
Keywords
Issue: Volume 58 - Issue 9 - September 2012
Index: Ostomy Wound Manage. 2012;58(9):16‚31.
Login or Register to download PDF
Abstract
Wound care professionals can improve clinical, patient-oriented wound outcomes and do so cost-effectively by using scientific evidence to meet patient and wound care goals and needs. A review of the literature was conducted to define evidence-based wound management, describe the potential of science to improve outcomes in wound care, and summarize strategies, tactics, and tools for wound care providers and recipients to utilize science to their mutual benefit.
In addition, changes in the availability of randomized and nonrandomized and clinical and preclinical evidence during the past 50 years were examined using MEDLINE database searches of English-language publications, combining the search terms wound, ulcer, or burn limited by the terms randomized or clinical for each decade since 1960. The number of published, nonrandomized wound studies has increased exponentially during the last five decades but, more recently, evidence from randomized controlled trials also has become available. Moreover, while many questions remain unanswered, a substantial number of publications have shown the use of available evidence-based guidelines and wound care strategies improves outcomes of care while saving time and money. The application of science-based wound care in clinical practice is increasing slowly; expensive techniques supported by limited or inconsistent evidence are still in use and add to wound care costs without certainty they improve outcomes. The literature provides compelling evidence that patients with a wide variety of diagnoses benefit when opinion-based care is replaced by clinical wisdom applied on a substrate of best available evidence. Patients with wounds deserve no less.
This article is based on the John Boswick Memorial award lecture presented at the Symposium on Advanced Wound Care, Gaylord Texan Conference Center, Dallas, TX. April 16, 2011.
Potential Conflicts of Interest: Dr. Bolton discloses she is a consultant or paid advisory board member for ConvaTec (Skillman, NJ), Derma Sciences, Inc (Princeton, NJ), EuroMed (Orangeburg, NY), and Systagenix Wound Management (Quincy, MA), as well as an expert witness for Gordian Medical (Irvine, CA).
Introduction
Wound care spans current medical specialties, and although it is not prominent in its own right on the healthcare horizon, its weight as a medical subspecialty is increasing. A meta-analysis1 of venous and pressure ulcer clinical studies has shown good wound care can dramatically reduce use of medical resources and costs while improving patient outcomes. The global economic burden of wound care is approaching $20 billion,2 excluding burdens of reduced quality of life, independence, or capacity to work or interact with others, as well as the burden on overworked providers in all settings.
According to a 2009 literature review,3 in the US, more than 5.7 million individuals have chronic wounds that might have been prevented or might heal faster using evidence-based (EB) care; and many more postsurgical wound-related complications such as infection, amputation, deep vein thrombosis, or pressure ulcers (PUs) could be minimized using EB surgical and peri-operative care. Wielding evidence can help wound care professionals and recipients spend less while improving outcomes.
A review of the literature was conducted to 1) clarify the meaning of EB wound care, 2) illustrate how evidence improves wound care outcomes, and 3) provide examples of EB strategies, tactics, and tools that providers and recipients can use to improve wound care outcomes.
Methods
Historical literature reviews4,5 and Cochrane, PubMed, and Google literature searches were used to find and verify definitions and facts. MEDLINE database searches on February 1, 2011 using the terms wound, ulcer, or burn were limited by the terms randomized or clinical to derive approximate counts of randomized and nonrandomized clinical and preclinical studies found in each decade from 1960 through 2010. Examples of EB strategies, tools, and tactics were selected from searches of wound care guidelines on the Agency for Healthcare Research and Quality (AHRQ) website and the National Guideline Clearinghouse (www.guidelines.gov) to illustrate key tactics, tools, and strategies that were successful in implementing EB wound care.
Readers are encouraged to review the source references to assess relevance to their practice. The tabulated results were not intended to be a comprehensive listing of all historic events or EB tools, tactics, or strategies to improve wound care outcomes. Results of these searches were tabulated to list important events in the history of EB medical practice; resources for tools, tactics, and strategies for implementing EB care; and provide a few examples of costly interventions requiring more consistent, high-quality evidence of efficacy to confirm a beneficial effect on patient and/or wound outcomes.
What is EB Wound Care?
