Introduction
Acute abdominal conditions represent one of the most fre-quent causes of hospital admission to emergency medical and surgical wards and continue to pose a significant clini-cal challenge worldwide [1, 2]. They encompass a broad spectrum of pathologies, ranging from inflammatory to ischemic and obstructive processes, many of which require urgent diagnosis and timely intervention [3]. Their incidence rises steadily with age, and in older adults these conditions are often associated with a more complex clinical course, greater healthcare resource utilization, and increased post-operative morbidity and mortality [4, 5].
A critical issue in this population is the atypical clinical presentation [6]. In elderly patients, classical symptoms are often blunted or absent, which may delay recognition of the underlying disease. Instead of abdominal pain, which is tra-ditionally regarded as the cardinal feature, older adults may present with nonspecific signs such as confusion, anorexia, nausea, vomiting, or even falls [6, 7]. Notably, up to one-third of elderly patients with acute abdomen have been reported to present without abdominal pain, particularly among frail and multimorbid individuals [8, 9]. This con-dition, hereafter defined as asymptomatic acute abdomen (AAA), is strongly associated with diagnostic delays, inap-propriate treatment, and higher mortality [10].
Several factors have been proposed to contribute to asymptomatic acute abdomen (AAA) in older adults, includ-ing age-related changes in nociception, reduced visceral sensitivity, and the cumulative burden of comorbidities such as diabetes mellitus [11]. Type 2 diabetes mellitus (T2DM), which is highly prevalent in the elderly population, is asso-ciated with chronic microvascular and neuro-metabolic complications, including peripheral neuropathy and auto-nomic dysfunction [12–14]. These conditions have been linked to altered pain perception and modified autonomic responses, which may contribute to atypical or attenuated clinical presentations of acute abdominal conditions [15– 18]. Conceptually, this phenomenon has been compared to silent myocardial ischemia in patients with diabetes [16]. This analogy, which is intended to support biological plau-sibility rather than to suggest identical pathophysiological mechanisms, have been described in gastrointestinal emer-gencies as well [17, 18].
Despite these observations, few studies have systemati-cally evaluated the relationship between T2DM, glycemic control, and AAA across different acute abdominal condi-tions [19, 20]. In particular, the influence of diabetes dura-tion and poor glycemic control on the likelihood of atypical presentations remains largely unexplored [21].
The aim of this cross-sectional analysis was to determine the prevalence of AAA in a population of elderly patients admitted with acute abdominal conditions and to identify predictors of asymptomatic presentation. We hypothesized that T2DM, especially when long-standing and poorly con-trolled, would be associated with an increased probability of AAA.
Methods
This was a cross-sectional study including all the patients aged≥65 years that were discharged, between January 2022 and December 2023, with a diagnosis of acute abdomen, from two tertiary care hospital wards (the Geriatrics Unit and the General and Emergency Surgery Unit of the Garib-aldi-Nesima Hospital, Catania, Italy).
Inclusion criteria were: (a) age≥65 years; (b) hospital admission due to an acute abdominal condition confirmed by imaging, endoscopy, or surgery. Exclusion criteria were: (a) incomplete clinical records; (b) non-abdominal acute conditions misclassified at triage.
Demographic characteristics, comorbidities, chronic medications, vital signs at admission, laboratory data, imaging findings, and final diagnosis were extracted from the patients’ medical records. The presence of abdominal pain at presentation was determined from triage documen-tation and coded dichotomously as present or absent (e.g. AAA).
The following baseline clinical, anthropometric and bio-chemical variables were evaluated: body weight, height, body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting plasma glucose (FPG), glycated hemoglobin (HbA1c, determined by high-performance liquid chromatography), total cholesterol, high density lipoprotein cholesterol (HDL-C), low density lipo-protein cholesterol (LDL-C, calculated with Friedewald for-mula if triglycerides value was lower than 400 mg/dl) [22], triglycerides (TG), creatinine levels, estimated glomerular filtration rate (according to the Chronic Kidney DiseaseEpidemiology Collaboration formula) [23], albumin-to-creatinine ratio (ACR), glutamic oxaloacetic transaminase (GOT), glutamic pyruvic transaminase (GPT), amylase, lipase, C-reactive protein (CRP), procalcitonin (PCT).
