
伤口世界
- 星期二, 18 6月 2024
西藏红缨合耳菊对酪氨酸酶抑制作用(二)
2.1 前言
酪氨酸酶(EC1.14.18.1)又称多酚氧化酶,它广泛存在于动植物体和人体内,是生物体合成黑色素的关键酶。酪氨酸酶是一种含铜的金属酶,每一个亚基含两个金属铜离子,两个铜离子分别与蛋白质分子中组氨酸结合,另有一个内源桥基将两个铜离子联系在一起,构成酪氨酸酶催化氧化反应活性中心,能够催化单酚羟化成二酚(单酚酶活性),并把二酚氧化成(二酚酶活性),醌在非酶促条件下形成最终的反应产物黑色素。反应过程如下:
皮肤黑色素细胞组织将黑色素转移到表皮基底层细胞中,随着细胞的新陈代谢而被带到角质层中,最后随角化细胞脱落。若皮肤黑色素过速增长和分布不均时,就会造成局部皮肤过黑及色素沉着,出现皮肤黑色素。皮肤内黑色素是由黑色素细胞生成的,其过程是酪氨酸在酪氨酸酶的作用下生成多巴和多巴醌,多巴再经多巴色素、最终合成黑色素,然后被分泌到周围的角肮细胞中。其中黑色素的形成过程中,酪氨酸酶起了关键酶的作用,黑色素产生的多少与酪氨酸酶的活性有直接的关系。因此,皮肤美白剂就是通过作用于皮肤黑色素生成,代谢过程中,抑制黑色素生成且符合安全规范的物质。由于酪氨酸酶分别作用于酪氨酸转化为和加两个过程,目前的皮肤美白剂就是通过抑制酪氨酸酶活性或者阻断酪氨酸生成黑色素的氧化途径,从而减少黑色素的生成达到美白皮肤的效果,
传统的皮肤美白剂,往往采用化学性物质,如过氧化氢、化氨基汞以及各种酚类衍生化合物。这些化合物能使黑色素组织迅速瓦解,达到快速美白之功效。但因其对皮肤腐蚀性、细胞毒性和过敏性等因素,具有极大的危险性,在许多因家的卫生规范中,已被禁用。目前要求的皮肤美白剂,不但美白效果有效且无毒副作用,一般源自天然植物提取物,如熊果昔、曲酸及其衍生物、维生素及其衍生物、甘草黄酮、以及中草药提取物等。
西藏红缨合耳菊(Synotis erythropappa(Bur.et Franch.)C.Jeffrey et Y.L.Chen)为菊科(Composilae)植物,属西藏特有植物。产于西藏东南部,西藏当地女性将红缨合耳菊捣碎、烧成灰等后,敷在皮肤表面用于皮肤保养及紫外线防护。美白剂对酪氨酸酶活性的抑制率大小成为衡量这类物质美白效果的重要依据本文通过研究西藏红缨合耳菊70%乙醇提取物及其石油醚、乙酸乙酯、正丁醇萃取部分及水溶部分对酪氨酸酶的抑制作用,并以常用的美白药物熊果苷作为阳性对照,探讨其是否具有抑制酪氨酸酶的效果,为红缨合耳菊在美白化妆品方面的开发利用提供依据。
2.2 材料与仪器
2.2.1 材料
红缨合耳菊 自採
酪氨酸 美国 Sigma 公司
酪氨酸酶 美国 Sigma 公司
L-多巴 美国 Sigma 公司