EB medical practice involves integrating clinical wisdom with the best available science to reach clinical decisions that optimize the relevance, statistical power, efficacy, and safety of patient-oriented care.6 This approach can be traced back to Hippocratic7displacement of Aesculepian myths in favor of meticulously recorded observations of the natural history of disease in actual patients (see Table 1).4,5 For more than 2,000 years, the impetus to use objective evidence was pitted against vested opinions regarding the need for pain and laudable pus to foster healing. Keen medical minds gradually came to appreciate the value of using standardized, unbiased observations to avoid preventable medical errors (eg, failure to wash hands) and promote performance measures to improve the quality of patient outcomes.
Strength of evidence. Today’s wound care provider has access to clear operational definitions of efficacy.8 The strength of evidence supporting aspects of wound diagnosis, screening, prevention, or treatment is assessed using standardized domains and ratings (see Figures 1a and 1b).9,10 The strongest evidence is the least biased. Random assignment of subjects to treatment and observation blinded to treatment can reduce bias. Strong evidence is further characterized by consistent results for precisely measured, directly relevant outcomes. Integrating these four characteristics, strength of evidence can be rated according to a scale such as shown in Figure 1b.
Strength of recommendation is graded highest if the recommendation is based on strong, consistent evidence that following this recommendation will provide maximum benefit and least harm to the patient (see Figure 1c).11
The Evidence 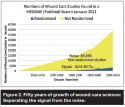


Evidence to guide decisions about wound care is more abundant than ever (see Figure 2). The MEDLINE search of randomized controlled trials (RCTs) revealed more than 5,218 wound-related RCTs during the last five decades, 3,285 of them clinical studies. Although RCTs can harbor methodological flaws, and most published wound care studies (n = 86,895) may be biased by nonrandomized assignment to treatment or unblinded outcome evaluation, discerning clinicians have ample science about efficacy and safety on which to base their decisions. Best evidence distilled as systematic reviews or meta-analyses is available at the websites listed in Table 2, with instructions for developing and recognizing high-quality EB guidelines,12 such as those available at the Department of Health and Human Services (HHS) AHRQ’s National Guideline Clearinghouse (www.guideline.gov). If the available reviews do not address the wound diagnosis of interest, more evidence is available by adding randomized to a search for relevant indications at the MEDLINE (PubMed) website (see Table 2).
In the 20th century, EB medical progress increased exponentially in areas as diverse as cardiology, dermatology, oncology, and radiology. Realizing that wound care should progress as well, providers started applying evidence to improve prevention and healing outcomes for acute and chronic wounds.
How does evidence improve wound care outcomes? Science helps improve wound outcomes by discriminating between what we do and do not know. It can help clinicians choose wound care interventions with best available evidence of efficacy and safety. Science also identifies equally effective, less costly interventions to achieve goals of care.
Successful application of EB medicine. A quasi-experimental, historically controlled study13 showed that regular EB-inservices on use of the Braden Scale and PU prevention techniques in a hospital-based home care agency reduced client PU prevalence from a baseline of 19% to 7.4% 4 months after the inservices to 6.7% and 8% after 8 and 18 months, respectively. In a quasi-experimental, historically controlled study14 of 69 pre-protocol subjects and 63 subjects using Braden Scale Risk scores of <18 in long-term care to focus EB PU care on the highest risk patients and on each patient’s most important areas of risk, the 6-month incidence of new PU decreased from 23% of 69 clients developing a PU before training on the EB protocol to 5% of 63 clients developing a PU while using the EB protocol, while reducing costs of care and the costs per day of a pressure ulcer-free life. In a prospective before-and-after study15 conducted among 88 residents of a Dutch nursing home, increased use of EB preventive mattresses from 27% to 45%, reduced mainly Grade 2 new PU incidence from 15% per month to 4.5% per month while reducing resource use. A quasi-experimental study16 comparing structured data abstracted from two retrospective studies in long-term care centers before implementing EB skin care protocols to similar prospective cohorts after implementing EB skin care showed EB skin care reduced the incidence of new PUs reported per month in a 150-bed long-term care facility from 13.2% to 1.5% and from 15% to 3.5% in a 110-bed long-term facility while reducing healing time and costs of managing existing Stage II PUs.
