
Achronic wound is one that fails to recover through an orderly process into a healed state. Wound healing usually stalls in the homeostasis/inflammatory phase due to cellular, microbial, and biochemical irregularity. Clinical studies show that delayed healing is heavily influenced by external factors (wound care, wound surface area, wound age) and patientrelated factors (comorbidities, non-concordance with first-line therapy, history of diabetes mellitus and/or deep venous thrombosis, BMI over 25) (Scalise et al, 2017). In order to optimise the wound healing process, there are currently two mainstream models for wound bed preparation namely TIME, t=tissue management, i=infection or inflammation, m=moisture balance, and e=edge of wound (Schultz et al, 2003) and DIME, d=debridement/devitalised tissue, i=infection or inflammation, m=moisture balance, and e=wound edge preparation/wound depth, (Synder et al, 2016).
Regardless of the increasing amount of research in wound care, the mushrooming of advanced dressings, and solid frameworks for wound management, wound healing is often set back by weeks, if not months (Onesti et al, 2013). Thorough wound closure is achieved in merely 25% to 50% of chronic or hard-to-heal cases, particularly for venous leg ulcers (VLU) and diabetic foot ulcers (DFU) (Falanga et al, 2008). To enhance wound bed preparation, the debridement of the slough, necrotic tissue, biofilm, bioburden, and apoptotic cells is critical to the management of a chronic wound. There are a number of different debridement methods, including biological debridement, surgical or mechanical debridement, autolytic debridement, and enzymatic debridement. The invasive nature of surgical or mechanical debridement usually requires anaesthesia or patients with a higher pain tolerance. On the other hand, autolytic and enzymatic debridement are more conservative methods.
Here we focus on enzymatic debridement using collagenase plus hyaluronic acid to actively target wound proteins and moisture retentive dressings for debridement enhancement. The latest evidence demonstrates the superiority of enzymatic debridement over autolytic debridement in accelerating re-epithelialisation as it specifically targets necrotic/sloughy tissue (Scalise et al, 2017).
Enzymatic debridement uses proteinases or natural proteolytic enzymes to facilitate wound repair by chemically dissolving the non-viable tissue within the wound bed. The proteinase activity also promotes re-epithelialisation, so that wound healing proceeds beyond the inflammatory phase into the proliferative and maturation phases (McCallon et al, 2015). This synergistic combination of collagenase and autolytic debridement amplifies the action of macrophage collagenase to disintegrate the proteins in the eschar. Standard procedure usually uses collagenase extracted from a specific strand of bacteria, Clostridium histolyticum (Scalise et al, 2017). However, another bacterial collagenase derived from Vibrio alginolyticus has been used in the enzyme debridement treatment, as it attacks the necrotic tissue, while leaving periwound healthy tissue intact (Di Pasquale et al, 2019). Its selectivity relies on the characteristic alkaline pH values of non-healing tissue that range between pH 7.15 and 8.9, while healing wounds are mildly acidic, with a pH generally lower than pH 7 (Percival et al, 2014). As the collagenase from Vibrio alginolyticus is only fully active at pH values ranging from 7 to 9, it perfectly overlaps with the pH value of necrotic tissues (Scalise et al, 2017).
Apart from the collagenase in action, studies have pointed to the vital role of moisture retentive agents in all phases of wound healing from inflammation to wound closure. Among many moisture retentive agents, hyaluronic acid stands out due to its efficacy in supporting wound healing as an integral part of the extracellular matrix (ECM) and by mediating the CD44 receptor to speed up the re-epithelialisation of the wound bed. Research has shown that applying hyaluronic acid also improves healing time and reduces scar formation (Leite and Frade, 2021).
Hyalo4® Start (Fidia Farmaceutici S.P.A.) is an enzymatic debriding ointment that amalgamates the proteinase, collagenase derived from non-pathogenic Vibrio alginolyticus and sodium hyaluronate 0.2%. It is designed as a convenient topical ointment in line with the TIME doctrine of wound bed management that customises the needs of different patients with chronic wounds. A previous case study has shown positive outcomes with Hyalo4 Start though the study is limited in sample size and patient aetiologies (Nair et al, 2020a).
Objective
This study aims to establish the clinical benefits of new enzyme debridement topical ointment containing collagenase and hyaluronic acid (Hyalo4® Start) in chronic wounds.