磷酸氢二钠 广州市化学试剂有限公司
磷酸二氢钠 广州市化学试剂有限公司
二甲基亚砜 广州市化学试剂有限公司
无水乙醇 广州市化学试剂有限公司
石油醚 广州市化学试剂有限公司
正丁醇 广州市化学试剂有限公司
乙酸乙酯 广州市化学试剂有限公司
熊果苷 美国Sigma公司
2.2.2 仪器
FA2104型电子天平(0.0001g) 日本岛津
TU-1901双光束紫外可见分光光度计 北京普析通用
HWS型智能恒温恒湿箱 上海苏坤仪器有限公司
移液枪 上海大龙精密仪器有限公司
旋转蒸发仪 上海金叶仪器有限公司
PH 计 上海精密仪器
粉碎机 广州仪器有限公司
搅拌器 广州仪器有限公司
2.3 实验方法
2.3.1 提取分离方法
将红缨合耳菊在50℃下烘干后粉碎,用70%的乙醇浸提红缨合耳菊粉末(70%乙醇体积:红缨合耳菊质量=15:1),在机械搅拌器搅拌、室温下浸提一周。浸提后用旋转蒸发仪在50℃下将提取液浓缩至无乙醇后依次用石油醚、乙酸乙酯、正丁醇萃取。所得四部分溶液用旋转蒸发仪在50℃缩得到浸膏,浸在50℃下真空干燥。观察各萃取部分性状并计算各部分提取率。
2.3.2酪氨酸酶活性抑制的测定
参考Y.B.Ryu等及邓湘庆等的方法并略作修改,先加入0.1m含不同浓度的抑制剂于比色杯中,再加进2.8mL预先在30℃恒温水浴保温的底物溶液,然后加入0.1mL酪氨酸酶水溶液,即刻充分混匀,在30℃恒温条件下,测定波长为475nm的光密度值,由其随时间的增长直线的斜率计算出酶的活力,酶抑制实验平行做三次。测定单酚酶活力所用的底物为2mmol/LTyr,酶的终浓度为40μg/mL:二酚酶所用底物为0.5 mmol/L L-DOPA,酶的终浓度为 8 μg/mL。
2.3.3酪氨酸酶抑制类型的测定
参考酪氨酸酶活性抑制的测定,在测活体系中,固定酶的浓度,改变底物L-DOPA的浓度,测定不同浓度提取物对酶活力的影响,以Lineweaver-Burk 双倒数作图,比较酶催化反应的动力学参数,包括表观米氏常数(Km)和最大反应速度(Vm)的变化来判断抑制类型。
2.4 实验结果
2.4.1 红缨合耳菊的提取分离
中草药的有效成分的提取方法很多,常见的有溶剂萃取法、沉淀法、盐析法、透析法、结晶、重结晶和分步结晶法等方法。但最常见的,用得最广的,效果较好的还是溶剂萃取法,溶剂进入药材组织中,溶解其中的化学成分,并将其从组织中逐渐提出的过程。本实验对红缨合耳菊的处理采用溶剂萃取法。
提取时提取液的颜色随浸提时长变深最终为深红褐色,提取物经减压旋转蒸发后得到具有芳香味的粘稠状、深红褐色物质。将其水溶后分别用石油醚、乙酸乙酯、正丁醇进行萃取,初步分离后各萃取部分的提取率及性状见表2-1。
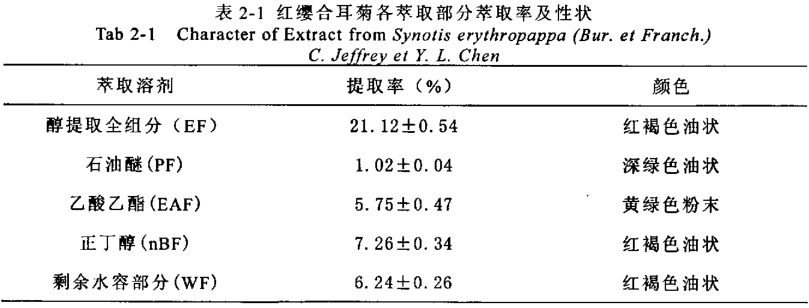