Meta-analyses reported that EB wound care using moisture-retentive dressings with a microbial-barrier reduced healing time, costs, and complications such as infection and pain in acute skin graft donor sites,17,18 other acute wounds including burns, traumatic wounds, skin graft donor sites, and chronic ulcers.18 A convenience sample19 of 117 patients whose coronary artery bypass graft sternotomy incisions were dressed postoperatively once weekly with a hydrocolloid wound dressing experienced lower costs of care and a 3.4% surgical site infection (SSI) rate compared to a 10.3% SSI rate (P <0.05) for 136 similar incisions dressed with an absorbent polyurethane foam pad dressing plus transparent film cover layer changed at postoperative day 2 to a nonocclusive adhesive pad dressing. Although the study may have been biased by surgeon age (younger surgeons used the hydrocolloid dressing), the only significant (P <0.05) operative procedure difference between groups was a longer arterial cross-clamp time and extracorporeal circulation time for patients operated on by the younger surgeons. Even though both procedure differences are ordinarily associated with an increased risk of complications, in this study the observed SSI for their patients was significantly lower. In a RCT among outpatients with diabetic foot ulcers,20 consistent EB offloading healed more Wagner Grade 1 or 2 ulcers in 12 weeks than was reported for patients wearing removable walker devices. These clinical healing outcomes with consistent offloading exceeded those reported from other RCTs on similar diabetic foot ulcers in outpatients for applying topical growth factors,21 bioengineered skin substitute,22 or autologous platelet gel.23
In a prospective cohort study in the Canadian Province of Nova Scotia,24 implementing EB protocols for home wound care clients reduced costs, resource use, and time to heal acute or chronic wounds compared to historic controls. Results of a retrospective (N = 120) versus prospective (N = 76) historically controlled, quasi-experimental study conducted in the US,25 showed that WOCNs consulting remotely through home telemedicine advising less-trained home care nurses to apply content-validated EB protocols of wound care on 76 clients reduced healing times of Stage II to Stage IV PUs, venous ulcers, and diabetic foot ulcers by an average of 4 to 11 weeks compared to 120 similar retrospective control patients from the same agencies per patient related to wound care from 60 at baseline to 33 with the EB WOCN consults, while significantly reducing the frequency of home care visits (P <0.05).
Wound professionals and patients in all settings have reported outcome benefits of EB care. Among the most challenging infectious disease cases presented at Walter Reed National Military Medical Center (WRNMMC) in Bethesda, MD are victims of improvised explosive devices (IEDs) concealed along the footpaths soldiers patrol in Afghanistan. The lower limb amputations are massively contaminated with soil and debris. Despite intensive surgical and medical management, the stumps may develop tenacious infections with molds from the environment. WRNMMC spends thousands of dollars apiece on USD Food and Drug Administration (FDA)-cleared devices to care for these desperately complicated patients despite a virtual absence of evidence about the comparative effectiveness of these proprietary systems compared to each other or to usual, customary care.26-33 Table 3 summarizes the less-than-compelling outcomes achieved using three such interventions.
Strategies, Tactics, and Tools to Improve Outcomes in Wound Care
Sound medical practice in wound care begins with an accurate diagnosis based on valid, reliable assessment techniques to determine patient- and wound-appropriate goals of care, then uses EB safe, effective actions to achieve them.34 The cycle continues by measuring progress with the same patient and wound assessment tools to ensure the actions taken are achieving their desired result (see Table 4).34,35
Figures 3 and 4, respectively, illustrate this goal-action-progress strategy using EB tactics and tools for venous and PU care. Each member of the wound care team who uses these strategies advances patient and wound progress, joining other EB medical professions providing high-quality care by doing “the right thing at the right time in the right way for the right person” to achieve “the best results possible.”36
Tactically, using evidence frees one to achieve desired wound outcomes instead of haphazardly caring for wounds without regard for the optimal results. Clinical cohort studies and literature reviews have shown wound care providers have improved client outcomes using a variety of different EB tactics, such as timely, appropriate interdisciplinary consults;37 multidisciplinary wound care teams;37,38 EB, content-validated wound and patient interventions;39-42 and staff education about procedures with evidence of safety, efficacy, and economy of resources.43 Wound care professionals and teams who utilize science to improve consistency and quality of wound and patient care and outcomes strive to provide patients with high-quality, consistent, timely, cost-effective care, benefitting their patients and institutions with improved outcomes while reducing resource use.