Methodology
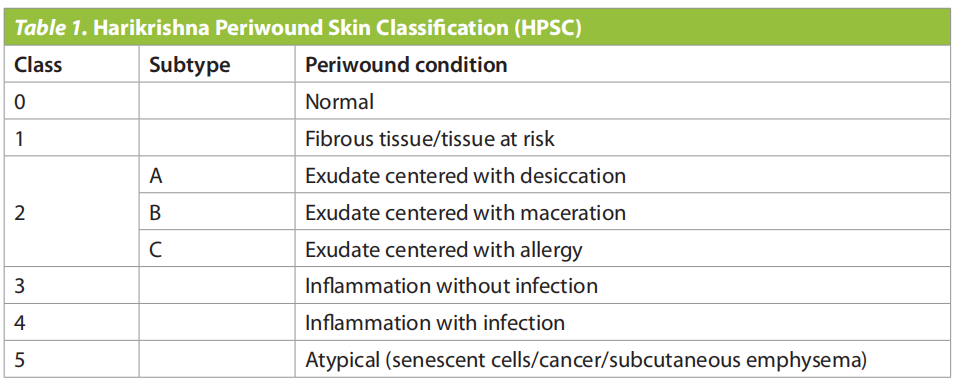
The case series study took place in Wound Care Clinic Hospital Kuala Lumpur between October 2021 to August 2022. It involved patients with chronic wounds (venous and arterial lower limbs ulcers, DFUs, and pressure ulcers). A convenience sampling method was used for this case series, and the inclusion criteria included patients admitted with lower limbs localised wounds present for more than one month. Wounds were assessed using TIME concept and Harikrishna Periwound Skin Classification (HPSC) to determine the status of the wound bed and the condition of periwound skin (Nair et al, 2020b) (Table 1). Only patients with a chronic wound, exudate and/ or inflammation with no infection, classified within HSPC Class 2 and 3 were included. All patients underwent the same procedure on the ward, and were treated by nurses. All wounds were rinsed with sterile water, followed by basic bedside enzymatic debridement with topical application of Hyalo4 Start as the standard of care. For the periwound area, polyurethane foam was applied following the barrier ointment. The dressing was changed every other day and reviewed in the clinic three times per week until the end of the study. Offloading with paddings was designated for DFUs, while 2-layer compression treatment was given for patients with VLUs. No other advanced dressings that could alter the healing times were employed for this study.
Measurement of wounds (length x width) and their progress was assessed every time the dressing was changed. To rate pain sensation, a visual analogue scale (VAS) assessment was performed before treatment, and weekly during the period the studies took place (Quinn and Wells, 1998). Patients were asked to rate their pain score from 0 (no pain) to 10 (maximal pain sensation).
This case series was carried out in accordance with the Declaration of Helsinki’s guidelines and approved by the hospital’s review board. Patients gave consent to use clinical images and case details for publication/research purposes before the start of the study.
Results
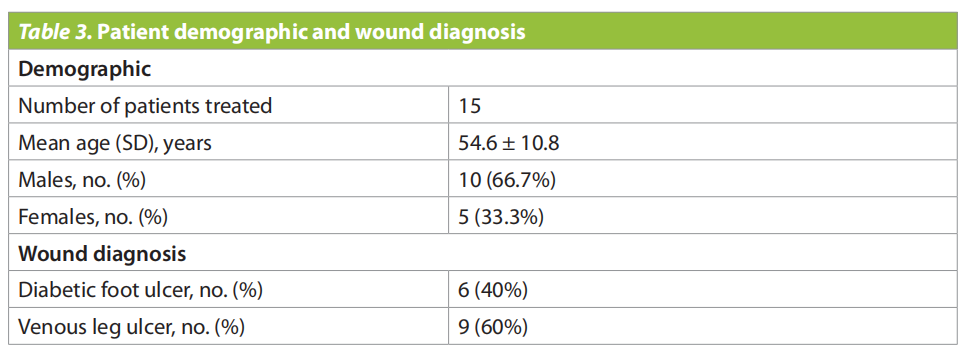
We recruited 15 patients (10 male, 5 female; (Table 3). The patients had differnet comorbidites i.e., diabetes mellitus (n=9), central cord syndrome quadriplegia (n=1), hypertension (n=9), and no known medical illness (n=3).