在实验过程中每次的浸提过程中得到的各萃取部分的性状基本一致,但是各部分萃取率稍微有些偏差。在使用旋转蒸发仪浓缩总提取物时一定要蒸到体积小于原加水的体积量为宜,若还有残留的乙醇则在萃取时可能使萃取产生偏差。在浓缩及真空干燥时温度不易超过60℃,温度过高可能会导致一些有效成分发生变化。
2.4.2对酪氨酸酶单酚酶活力的影响
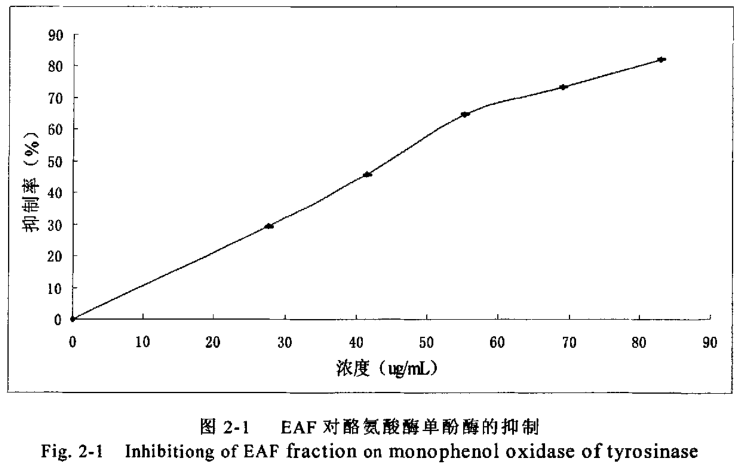
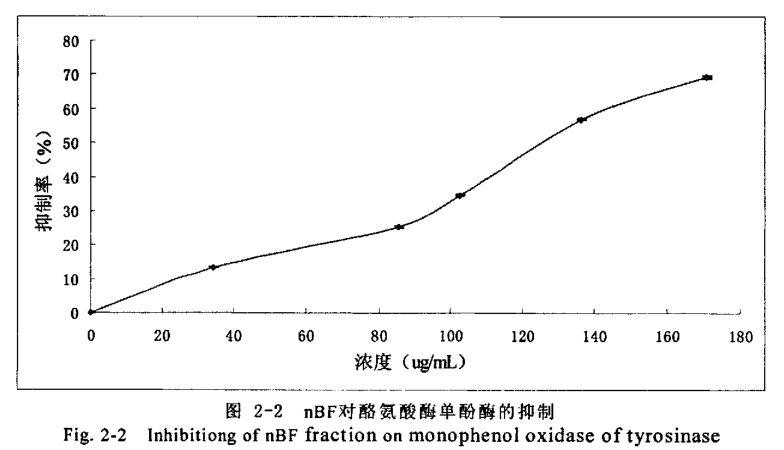
以L-Tyr为底物,测试各部分对酪氨酸酶单酚酶活力的影响,结果见表2-2。
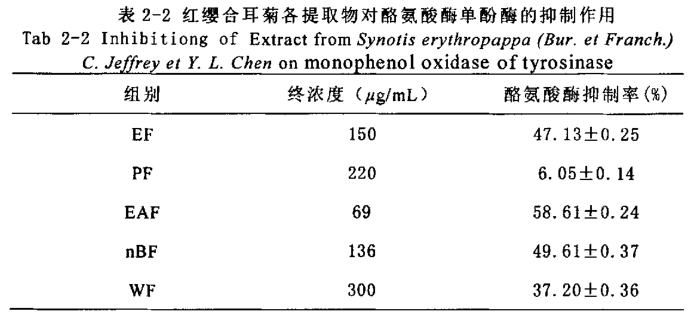
实验中醇提取物及其石油醚、水溶部分ICso均超过150g/mL,而乙酸乙酯正丁醇部分ICso均小于150μg/mL,提示了EAF、nBF部分富集了西藏红缨合耳菊抑制酪氨酸酶单酚酶的主要有效组分。我们进一步分别EAF、nBF部分对酪氨酸酶的抑制作用进行了研究,研究结果(见图2-1、2-2)表明抑制率随提取物的浓度的增加而变大,EAF、nBF部分的IC50分别为57.8、140g/mL。
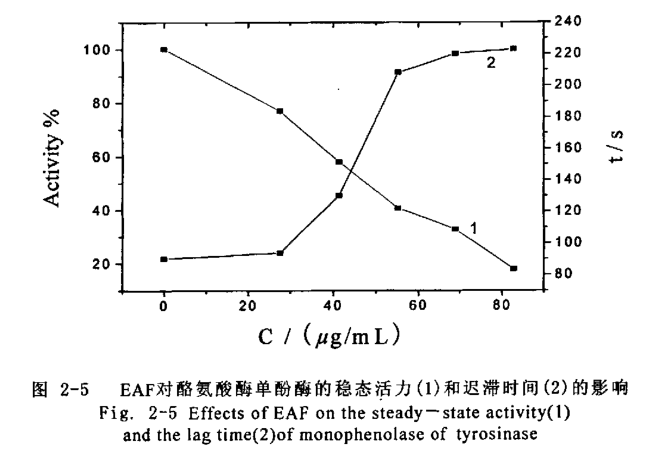
2.4.3对酪氨酸酶单酚酶活性的迟滞影响
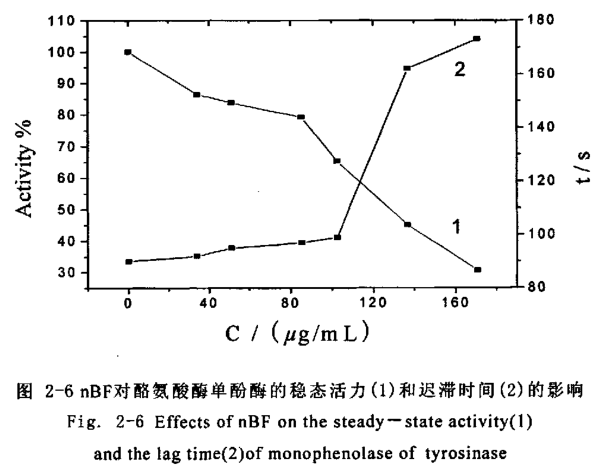
酪氨酸酶单酚酶的催化特征有迟滞过程,催化酪氨酸羟基化过程见图2-3、图2-4,随着抑制剂浓度的增大酪氨酸酶的稳态活力(直线部分的斜率)逐渐下降并伴随着迟滞时间的延长。
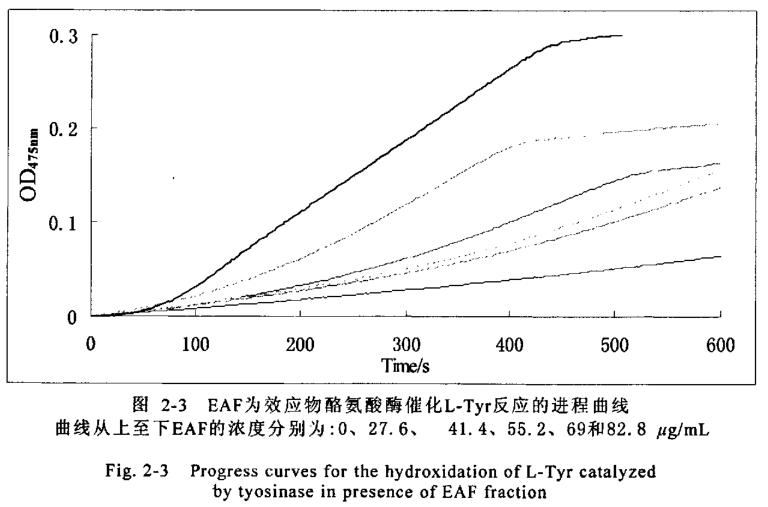
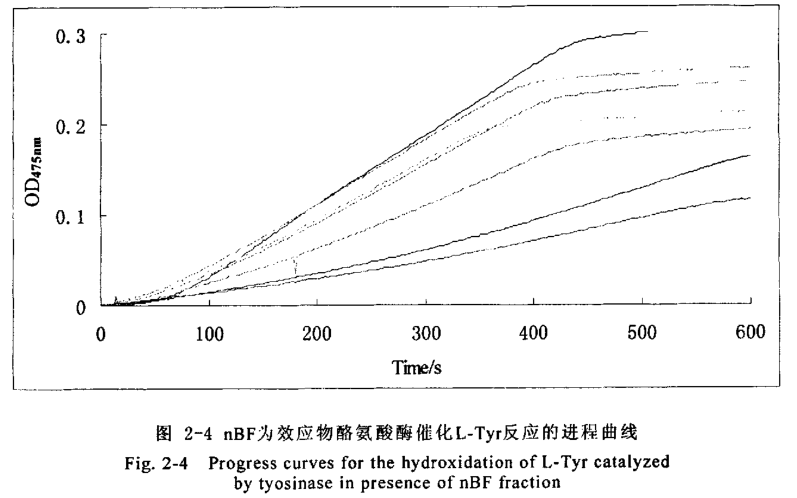
曲线从上至下nBF的浓度分别为:0、34.1、51.2、85.4、102.5、136.6和170.8 g/mL82.8μg/mLEAF部分使得酶的稳态活力下降了
82.1%(图2-5线1)、使迟滞时间从78S延长到223S(图2-5线2);170.8g/mL的nBF部分使得酶的稳态活力下降了69.4%(图2-6线1)、使迟滞时间从78S延长到173S(图2-6线2)。
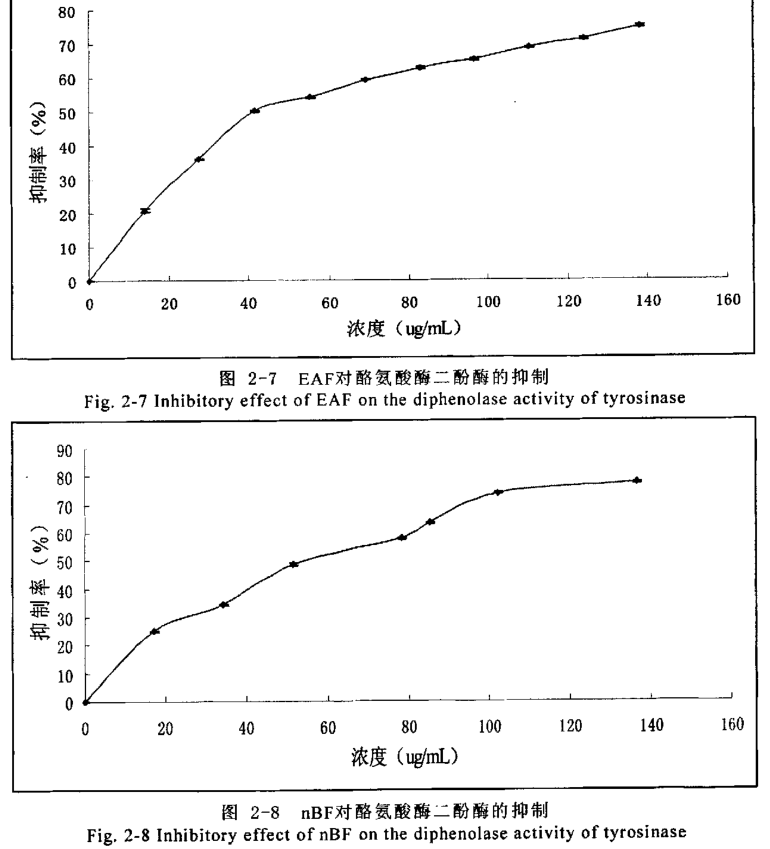
2.4.4 对酪氨酸酶双酚酶活力的影响
以L-DOPA为底物,测试各部分对酪氨酸酶双酚酶活力的影响,结果见表2-3。
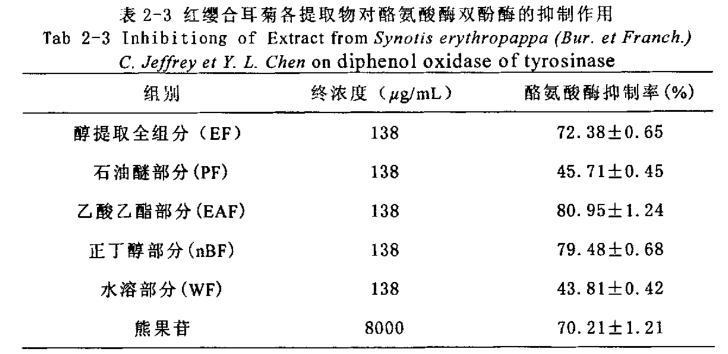
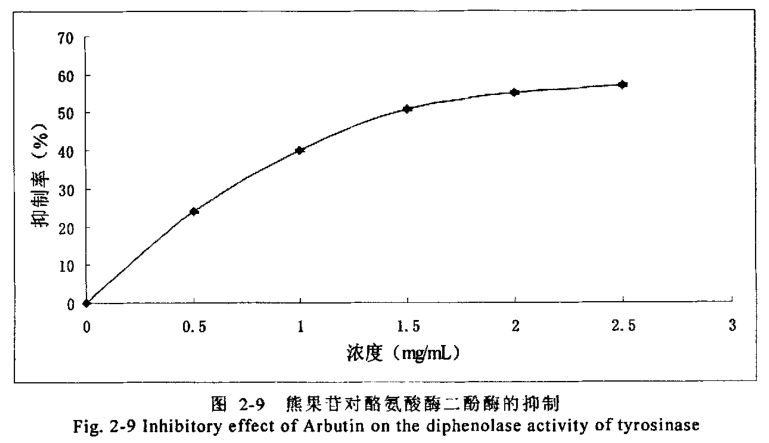