The presence of different comorbidities: hyperten-sion (SBP≥140 mmHg and/or DBP≥90 mmHg, or taking antihypertensive medication), established cardiovascular disease (e.g. myocardial infarction, heart failure, stroke), chronic kidney disease (e.g. if either eGFR<60 ml/min or ACR>30 mg/g), T2DM, obesity (BMI≥30 kg/m2 ), dyslip-idemia (defined according to the 2025 focused update of the 2019 ESC/EAS guidelines [24] or by already taking lipid-lowering drugs at the time of hospital admission), malignan- cies and chronic obstructive pulmonary diseases (COPD). Patients’ smoking habit and concomitant medications were also recorded.
The main study outcome was the evaluation of the absence/presence of abdominal pain at presentation accord-ing to different comorbidities.
Diabetes duration was calculated from the year of diag-nosis. Secondary analyses were restricted to the diabetic subgroup to evaluate associations between AAA, diabetes duration, and HbA1c levels at hospital ward admission. The study was conducted in accordance with the princi-ples of the Declaration of Helsinki and its later amendments [25]. Ethical committee approval was not required accord-ing to institutional regulations for retrospective analyses of anonymized data. For this type of study, informed consent was not required.
Statistical analysis
The available population determined the sample size; analy-ses should be therefore regarded as exploratory and hypoth-esis-generating. Given the clinical context and the risk of skewed distributions in older acute-care patients, continuous variables were primarily summarized as median and inter-quartile range [IQR]. Group comparisons were performed using non-parametric methods. Sensitivity analyses using parametric methods were conducted where appropriate to confirm robustness. Categorical variables are presented as absolute numbers and percentages.
Comparisons between groups (e.g. AAA vs. pain at pre-sentation) were performed using the Mann–Whitney U test for continuous variables, and the chi-square or Fisher’s exact test for categorical variables, as appropriate.
Univariate analyses were conducted for descriptive pur-poses only. Multivariable logistic regression analysis was used to explore factors associated with AAA and represents the primary analysis. The adjustment set was pre-specified a priori based on clinical relevance and data availability, and included age, sex, T2DM, heart rate, and presence of fever. All covariates were entered simultaneously into the model; no data-driven variable selection procedures were applied. Model performance metrics were not used for prediction purposes. Continuous predictors were modeled linearly due to sample size constraints. Analyses were conducted using a complete-case approach.
A two-sided p-value<0.05 was considered statistically significant. Statistical analyses were carried out using STATA software, version 18.0 (StataCorp, College Station, TX, USA).
Results
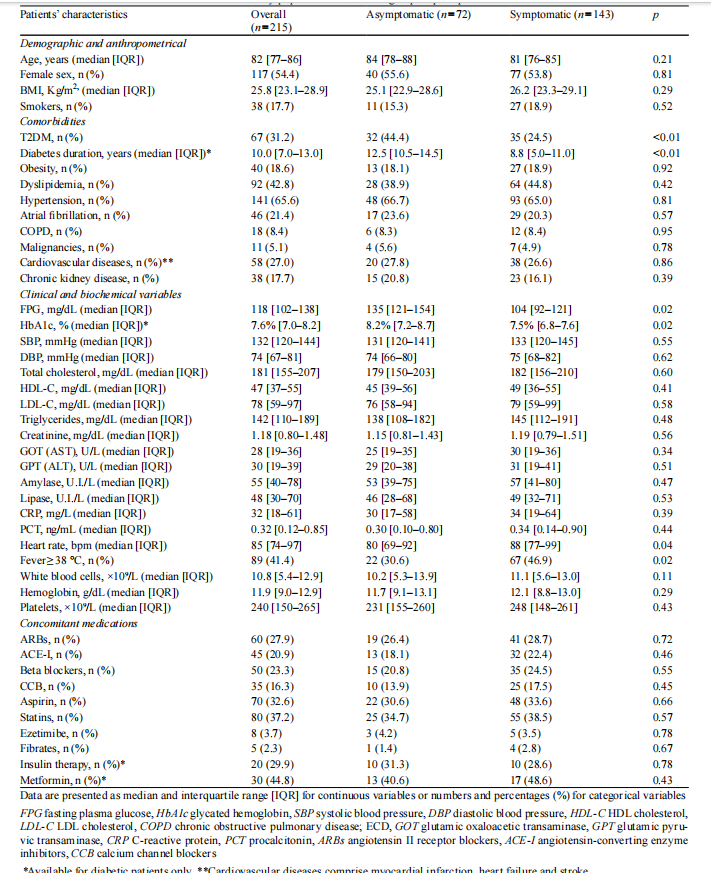
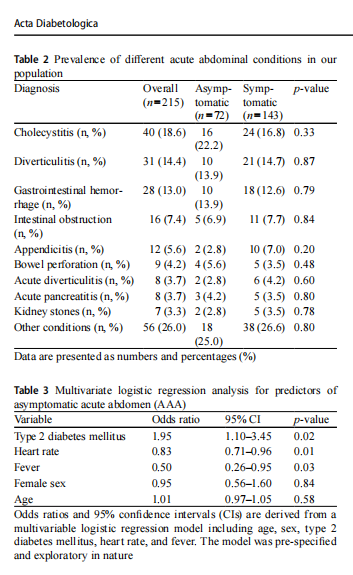