Among all patient, six of the patients were diagnosed with DFU while the remaining nine patients were diagnosed with VLU (Table 3).
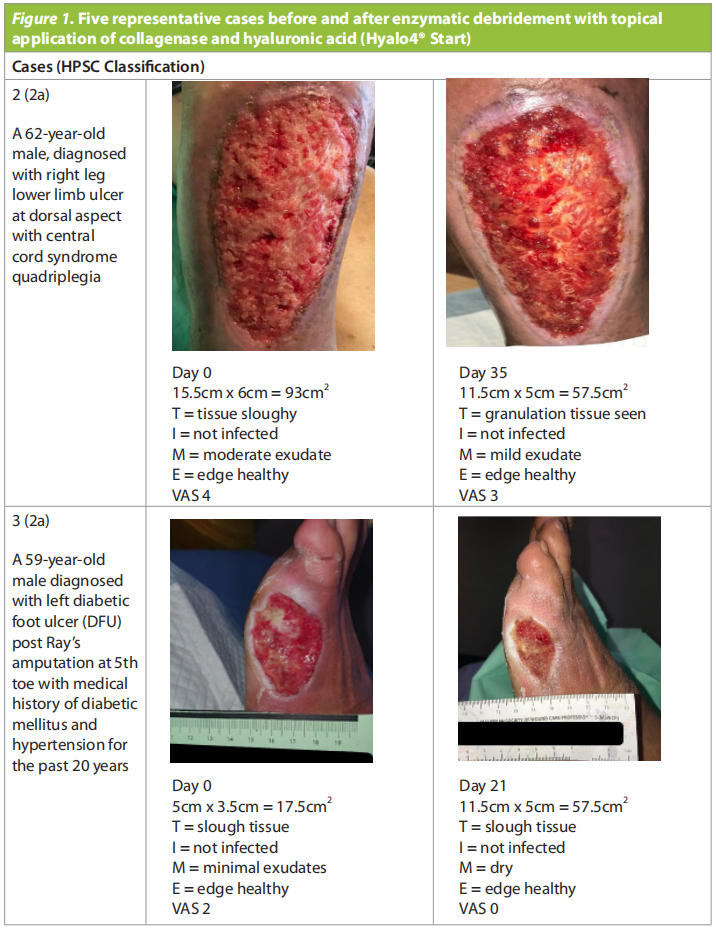
Below are five typical chronic wound cases found in Wound Care Clinic in Hospital Kuala Lumpur (Figure 1).


At the end of the study, out of the 15 patients, 8 patients achieved a large wound size reduction, 12 of them achieved a significant reduction of exudate and improvement of wound bed (granulation tissue observed on eight patients), and one patient achieved wound closure (Figure 2). Wound size reduction in the 8 patients ranged from 20–100%.
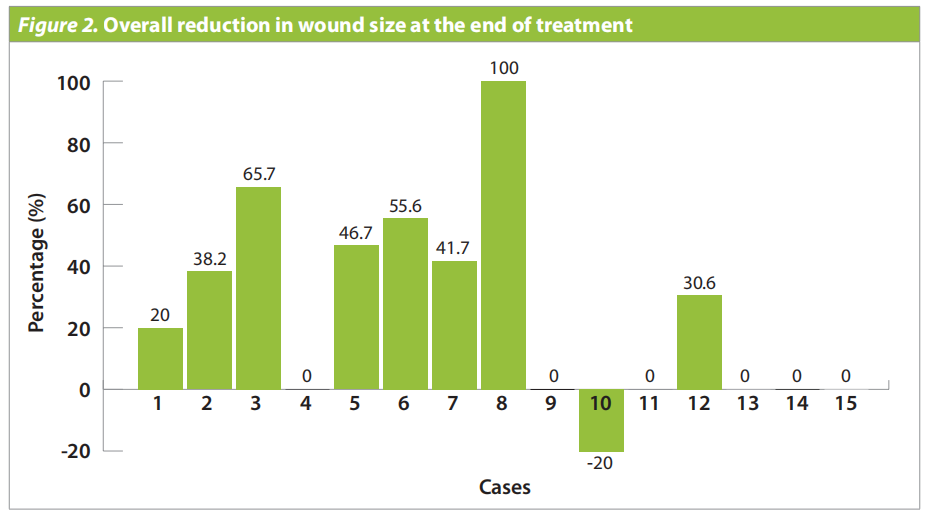
Table 2 describes five cases where wound reduction occurred after treatment. The wound size was maintained in six patients and one patient had a larger wound by the end of the treatment, although the exudate had dried up or diminished to a minimum for all seven. Only one patient did not experience any improvement regarding wound size, exudate excretion, and periwound tissue edge, although the patient reported 0 pain towards the end of treatment. All patients described 1 to 2 points of pain reduction as assessed using VAS score, 12 patients reported a minimal pain score of 1 or 2 points at the end of treatment, while three patients reported no pain. As patients recruited reported low VAS pain scores before treatment, the described pain sensation reduction ranged from 25% (n=2) to an astounding 100% (n=4) after treatment with Hyalo4 Start.