实验中1384g/m醇提取物、乙酸乙酯、正丁醇部分对酪氨酸酶抑制率分别为72.38%、80.95%、79.48%均超过8.0mg/mL 熊果苷的 70.21%,而石油醚及水溶部分对酶的抑制活性较弱,说明西藏红缨合耳菊抑制酪氨酸酶双酚酶的主要有效组分集中在EAF、BF部分。进一步研究EAF、nBF部分对酪氨酸酶双酶活力抑制能力发现抑制率随着提取物浓度的增大而增大,ICS0分别为41.2、59.6μg/mL(见图7、图8)。比熊果苷抑制双酚酶活性的IC5o值 1.44 mg/mL低得多(见图2-9)。
2.4.5对酪氨酸酶抑制类型
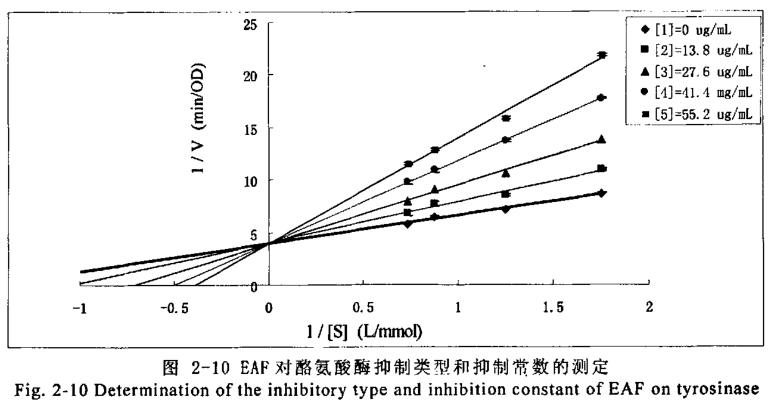
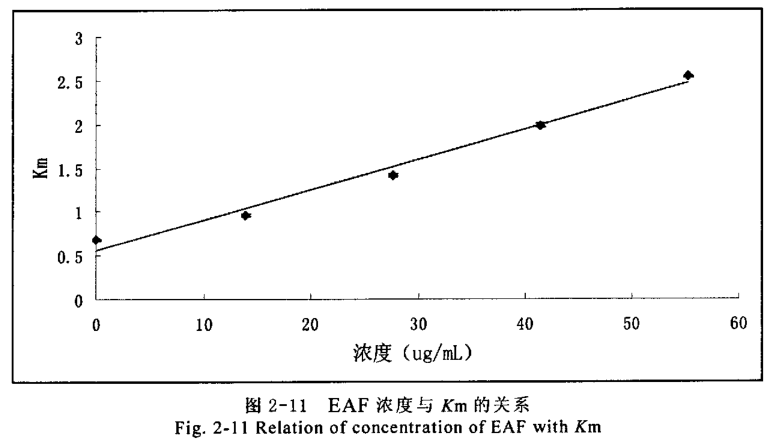
进一步研究EAF、nBF部分对酪氨酸酶二酚酶抑制作用类型,在测活体系中,固定酶的浓度,改变底物L-DOPA的浓度,测定不同浓度效应物对酶活力的影响,以 Lineweaver-Burk双倒数作图判断抑制类型。乙酸乙酯部分双倒数图(见图 2-10)得到一组纵轴截距不变的直线,表明其抑制类型为竞争性类型。以不同浓度乙酸乙酯部分测定的Km对抑制剂浓度作图可得一条直线(见图2-11),从直线的斜率求得抑制常数(K;)为19.7 g/mL。
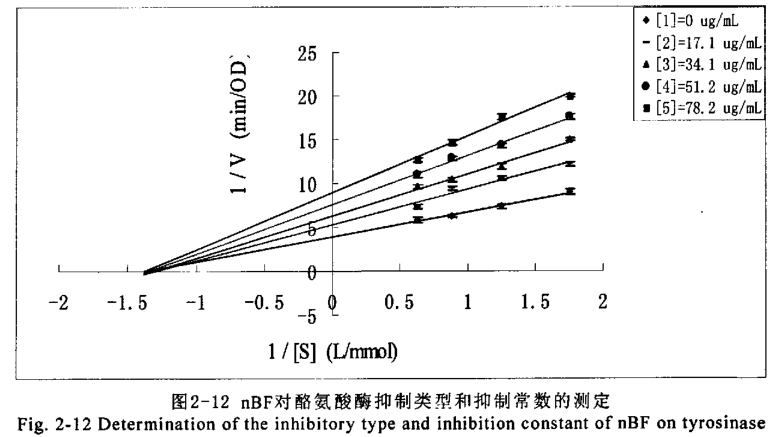
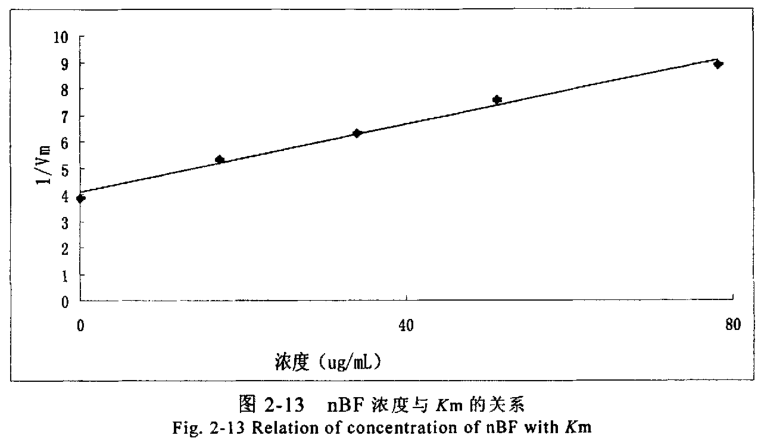
正丁醇部分双倒数图(见图2-12)得到一组横轴截距不变的直线,表明其抑制类型为非竞争性类型。以不同浓度正丁醇部分测定的1/Vmax对抑制剂度作图可得一条直线(图2-13),从直线的斜率求得抑制常数(K)为60.7g/mL 。
2.5 讨论
酪氨酸酶为黑素生物合成的限速酶,控制其活力可控制黑素生成量。酪氨酸酶在黑色素的生物合成过程中起着关键作用,该酶活性过高会导致色斑及黑色素瘤的形成,酪氨酸酶是合成黑色素的关键酶。因此,在美自化妆品中添加能抑制酪氨酸酶活性的美白剂,可以通过抑制酪氨酸酶活性直接抑制黑色素的生成,从而达到美白肌肤的目的。早期研究发现,熊果苷对酪氨酸酶活性有明显抑制作用本研究结果表明熊果苷浓度在一定范围内,酪氨酶活性随其浓度增加而降低,表现出较强的对酪氨酸酶的抑制作用,与前人研究结果一致。因此本实验选择熊果苷作为阳性对照物,观察红缨合耳菊提取物对酪氨酸酶的抑制作用,为寻找新的美白功效的化妆品原料提供实验依据。从上面两种抑制剂相比较来看,红缨合耳菊提取物对酪氨酸酶的抑制效果远优于熊果苷。并且可以看出红缨合耳菊提取物对酪氨酸酶的抑制效果非常明显。