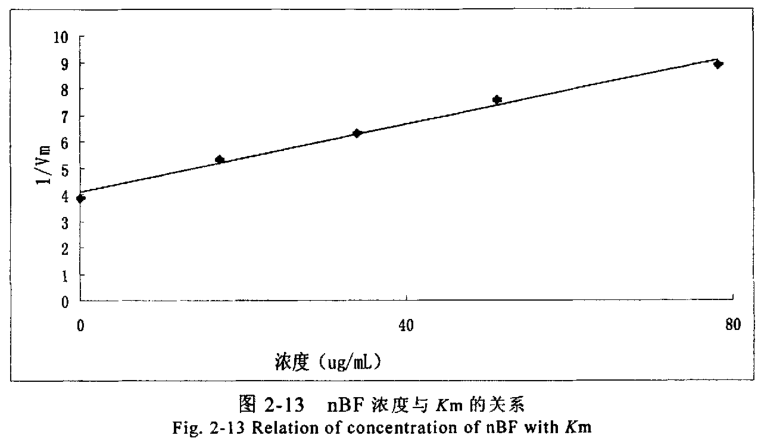
正丁醇部分双倒数图(见图2-12)得到一组横轴截距不变的直线,表明其抑制类型为非竞争性类型。以不同浓度正丁醇部分测定的1/Vmax对抑制剂度作图可得一条直线(图2-13),从直线的斜率求得抑制常数(K)为60.7g/mL 。
2.5 讨论
酪氨酸酶为黑素生物合成的限速酶,控制其活力可控制黑素生成量。酪氨酸酶在黑色素的生物合成过程中起着关键作用,该酶活性过高会导致色斑及黑色素瘤的形成,酪氨酸酶是合成黑色素的关键酶。因此,在美自化妆品中添加能抑制酪氨酸酶活性的美白剂,可以通过抑制酪氨酸酶活性直接抑制黑色素的生成,从而达到美白肌肤的目的。早期研究发现,熊果苷对酪氨酸酶活性有明显抑制作用本研究结果表明熊果苷浓度在一定范围内,酪氨酶活性随其浓度增加而降低,表现出较强的对酪氨酸酶的抑制作用,与前人研究结果一致。因此本实验选择熊果苷作为阳性对照物,观察红缨合耳菊提取物对酪氨酸酶的抑制作用,为寻找新的美白功效的化妆品原料提供实验依据。从上面两种抑制剂相比较来看,红缨合耳菊提取物对酪氨酸酶的抑制效果远优于熊果苷。并且可以看出红缨合耳菊提取物对酪氨酸酶的抑制效果非常明显。红缨合耳菊的EAF、nBF部分对酪氨酸酶的单酚酶的抑制效果明显优于熊果苷,这两部分的半数抑制率IC5分别可达到57.8、140μg/mL;且延迟时间较长,82.8g/mLEAF部分使得酶的稳态活力下降了82.1%、使迟滞时间从78S延长到223S:170.8g/mL的nBF部分使得酶的稳态活力下降了69.4%、使迟滞时间从78S延长到173S。在这个过程中不仅可以有效的抑制酪氨酸酶单酚酶的活性,并且能延迟黑色素的最初反应进程。对酪氨酸酶双酚酶也有明显的抑制作用,随提取物浓度的增加,酪氨酸酶的活性逐渐降低,EAF、nBF部分的IC50分别为41.2、59.6g/mL其效果远优于熊果苷(IC50值为1.44mg/mL),与熊果苷比较,EAF、nBF部分起到了与熊果苷相似的抑制作用,且相关关系分析说明EAF、nBF部分浓度与其对酪氨酸酶活性抑制率之间存在正相关关系。抑制剂对酶的抑制作用主要表现为两个类型不可逆抑制和可逆抑制。从红缨合耳菊提物对酪氨酸酶的抑制作用的实验结果可以表明,红缨合耳菊提取物对酪氨酸酶的抑制作用明显的表现为可逆抑制。而可逆抑制又分为竞争性抑制,非竞争性抑制,反竞争抑制及混合性抑制等类型。因此本实验在验证了红缨合耳菊提物对酪氨酸酶的抑制作用表现为可逆抑制后,进一步作了抑制作用的动力学分析。从动力学实验分析中可以初步得出结论,EAF部分对酪氨酸酶的抑制效果主要表现为竞争性抑制,抑制常数(K)为19.7g/mL;而nBF部分对酪氨酸酶的抑制作用主要表现为非竞争性抑制抑制常数(K;)为60.7g/mL。由于红缨合耳菊提取物是粗提产品,成分复杂,也不排除有其它抑制类型的可能性,因此该结论只能是初步的,只有将有效成分提纯后才能进-步测出其有效成分对酪氨酸酶的抑制类型。与常用的化妆品添加剂熊果苷相比较我们会发现其体外酪氨酸酶抑制效果非常理想,美自效果几乎是熊果苷的40倍,而且这是天然植物的提取物,属于纯天然的美白化妆品添加剂。红缨合耳菊提取物对酪氨酸酶的抑制作用为预防和治疗各种色素病及黑色素瘤开辟了一条新途径,在化妆品行业和临床医学应用方面具有开发价值,为进一步对有效成分的提纯、开发和利用打下基础。
2.6本章小结
1.用石油醚、乙酸乙酯、正丁醇将红缨合耳菊提取物依次进行萃取,初步对其进行分离提取,得到四个不同极性段的物质。
2.测定了红缨合耳菊提取物对酪氨酸酶单酚酶的影响,研究发现乙酸乙酯及正丁醇萃取部分对单酚酶有强的抑制作用,半数抑制率IC5分别为57.8、140ug/mL。
3.测定了乙酸乙酯及正丁醇萃取部分对单酚酶的延迟作用,82.8g/mLEAF部分使得酶的稳态活力下降了.82.1%、使迟滞时间从78S延长到223S;170.8Hg/mL的BF部分使得酶的稳态活力下降了69.4%、使迟滞时间从78S延长到173 S
4.测定了测定了红缨合耳菊提取物对酪氨酸酶双酚酶的影响,研究发现乙酸乙酯及正丁醇萃取部分对单酚酶有强的抑制作用,半数抑制率ICs0分别为41.259.6 g/mL.
5.研究了乙酸乙酯及正丁醇萃取部分对双酚酶的抑制作用类型,发现EAF部分对二酚酶的抑制作用表现为可逆竞争性抑制类型,抑制常数为19.7g/mL;nBF部分对二酚酶抑制作用表现为可逆非竞争性抑制类型,抑制常数为60.7ug/mL。
未完待续……

{kind=link}
{kind=link}
{kind=link}
{kind=link}