Discussion
In parallel with previous studies, all patients who had wounds for more than one month, the topical application of Hyalo4® Start seems to resume the wound healing stop clock (Onesti et al, 2013; Onesti et al, 2016; Scalise et al, 2017). As the duration of treatment for the patients recruited differed significantly, the result varied substantially. However, the improvement pattern indicates that the wound healing rate picks up significantly after more than 12 days of treatment with Hyalo4 Start. Out of 7 patients that saw no reduction or an increase in wound size, four were treated for less than 12 days. One patient with DFU who had been treated for 12 days had a large lesion (wound size = 100cm2 ). However, the sloughy tissue had become viable, and the exudate had stopped. Another anomaly was a patient with DFU that had been treated for 63 days. However, the wound tissue barely turned viable, and there was no reduction in wound size other than the absence of exudate. Finally, one patient with a relatively small wound size (10cm2 ) showed no improvement in all aspects except for pain score despite being treated for 21 days.
The delayed wound healing might be related to poor concordance, to either the offloading shoe for DFUs or to compression therapy for VLUs (Kavitha et al, 2014; Raffetto et al, 2020). This finding signals that although enzyme debridement is a beneficial insert in chronic wound care management, other factors could lead to stalled wound healing. Poor wound healing could also be associated with underlying comorbidities, personal hygiene care, professional execution of first-line therapy (offloading and compression therapy), and the initial wound size (Stadelmann et al, 1998).
Clinical observations show that there is no dermatitis or periwound abrasion following the topical treatment of Hyalo4 Start, thus endorsing the selectivity of the collagenase used in the formulation. Having intact periwound tissue should speed up the wound healing process and leave the patient generally more comfortable. It is worth noting that the improvement in wound size, excretion of exudate and reduced pain score in patients with different underlying comorbidities, suggesting that Hyalo4 Start works for patients with varying aetiologies (Hyalo4 Start Concise Product Info, 2016). One interesting finding is that the wound healing rate is not correlated with the age of patients recruited.
Last but not least, it is noteworthy that all patients reported considerably low pain scores before the treatment with Hyalo4 Start, ranging from 1 point to 4 points, and 12 of the patients reported to rate pain scores of 2 and lower after the treatment. A plausible explanation for the reduced pain score could be attributed to hyaluronic acid’s ability to mitigate pain by activating k-opioid receptors (Zavan et al, 2013).
Limitations
Limitations for this study include the lack of monitoring of nutrition intake, length of the treatment period, and chronic wounds classified as Class 4 and 5 as by the HSPC were not included as more aggressive treatment would be required for such wounds. More studies are required to address the missing data of this case study.
Conclusion
This case series study demonstrated the clinical efficacy of hyaluronic acid and collagenase ointment (Hyalo4 Start) in promoting wound debridement and closure. Effective wound debridement was observed in 15 out of 16 patients. Wound size and exudate level reduction, as well as a pain score improvement indicate that Hyalo4 Start aids wound healing in patients with DFUs, VLUs and arterial lower limbs ulcers. The selective action on wound tissue and simple treatment of the topical ointment has the potential to be valuable in wound care management in the healthcare. The result are similar to those of the previous study, which had a smaller sample size. Thus adding to the suggestion that advanced enzymatic debridement formulation could be a a useful tool in routine chronic non-infectious wound management.
Declaration of interest:
EP Plus Group supplied the hyaluronic acid and collagenase ointment (Hyalo4® Start) used for this study. However, the author has no conflicts of interest to declare.