红缨合耳菊的EAF、nBF部分对酪氨酸酶的单酚酶的抑制效果明显优于熊果苷,这两部分的半数抑制率IC5分别可达到57.8、140μg/mL;且延迟时间较长,82.8g/mLEAF部分使得酶的稳态活力下降了82.1%、使迟滞时间从78S延长到223S:170.8g/mL的nBF部分使得酶的稳态活力下降了69.4%、使迟滞时间从78S延长到173S。在这个过程中不仅可以有效的抑制酪氨酸酶单酚酶的活性,并且能延迟黑色素的最初反应进程。对酪氨酸酶双酚酶也有明显的抑制作用,随提取物浓度的增加,酪氨酸酶的活性逐渐降低,EAF、nBF部分的IC50分别为41.2、59.6g/mL其效果远优于熊果苷(IC50值为1.44mg/mL),与熊果苷比较,EAF、nBF部分起到了与熊果苷相似的抑制作用,且相关关系分析说明EAF、nBF部分浓度与其对酪氨酸酶活性抑制率之间存在正相关关系。抑制剂对酶的抑制作用主要表现为两个类型不可逆抑制和可逆抑制。从红缨合耳菊提物对酪氨酸酶的抑制作用的实验结果可以表明,红缨合耳菊提取物对酪氨酸酶的抑制作用明显的表现为可逆抑制。而可逆抑制又分为竞争性抑制,非竞争性抑制,反竞争抑制及混合性抑制等类型。因此本实验在验证了红缨合耳菊提物对酪氨酸酶的抑制作用表现为可逆抑制后,进一步作了抑制作用的动力学分析。从动力学实验分析中可以初步得出结论,EAF部分对酪氨酸酶的抑制效果主要表现为竞争性抑制,抑制常数(K)为19.7g/mL;而nBF部分对酪氨酸酶的抑制作用主要表现为非竞争性抑制抑制常数(K;)为60.7g/mL。由于红缨合耳菊提取物是粗提产品,成分复杂,也不排除有其它抑制类型的可能性,因此该结论只能是初步的,只有将有效成分提纯后才能进-步测出其有效成分对酪氨酸酶的抑制类型。与常用的化妆品添加剂熊果苷相比较我们会发现其体外酪氨酸酶抑制效果非常理想,美自效果几乎是熊果苷的40倍,而且这是天然植物的提取物,属于纯天然的美白化妆品添加剂。红缨合耳菊提取物对酪氨酸酶的抑制作用为预防和治疗各种色素病及黑色素瘤开辟了一条新途径,在化妆品行业和临床医学应用方面具有开发价值,为进一步对有效成分的提纯、开发和利用打下基础。
2.6本章小结
1.用石油醚、乙酸乙酯、正丁醇将红缨合耳菊提取物依次进行萃取,初步对其进行分离提取,得到四个不同极性段的物质。
2.测定了红缨合耳菊提取物对酪氨酸酶单酚酶的影响,研究发现乙酸乙酯及正丁醇萃取部分对单酚酶有强的抑制作用,半数抑制率IC5分别为57.8、140ug/mL。
3.测定了乙酸乙酯及正丁醇萃取部分对单酚酶的延迟作用,82.8g/mLEAF部分使得酶的稳态活力下降了.82.1%、使迟滞时间从78S延长到223S;170.8Hg/mL的BF部分使得酶的稳态活力下降了69.4%、使迟滞时间从78S延长到173 S