Putting EB methods to the test. To test how these strategies, tactics, and tools work in the real world, researchers used content-validated EB interventions to manage a cohort of 588 patients with chronic wounds, mainly cared for by minimally trained providers consulting with wound ostomy continence nurses (WOCNs).42 Most chronic venous or PUs healed in 12 weeks or less (see Figure 5) using these simple principles:34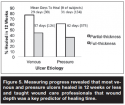
1. Wound care goals based on valid, reliable wound44 and patient45 assessments;
2. Patient-care goals based on valid, reliable patient chronic wound risk factors — eg, protect or offload immobile or insensate sites or reduce edema with appropriate compression;
3. EB, content-validated wound care decision tools or algorithms39-42 applied using moist wound healing combined, when needed, with autolytic debridement of necrotic tissue, adding moisture to dry wounds or absorbent primary dressings until excess exudate diminishes;
4. Healing progress documented and caregivers informed as soon as a wound departs from a normal healing trajectory.35 If wound areas do not decrease at least 20% during 4 weeks of care, patient and wound should be re-assessed to ensure all causes of tissue damage have been addressed properly.39-41
Documenting healing progress revealed that partial-thickness venous and PUs heal in half the time as similar full-thickness ulcers (see Figure 5). Time and resources were saved by limiting damage and healing chronic wounds while still shallow.42
Table 5 lists EB, validated tools that can help achieve patient and wound care goals. Using these tools achieves success only if blended with clinical experience and clear communication among wound care teams and care recipients. Putting a completed Braden Scale in the patient’s file does little good unless, for example, a mobility score of 1 is quickly and accurately communicated to the right personnel and results in appropriate action to redistribute pressure over affected pressure points.
Challenges to implementing EB strategies. Sometimes there are administrative or legal barriers to using EB tools. A scenario from the lab provides an example.
Background. Clinicians owe much to Hans Christian Joachim Gram (1853–1938), whose Gram stain made it possible to determine within seconds the identity of the likely etiological agent in a wound infection.47 By substituting guesswork for microscopy, the physician who prescribes broad-spectrum initial coverage can exacerbate the selection of treatment-resistant microbial strains while opening the door to adverse events from unneeded drugs. Furthermore, skipping microscopy means giving up an important screen for unusual pathogens that require more than routine management choices.
Nearly half a century ago, Paine49 lamented “a perpetual disinclination for doing Gram stains in situations in which the procedure would be helpful.” By streamlining the procedure, he hoped to further “an encouraging reawakening of interest in young physicians in making and examining Gram-stained smears from their own patients.” Instead, in 1988 the Clinical Laboratory Improvement Amendments (CLIA)50 made it a crime for all but CLIA-accredited laboratories to prepare and examine a Gram-stained smear as a part of a patient diagnosis. It should be noted that CLIA authority extends beyond the Centers for Medicare and Medicaid Services to patients who are not Medicare or Medicaid beneficiaries.
Potential scenario. A middle-aged man with diabetes mellitus is hospitalized with an apparently infected wound on his right leg. The practitioner would like advice from an infectious disease consultant. If Dr. Able is called, she will prepare a smear of the exudate and go down to the hospital’s microbiology laboratory to Gram-stain the slide and use one of the microscopes before returning to write some orders. If Dr. Baker is consulted, he will prescribe based on prior probabilities and modify his management the next day after checking with the laboratory to see what has come up overnight on the culture plates. However, Dr. Able would be in violation of CLIA unless she has been willing to spend hundreds of unreimbursed dollars annually as though she were a diagnostic laboratory.
According to EB medicine, to get the best from close encounters with micro-organisms, the clinician should perform (with the microbiologist) a good-quality quantitative swab46 and smear by dipping a dry swab in the exudate and then rolling the swab gently (to avoid shear forces on the leukocytes) on a glass slide to leave a thin film. A separate swab should be submitted for each type of stain or microscopical examination requested. The lab should be informed as to whether the smear was left to air-dry or fixed with heat or methanol.