A total of 215 patients aged≥65 years were analyzed, with a median age of 82 years [77–86]; 54.4% (n=117) were female and 31.2% (n=67) were affected by T2DM. Overall, 72 patients (33.5%) presented without abdominal pain. The prevalence of T2DM was significantly higher in patients with AAA compared to those experiencing abdominal pain (44.4% vs. 24.5%, p<0.01). Clinical, anthropometrical and biochemical characteristics of the study population accord-ing to pain perception are summarized in Table 1. Patients with AAA displayed higher FPG (135 mg/dl [121–154] vs. 104 mg/dl [92–121]; p=0.02), higher HbA1c levels (8.2% [7.2–8.7] vs. 7.5% [6.8–7.6]; p=0.02), and a longer dura-tion of diabetes (12.5 years [10.5–14.5] vs. 8.8 [5.0–11.0]; p<<0.01) compared to those experiencing abdominal pain. The most frequent acute abdominal conditions were cho-lecystitis (18.6%), diverticulitis (14.4%), gastrointestinal hemorrhage (13.0%), intestinal obstruction (7.4%), acute appendicitis (5.6%), bowel perforation (4.2%), acute diver-ticulitis (3.7%), acute pancreatitis (3.7%) and kidney stones (3.3%), with no differences in their prevalence between the asymptomatic and symptomatic group (Table 2).
On multivariate logistic regression analysis several vari-ables were associated with AAA, including T2DM (OR 1.95, 95%CI 1.10–3.45, p=0.02), lower heart rate (OR 0.83, 95%CI 0.71–0.96, p=0.01) and the absence of fever (OR 0.50, 95%CI 0.26–0.95, p=0.03) (Table 3). Further evaluations were limited to the subgroup of patients with T2DM (n=67).
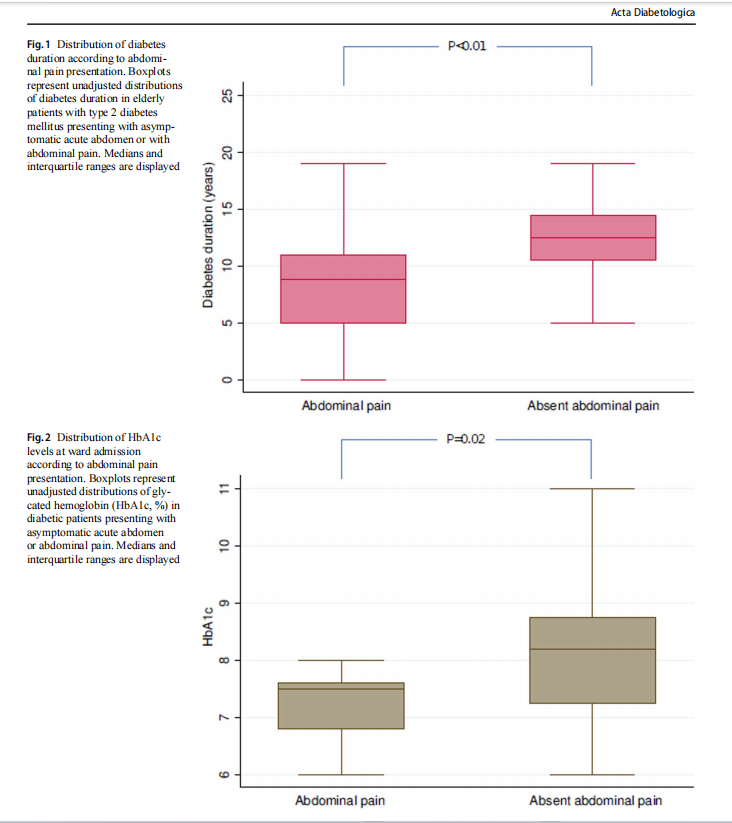
Figures 1 and 2 show the box-plot distribution of diabetes duration and HbA1c levels at ward admission according to abdominal pain presentation. Specifically, patients presenting with asymptomatic acute abdomen exhibited a longer duration of diabetes compared with those reporting abdominal pain (12.5 years [10.5–14.5]vs. 8.8 years [5.0–11.0], p<0.01). Similarly, HbA1c lev- els at ward admission were higher among asymptomatic patients than among those with symptomatic presentation (8.2% [7.2–8.7] vs. 7.5% [6.8–7.6], p=0.02). These box-plots illustrate unadjusted distributions and highlight vari-ability and overlap between groups; therefore, they should be interpreted as descriptive representations rather than evi-dence of dose–response or causal relationships.
Discussion
In this cross-sectional analysis, approximately one-third of elderly patients with acute abdominal conditions presented without abdominal pain. This prevalence aligns with previ-ous reports describing atypical presentations in 20–35% of older adults [8–10, 26].
The key finding of our study is the association between T2DM and pain absence. Nearly half of diabetic patients were asymptomatic, compared with only one quarter of non-diabetic individuals. This observation supports previ-ous evidence of altered nociception in diabetes [12–14]. However, given the retrospective observational design, these findings should be interpreted as associative rather than causal. The study identifies clinical variables associ-ated with asymptomatic presentation but does not allow inference on underlying mechanisms.