4.测定了测定了红缨合耳菊提取物对酪氨酸酶双酚酶的影响,研究发现乙酸乙酯及正丁醇萃取部分对单酚酶有强的抑制作用,半数抑制率ICs0分别为41.259.6 g/mL.
5.研究了乙酸乙酯及正丁醇萃取部分对双酚酶的抑制作用类型,发现EAF部分对二酚酶的抑制作用表现为可逆竞争性抑制类型,抑制常数为19.7g/mL;nBF部分对二酚酶抑制作用表现为可逆非竞争性抑制类型,抑制常数为60.7ug/mL。
未完待续……
- 星期一, 17 6月 2024
西藏红缨合耳菊提取物的美白机理研究(一)
摘 要
西藏红缨合耳菊(Synotis erythropappa (Bur.et Franch)C. Jeffrey et Y. L. Chen)为菊科(Compositae)植物,属西藏特有植物。产于西藏东南部,西藏当地女性将红缨合耳菊捣碎、烧成灰等后,敷在皮肤表面用于皮肤保养及紫外线防护。黑色素的大量产生是皮肤变黑的重要原因,人体中酪氨酸酶是催化酪氨酸形成多巴,以及多巴形成多巴醌,并最终产生黑色素的关键酶。羟自由基是人体内产生的不稳定的且具有强氧化性的物质,与人体的衰老有密切的联系,氧自由基同样对人体的衰老有密切关系,同时它也在黑色素的形成过程中起到氧化的作用。当自由基大量产生,又得不到有效的清除时,会导致机体组织不断老化。
本文通过研究红缨合耳菊提取物的美白机理,包括红缨合耳菊提取物对酪氨酸酶的抑制作用、B16细胞的影响、自由基清除作用等,探讨了红缨合耳菊在美白方面的功效。取得的结果如下:
一、以酪氨酸为底物,探讨红缨合耳菊提取物酪氨酸酶单酚酶的抑制效果结果表明红缨合耳菊提取物的乙酸乙酯及正丁醇萃取部分有较强的抑制能力,对酪氨酸酶单酚酶的半数抑制浓度IC50分别为57.8、140ug/mL。并能使抑制过程产生延迟作用。
二、以多巴为底物探讨红缨合耳菊提取物酪氨酸酶双酚酶的抑制效果。结果表明红缨合耳菊提取物的乙酸乙酯及正丁醇萃取部分有较强的抑制能力,对双酚酶的半数抑制浓度IC50分别为41.2、59.6ug/mL。通过动力学实验得出抑制类型分别为竞争性抑制以及非竞争性抑制。
三、探讨了红缨合耳菊提取物对B16细胞的影响,结果表明红缨合耳菊提取物对细胞形态和生长均有一定的抑制作用,其中以乙酸乙酯萃取部分最大320ug/mL时细胞生长抑制率可达到65.67%,而正丁醇萃取部分及水溶部分仅为10%左右。
四、红缨合耳菊提取物在抗氧化方面的研究,探讨红缨合耳菊提取物对DPPH和氧自由基的清除作用量。对羟自由基的清除作用在一定程度上可以与抗坏血酸相媲美。乙酸乙酯、正丁醇萃取部分半数清除率IC50分别为2.51、5.12ug/mL与抗坏血酸的ICso值2.42μg/mL相差不多,对氧自由基的半数抑制浓度IC50分为0.27、0.39 mg/mL.