When dealing with potentially infected wounds, the authors have found that proper sampling and quick, clear, communications with the microbiologist on the team can help inform antibiotic use decisions, long before the formal microbiology report is released. For example, if an acceptable specimen is sent to the lab on Monday morning, culture and sensitivity results might be expected by early Wednesday, although the laboratory technologist may have a good idea about the identity of the infecting agent much earlier from its appearance on the Gram-stained smear. By Tuesday morning, the colony morphology, whether the organism is hemolytic, some crucial details of its biochemistry, and even (although this is strictly forbidden) what it smells like can lead the technologist to be more-or-less confident of the genus and species of the pathogen. By the time the official report can be released on Wednesday, only the details of the antimicrobial susceptibility pattern may be news to the laboratory. In fact, because superficial specimens usually are not accepted for anaerobic culture, the only evidence of anaerobic bacterial involvement in a wound infection may be visualization on the Gram-stained smear of the mixed Gram-negative and Gram-positive cocci and bacilli characteristic of infections from oral, colonic, or vaginal bacteria. Getting to know early laboratory results requires time, diplomacy, and recognition that preliminary results should not be taken as the final word.
Legislation of science can be trying, but it need not cost patients’ lives. It is true that many physicians are not accomplished microscopists, but protecting patients against rogue Gram stainers is like making dental floss available only by prescription so people won’t become dangerously thin from flossing when they should be eating. When was the last time a cardiac surgeon was known to struggle with an orthopedist over how to adjust the condenser on the microscope? Meanwhile, the wound care facility may want to consider securing CLIA accreditation for direct specimen examination by microscopy, including Gram, methylene blue, and acid-fast smears at a minimum.
Limitations
This focused review is limited to a few examples to illustrate how EB tools, tactics, and strategies work to improve wound care outcomes. It is not comprehensive, only touching on major issues that need to be resolved with good science and the challenges inherent in any health strategy. Science is rarely perfect and never complete. Well-intentioned “experts” may draw inaccurate conclusions, but they are usually corrected with evidence51-56 (see Table 6). If RCT evidence related to meeting a particular patient’s needs or goals is available to enable comparison of clinically measured clinical outcomes for similar patients with cases published in the literature, is there any reason to ignore it? The clinician’s preferred protocol may be applied if no reported outcomes exceed his/her documented results — ie, no evidence conflicts with that protocol.
Conclusion
Neither scientists nor clinicians are perfect, but together they are lifting wound care out of the dark ages of opinion-based care. The research demonstrates compelling patient benefits when clinical wisdom acts on a substrate of the best available evidence. Although the literature still contains a lot more noise than signals, the amount of available evidence has increased in recent years and slowly, but surely, wound professionals are adopting strategies, tactics, and tools to improve wound care quality and outcomes. Clear operational definitions52,53 are being developed and honed to describe interventions, etiology, severity, and likelihood of healing. Screening and diagnostic risk factors are being validated appropriately. Interventions such as appropriate compression to reduce edema and moist wound healing are being defined. Wound care protocols and guidelines are evolving from the mainly consensus-based documents of the 1990s to content-validated, science-based tools that help providers use evidence to achieve wound and patient outcomes instead of simply caring for wounds. This best available evidence will help illuminate wound care decisions, improve outcomes, and make solid decisions free of opinions, fears, or biased sales pitches. Hippocrates was right:7 Science is a strong weapon against such ignorance. Providers and recipients of wound care have the right to know the scientific basis of their care options. The scientific method guided physics, chemistry, biology, and medicine away from the tyranny of untested opinion, improving clinical outcomes and expanding the healthcare universe and the capacity to utilize it. Providers and recipients of wound care deserve nothing less.
Disclaimer
The views and opinions expressed herein are solely those of the authors and do not necessarily state or reflect those of AHRQ, the Public Health Service (PHS), or the US Department of HHS. Reference in this article to any specific commercial products, process, service, manufacturer, company, or trademark does not constitute its endorsement or recommendation by AHRQ, the PHS, or HHS. As an agency of the US Government, the AHRQ cannot endorse or appear to endorse any specific commercial products or services.
Dr. Bolton is Adjunct Associate Professor, Department of Surgery (Bioengineering), Robert Wood Johnson University Medical School; and President, Bolton SCI, LLC, Metuchen, NJ. Dr. Baine is Senior Medical Advisor, Center for Outcomes and Evidence, Agency for Healthcare Research and Quality, US Department of Health and Human Services, Rockville, MD. Please address correspondence to: Laura L. Bolton, PhD, 15 Franklyn Place, Metuchen, NJ 08840; email: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。.