From a pathophysiological perspective, long-standing and poorly controlled diabetes has been associated with altered visceral pain perception through metabolic and neu-rovascular mechanisms, including chronic hyperglycemia-related nerve damage and autonomic dysfunction [27–30]. Although our study did not directly assess neuropathy, dia-betes duration and HbA1c represent clinically meaningful proxies of cumulative metabolic burden. In this context, the association between higher HbA1c levels, longer dis-ease duration, and absent abdominal pain observed in our subgroup analysis supports the biological plausibility of blunted visceral nociception in diabetic patients, without allowing mechanistic inference [31–33].
Beyond peripheral diabetic neuropathy, altered pain per-ception in older adults has been described in association with changes in central pain processing and age‑related modifi-cations in nociceptive integration. Recent studies in geriat-ric populations have highlighted age-associated changes in pain thresholds and functional connectivity of pain modula-tory networks, which may contribute to atypical or blunted symptom presentation in older individuals [34–36]. It is known that unfavorable metabolic conditions may lead to an increased mortality in patients admitted to acute care wards [37]. Clinically, the absence of abdominal pain should not provide reassurance in elderly patients with dia- betes. A high index of suspicion is warranted, and diagnostic strategies should emphasize early imaging and laboratory evaluation in this high-risk group [20, 38, 39]. Moreover, careful consideration of pharmacologic profiles is war-ranted, since medications influencing volume status or auto-nomic tone, may further alter hemodynamic responses and symptom perception in elderly diabetic patients [40]. Incor-porating patients’ glycemic control and diabetes history into the initial assessment might facilitate timely recognition of atypical cases and prevent diagnostic delay.
Our findings also have implications for surgical decision-making. Previous studies have reported poorer outcomes and higher mortality among elderly individuals undergo-ing emergency surgery for abdominal conditions [18, 41]. Frailty, multimorbidity, and atypical presentations contrib-ute to these adverse outcomes [5, 42]. Heightened aware-ness of AAA, particularly in diabetic patients, may improve triage, expedite intervention, and ultimately enhance
The observed relationship between lower heart rate and absent pain perception likely reflects underlying autonomic dysfunction. In elderly patients, especially those with long-standing diabetes, autonomic neuropathy can blunt sympa-thetic activation and attenuate the chronotropic response to nociceptive stimuli. Aging itself further diminishes barore-flex sensitivity and cardiovascular reactivity, thereby con-tributing to clinically silent presentations [41].