上述实验证明红缨合耳菊提取物具有抑制酪氨酸酶单酚酶及双酚酶的作用对细胞有一定的毒性,此外还具有清除自由基、抗氧化损伤、抗衰老的双重功效有望用于美白护肤和抗衰老型化妆品中。
关键词:红缨合耳菊;酪氨酸酶;B16黑色素瘤细胞;自由基
Abstract
Synotis erythropappa (Bur.et Franch.)C, Jeffrey et Y.L. Chen is Compositae plant, as a natural plant of Tibet. They mainly product in east-nouth of Tibet. The females apple the triturate or ash of them to cure skin disease, Also to avid eultraviolet radiation. As we known, the product of melanin is responsible for the process of skin blackening. Besides, tyrosinase is a key enzyme which can catalyze tyrosine to L-DOPA, and catalyze L-DOPA to dioxyphenylalanine quinine.
Free radicals, a matter produced in vivo, which is close connection with ageing.is instable but powerful in oxidation, If plenty of the free radicals produced with out efficient cleaning, the prganism will be ageing uninterrupt, This paper do some research on the effect of the extract of Synotis erythropappa (Bur. et Franch.)C Jeffrey et Y,L. Chen on the cosmetology,Bl6 cells and antioxygen, From the rsearch of the effect on the inhibition ratio of the tyrosinase and the cleaning of freradicals, we get the following results:
The research of water extract of Synotis erythropappa (Bur. et Franch.)C. Jeffrey et Y.L. Chen on monophenol oxidase of tyrosinase. We discover that the four factions extracted all have inhibitory activities on tyrosinase, inhibitory activity of ethyl acetate and n-butanol fraction are higher than others, concentration that resultsin 50% activity(ICso) lost is 57.8、140 μg/mL, Also they Can extend the lag of the action time of monophenol oxidase.
The research of water extract of Synotis erythropappa (Bur. et Franch.)C Jefrey et Y L. Chen on diphenol oxidase of tyrosinase. We discover that the four fractions extracted all have inhibitory activities on tyrosinase, inhibitory activity of ethyl acetate and n-butanol fraction are higher than others, concentration that resultsin 50% activity(ICso) lost is 41l.2、59.6 μg/mL, The inhibition kinetics analyzed by Hnewaver-Burk plots showed that ethyl acetate faction is a competitive type inhibitor, and the inhibition constants for free enzyme(K¡) was determined to be19.7μg/mL. n-butanol fraction is a uncompetitive type inhibitor, and the inhibition constants for free enzyme(K¡) was determined to be 60.7 μg/mL.
The research of extract from Synotis erythropappa(Bur. et Franch.)C. Jeffrey et Y,L. Chen on Bl6 cells. We discover that the four fractions extracted all have inhibitory activities on B16 cells, inhibitory activity of ethyl acetate fractionare higher than others, ICso is 65.67%.
The research of extract of Synotis erythropappa (Bur. et Franch.) C. Jeffreyet Y, L. Chen on free radicals. We discover that the four fractions extracted all haveinhibitory activities on free radicals, inhibitory activity of ethyl acetate and n-butanol fraction are higher than others, IC50 is 2.51、5.12 g/ml on DPPH and 0.27、0.39mg/mL on oxygen free radicals.
The above-mentioned research demonstrates that Synotis erythropappa (Bur. etFranch,)C, Jeffrey et Y,L. Chen has the effect on skin whitening anf anti-ageing. Soit is promising be used in skin protection cosmetics.
Key word: Synotis erythropappa (Bur. et Franch.)C. Jeffrey et Y. L. Chen; tyrosinase: Bl6 cell; free radicals.
- 星期五, 14 6月 2024
光声电治疗术后皮肤黏膜屏障修复专家共识
中华医学会医学美容学会激光美容学组,中华医学会皮肤性病学会美容激光学组
[关键词】 皮肤黏膜修复,光声电治疗术后;共识
[中图分类号】 R751.05[文献标识码】Bdoi:10.16761/i.cnki.1000-4963.2019.05.019
[文章编号]1000-4963 2019)05-0319-04
- 星期四, 13 6月 2024
西藏红缨合耳菊提取物对酪氨酸酶的抑制作用
徐学涛1,张:l昆h,杜志云’,郑劭1,方岩雄1,卫星船1,赵肃清1,俞新华2(1.广东工业大学轻工化工学院,广东广州510006;2.华南农业大学生命科学学院,广东广州510642)
摘要目的:研究西藏红缨合耳菊提取物对酪氨酸酶的抑制作用。方法:将红缨合耳菊的70%乙醇提取物依次用石油醚、乙酸乙酯、正丁醇萃取。然后测定各部分对酪氨酸酶的抑制作用,并进行酶抑制动力学研究。结果:乙酸乙酯、正丁醇的萃取部分对酪氨酸酶的活性抑制较强;对单酚酶抑制作用明显并有延迟作用,半数抑制浓度(IC50)分别为57.8、140 pg/ml;对双酚酶的抑制作用显示浓度依赖关系,IC50分别为4I.2、59.6∥lIll,相比熊果苷抑制双酚酶活性的Ic,。值1.44rag/ml,抑制效果分别是熊果苷的35、24倍;抑制类型:乙酸乙酯部分为竞争性抑制,晒为19.7斗g/mJ,正丁醇部分为非竞争性抑制,鼬为60.7t∥ml。结论:西藏红缨合耳菊乙醇提取物的乙酸乙酯、正丁醇萃取部分对酪氨酸酶活性抑制较强。
关键词红缨合耳菊;酪氨酸酶;化妆品
中图分类号:R285.5
文献标识码:A
文章编号:1001掣54(2008)10-1544-04
Inhibition of Extracts from Synotis erythropappa OR Tyrosinase XU Xue·ta01,ZHANG Kunl,DU Zhi—yunl,ZHENG Jie。,FANG Yan.xiong‘,WE/Xing-ehuanl,ZHAO Su.qing。,YU Xin.hna2
(1.Faculty of Chemical Engineering and Light Industry,Guangdong University of Technology,Guangzhou 510006,China;2.College of Life Science,South China Agricultural University,Guangzhou 510642,China)
Abstract
Objectire:To study the inhibition of extracts from Synotis erythropappa On tyrosinase.Methods:The 70%ethanol ex. tracts were extracted by petroleum benzine,ethyl acetate and n-butanol,and the inhibitory activities against tyrosinase of every fraction were determined in vitro and the inhibitory kinetics of ethyl acetate and n-butanol fractions we地investigated.Results:The four fractions extracted all had inhibitory activities on tyrosinase。inhibitory activities of ethyl acetate and n-butanol fraction were higher.Their IC50 were 57.8、140 t,#ml for monophenol oxidase activity and 41.2、59.6 w旷IIll for diphenol oxidase activity,respectively.The inhibition kinetics analyzed by Hnewaver—Bunk plots showed that ethyl acetate fraction was a competitive type inhibitor,and its Ki Was de—termined to be 19.7 pe,/mL n·butanol fraction was an uncompetitive type inhibitor,and its Ki Was determined to be 60.7¨∥m1.Conclusion:Ethyl acetate and n—butanol fractions of extracts from Synotis erythropappa show potential inhibitory activity on tymsinase.