REFERENCES
1. Di Pasquale R, Vaccaro S, Caputo M, et al (2019) Collagenase-assisted wound bed preparation: An in vitro comparison between Vibrio alginolyticus and Clostridium histolyticum collagenases on substrate specificity. Int Wound J 16(4):1013–23. https://doi. org/10.1111/iwj.13148
2. Falanga V, Brem H, Ennis WJ et al (2008) Maintenance debridement in the treatment of difficult-to-heal chronic wounds. Recommendations of an expert panel. Ostomy Wound Manage Suppl:2–13
3. Hyalo4® Start (2016) Concise Product Info. https://tinyurl. com/4t5nwxc7 (accessed 3 October 2022)
4. Kavitha KV, Tiwari S, Purandare VB et al (2014) Choice of wound care in diabetic foot ulcer: A practical approach. World J Diabetes 15;5(4):546–56. https://doi. org/10.4239%2Fwjd.v5.i4.546
5. Leite MN, Frade MAC (2021) Efficacy of 0.2% hyaluronic acid in the healing of skin abrasions in rats. Heliyon 7(7):e07572. https://doi.org/10.1016%2Fj.heliyon.2021. e07572
6. McCallon SK, Weir D, Lantis JC 2nd (2015) Optimizing wound bed preparation with collagenase enzymatic debridement. J Am Coll Clin Wound Spec 6(1-2):14–23. https://doi.org/10.1016/j.jccw.2015.08.003
7. Nair HKR, Chong SS, Othman AM (2020) Validation of Harikrishna Periwound Skin Classification for wound assessment. J Wound Care 29(Sup4):S44–8. https://doi. org/10.12968/jowc.2020.29.sup4.s44
8. Nair HKR et al (2020) Application of hyaluronic acid and collagenase ointment in the treatment of chronic wounds: a case series. Wounds Asia 3(2):48–54.
9. Percival SL , McCarty S, Hunt JA, Woods EJ (2014) The effects of pH on wound healing, biofilms, and antimicrobial efficacy. Wound Repair Regen 22:174–86.
10. Onesti MG, Fioramonti P, Carella S, Fino P, Sorvillo V, Scuderi N (2013) A new association between hyaluronic acid and collagenase in wound repair: an open study. Eur Rev Med Pharmacol Sci 17(2):210–6.
11. Onesti MG, Fioramonti P, Fino P et al (2016) Effect of enzymatic debridement with two different collagenases versus mechanical debridement on chronic hard-to-heal wounds. Int Wound J 13(6): 1111–15. https://doi.org/10.1111/iwj.12421
12. Quinn JV, Wells GA (1998) An assessment of clinical wound evaluation scales. Acad Emerg Med 5(6):583–6. https:// doi.org/10.1111/j.1553-2712.1998.tb02465.x
13. Raffetto JD, Ligi D, Maniscalco R et al (2020) Why venous leg ulcers have difficulty healing: overview on pathophysiology, clinical consequences, and treatment. J Clin Med 24;10(1):29. https://doi. org/10.3390/jcm10010029
14. Scalise A, Campitiello F, Della Corte A et al (2017) Enzymatic debridement: is HA-collagenase the right synergy? Randomized double-blind controlled clinical trial in venous leg ulcers. Eur Rev Med Pharmacol Sci 21(6):1421–31.
15. Schultz GS, Sibbald RG, Falanga V et al (2003) Wound bed preparation: a systematic approach to wound management. Wound Repair Regen 11 Suppl 1:S1–28. https://doi.org/10.1046/j.1524-475x.11.s2.1.x
16. Snyder RJ, Fife C, Moore Z (2016) Components and quality measures of DIME (devitalized tissue, infection/ inflammation, moisture balance, and edge preparation) in wound care. Adv Skin Wound Care 29(5):205–15. https://doi.org/10.1097%2F01.ASW.0000482354.01988. b4
17. Stadelmann WK, Digenis AG, Tobin GR (1998) Impediments to wound healing. Am J Surg 176(2A Suppl):39S-47S. https://doi.org/10.1016/s0002-9610(98)00184-6
18. Zavan B, Ferroni L, Giorgi C et al (2013) Hyaluronic acid induces activation of the κ-opiod receptor. PLoS One 8(1): e55510. https://doi.org/10.1371/journal. pone.0055510
This article is excerpted from the Wounds Asia 2022 | Vol 5 Issue 3 | by Wound world.