Similarly, the lack of fever as an independent predic-tor of AAA may be explained by immune-senescence and blunted inflammatory responses in older adult [4, 41]. Elderly patients often exhibit impaired cytokine release and attenuated febrile reactions to infection or inflammation. Moreover, chronic comorbidities such as diabetes and car-diovascular disease can further suppress systemic inflam-matory activation, meaning that the absence of fever does not exclude serious intra-abdominal pathology in this popu-lation [1, 4].
It is important to underline that these associations should be interpreted at an associative level, acknowledging that peripheral neuropathy, autonomic dysfunction, and altera-tions in central pain processing and age-related nociceptive integration may all contribute to blunted visceral pain per-ception in older adults.
While the association between diabetes and atypical abdominal symptoms has been previously described, our study adds value by highlighting the potential roles of dia-betes duration and glycaemic control. Other strengths of this study comprise the inclusion of multiple acute abdominal diagnoses, and the accurate metabolic characterization of the studied patients.
Nevertheless, several limitations should be acknowl-edged. An important limitation of this study concerns the definition of asymptomatic acute abdomen, which was based exclusively on triage documentation reporting the absence of abdominal pain. No standardized pain assess-ment scale was systematically applied, and information on cognitive status, delirium, dementia, or communica-tion impairments was not available. In an elderly popula-tion, these factors may substantially affect pain reporting and introduce a risk of misclassification bias, potentially
leading to underestimation or misclassification of symp-tomatic presentations. Consequently, this limitation restricts the internal validity of the study and should be considered when interpreting the observed associations. Furthermore, all participants were Caucasian, which restricts the appli-cability of our findings to ethnically diverse populations.
Finally, several potentially relevant confounders could not be included in the multivariable analysis, including the use of beta-blockers or other chronotropic drugs, presence of diabetic neuropathy or autonomic dysfunction, frailty indi-ces, and opioid or analgesic use prior to admission. The absence of these variables may have influenced the observed associations, particularly those involving heart rate and pain perception, and represents a limitation of the study.
In conclusion, asymptomatic acute abdomen represents a common clinical presentation among elderly patients admitted to hospital wards. Among elderly individuals with T2DM, asymptomatic presentation was more frequently observed in association with longer disease duration and higher HbA1c levels. These findings identify a clinically relevant association that may assist in recognizing patients at increased risk of delayed diagnosis. Given the retrospec-tive observational design, causal relationships and underly-ing mechanisms cannot be inferred and should be explored in future prospective studies.
Author contributions Conceptualization: Andrea Tumminia, Raffaella Romano, Francesco Galeano, Roberto Baratta, Filippo Luca Fimog-nari and Marcello Romano. Methodology: Andrea Tumminia, Raffa-ella Romano, Francesco Galeano, Luigi Piazza, Filippo Luca Fimog-nari, Roberto Baratta and Marcello Romano. Investigation: Andrea Tumminia, Raffaella Romano, Antonino Di Pino, Maurizio Di Marco, Luigi Piazza, Maria Carolina Picardo, Paola Magnano San Lio and Marcello Romano. Resources: Andrea Tumminia, Raffaella Romano, Francesco Frasca, Lucia Frittitta and Marcello Romano. Writing and original draft preparation: Andrea Tumminia, Raffaella Romano, Fran-cesco Frasca, Francesco Galeano, Vittorio Oteri, Alessia Longo, Lu-cia Frittitta, Rosario Le Moli, Tommaso Piticchio, Antonino Di Pino, Maurizio Di Marco, Luigi Piazza, Maria Carolina Picardo, Paola Mag-nano San Lio, Filippo Luca Fimognari and Marcello Romano. All au-thors have read and agreed to the published version of the manuscript.
Funding Open access funding provided by Università degli Studi di Catania within the CRUI-CARE Agreement. The study was performed without any funding
Declarations
Conflict of interest The authors have no conflict of interest to declare regarding this study.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.o rg/licenses/by/4.0/.
This article is excerpted from the 《Acta Diabetologica》 by Wound World.