Key words
Synot/s erythropappa(Bur.et France)C.Jeffrey et Y.L Chen;Tyrosinase;Cosmetic
- 星期二, 11 6月 2024
光声电治疗术后皮肤黏膜屏障修复专家共识
中华医学会医学美容学会激光美容学组,中华医学会皮肤性病学会美容激光学组
[关键词] 皮肤黏膜修复,光声电治疗术后;共识[中图分类号1R751.05[文献标识码]B
文章编号]1000-4963 2019)05-0319-04
doi:10.16761/i.enki.1000-4963.2019.05.019
- 星期五, 07 6月 2024
中国年龄相关性黄斑变性临床诊疗指南 (2023年)
中华医学会眼科学分会眼底病学组 中国医师协会眼科医师分会眼底病学组
通信作者:许迅,上海交通大学医学院附属第一人民医院眼科 国家眼部疾病临床医学
研究中心 上海市眼底病重点实验室 上海眼视觉与光医学工程技术研究中心 上海市眼科疾病精准诊疗工程技术研究中心,上海 200080,Email:该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。
【摘要】 年龄相关性黄斑变性(AMD)是老年人群低视力乃至失明的主要原因,随着我国人口老龄化加剧,AMD的患病人数将持续上升。近10年,眼底影像学检查技术飞速发展,为AMD的分型、诊断和随访提供了新的视角和途径,新药的开发为 AMD尤其新生血管性 AMD提供了更为多样的干预和治疗方法,而强调精准个体化治疗对眼底病医师提出了更高要求。为此,中华医学会眼科学分会眼底病学组、中国医师协会眼科医师分会眼底病学组与国家眼部疾病临床医学研究中心基于最新循证医学证据,结合国际指南和我国社会经济发展现状,围绕 8个临床问题提出推荐意见,形成了我国的AMD临床诊疗指南,以期加强和完善我国AMD诊疗工作的规范化,提高我国AMD的诊疗、预防和随访水平。(本文于2023年4月6日优先出版在中华眼科杂志官网)
【关键词】 黄斑变性; 诊疗准则(主题); 循证医学
实践指南注册:国际实践指南注册与透明化平台,IPGPR‑2021CN111
Evidence‑based guidelines for diagnosis and treatment of age‑related macular degeneration in China (2023)
Chinese Vitreo‑Retina Society of Chinese Medical Association, Fundus Disease Group of Chinese Ophthalmologist Association
Corresponding author: Xu Xun, Department of Ophthalmology, Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine, National Clinical Research Center for Eye Diseases, Shanghai
Key Laboratory of Ocular Fundus Diseases, Shanghai Engineering Center for Visual Science and Photomedicine, Shanghai Engineering Center for Precise Diagnosis and Treatment of Eye Diseases,
Shanghai 200080, China, Email: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。
【Abstract】 Age‑related macular degeneration (AMD) is the main cause of low vision and even blindness in the elderly. With the aging of our population, the number of AMD patients will continue to rise. In the past decade, the rapid development of ocular fundus imaging technology has provided a new perspective and approach for the classification, diagnosis and follow‑up of AMD. The advent of new drugs has provided more diverse intervention and treatment methods for AMD, especially for neovascular AMD, and the emphasis on accurate and individualized treatment has put forward higher requirements for retinal specialists. Therefore, based on the latest evidence‑based medical information, combined with the international guidelines and the current situation of China′s social and economic development, experts from the Chinese Vitreo‑Retinal Society of Chinese Medical Association, the Fundus Disease Group of Chinese Ophthalmologist Association, and the National Clinical Research Center for Eye Diseases gave recommendations around eight clinical problems and formed China′s guidelines for the clinical diagnosis and treatment of AMD. With the implementation of these guidelines, we can standardize the diagnosis, treatment, prevention and follow‑up of AMD in China. (This article was published ahead of print on the official website of Chinese Journal of Ophthalmology on April 6, 2023)
【Key words】
Macular degeneration;
Practice guidelines as topic;
Evidence‑based
medicine
Practice guideline registration: Practice Guideline Registration for Transparency, IPGRD‑2021CN111

{kind=link}
{kind=link}
{kind=link}
{kind=link}