文献精选

原创: 国际糖尿病 idiabetes
糖尿病会导致伤口愈合变慢,使糖尿病患者发生感染和其他并发症的风险增加。控制好糖尿病可改善伤口愈合,减少发生严重感染的概率。

原创: Wound Academy 慢伤前沿
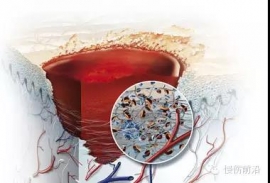
生物膜的构成
生物膜是一种复杂的微生物群落,含有相互及与表面黏附的微生物,被细胞外聚合物质包裹【1, 2】。这些细胞外聚合物质主要是合成的多聚糖保护基质,由微生物分泌,将生物膜牢牢地粘附在活体或非活体表面。

原创: 小米星 护士网
压疮是长期卧床的年老体弱、昏迷瘫痪和危重患者常见的并发症之一,常好发于长期卧床不能自理、昏迷、营养不良等患者,压疮一旦形成,将大大增加患者的治疗和照顾负担。Ⅱ期压疮表现为局部红肿向外扩张,炎性浸润,皮肤变为紫红色,表皮脱落,常带有水疱出现,疼痛剧烈。
