Most of you, if not all, will be aware of the ancient use of silver, dating back to the ancient Egyptians. Centuries BC, silver was used to purify water and reduce wound infections. In the middle ages, silver nitrate was used to cauterise wounds, much as we use it to shrink hypergranulation tissue today. As the awareness of postoperative infections rose, silver wire was sometimes used to close wounds. In the 20th century, colloidal silver, a liquid suspension of microscopic silver particles, was used as a disinfectant and was also used as an intravenous treatment of infection before the development of antibiotics. It has also been taken as an health supplement and as nose drops.
Recently, I have attended multiple meetings regarding diabetic foot management where the question has arisen ‘when should we start adjunctive or advanced treatment options?’. For the purposes of this discussion, adjunctive or advanced therapies include active modalities such as collagen, topical oxygen therapy, or leukopatch, as opposed to ‘advanced dressings’, such as a foam and hydrofibre, which are used to manage wound symptoms such as exudate or bioburden as part of standard of care. The conclusion here was that, if at four weeks there was not a 50% area reduction of the wound at this point, we started to discuss following the ‘four-week rule (or guidance)’.
What is the ‘four-week rule’?
Studies from the literature have suggested for some time that, if the foot wound area has not been reduced by 50% following four weeks of standard of care treatment — infection control, optimise perfusion, pressure offloading, local wound care ([IWGDF, 2023) — then the wound is unlikely to heal by 12 weeks. This is based on the study by Sheenan et al (2003), who measured wound area in 203 patients at baseline and again after four weeks. Subjects with a reduction in ulcer area greater than the four-week median had a 12-week healing rate of 58%, whereas those with reduction in ulcer area less than the four-week median had a healing rate of only 9% (p<0.01). The absolute change in ulcer area at four weeks was significantly greater in healers versus non-healers. (Warriner, 2011)
What is the rationale for the use of the ‘four-week rule’?
As Sheenan et al (2003) described, ‘The percent change in foot ulcer area after four weeks of observation is a robust predictor of healing at 12 weeks. This simple tool may serve as a pivotal clinical decision point in the care of diabetic foot ulcers (DFU) for early identification of patients who may not respond to standard care and may need additional treatment’.
The literature suggests that around 60% of DFUs meet the criteria of 50% area reduction in four weeks, meaning around 40% of DFU are on a non-healing trajectory and will be hard to-heal. This ‘four-week’ rule has been used in many algorithms as a ‘tipping point’ (Warriner et al, 2011) for the use of adjunctive therapies such as: topical oxygen therapy (Frykberg et al, 2023), collagen (Fletcher et al, 2020) and topical haemoglobin spray (Chadwick et al, (2015). Additionally, insurance companies in countries such as the US use the ‘four-week rule’ for wounds that do not achieve 50% healing as a threshold or decision point for when clinicians can move to adjunctive therapies. The IWGDF (2023), made a number of conditional supportive recommendations for the use of interventions to improve healing of DFU in people with diabetes. These include the use of sucrose octasulfate dressings, negative pressure wound therapies for postoperative wounds, placental-derived products, autologous leucocyte/platelet/fibrin patches, topical oxygen therapy and hyperbaric oxygen. In all cases, the IWGDF stressed that these advanced therapies should be used where best standard of care was not able to heal the wound alone, although no specific time frame was given with the latest guidance. The purpose of the four-week rule, therefore, is to reassess the patient’s healing at four weeks for the benefit of the patient and to establish the effectiveness of the current protocol.
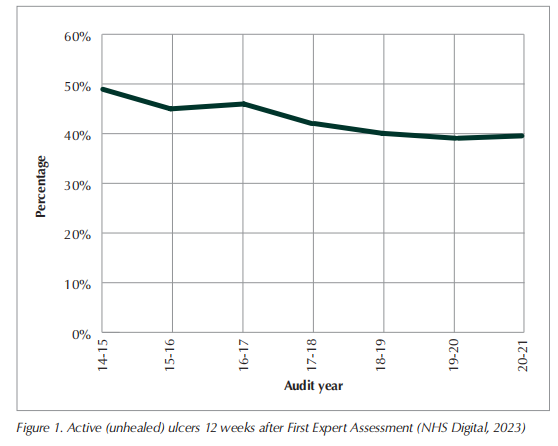
How are we doing in the UK? According to the work of Guest et al, not very well (2015; 2017; 2020). First, there appears to be a failure of adequate objective wound measurement. Despite the advent of more accurate measurement systems into some clinics, many use a simple ruler to measure the longest and widest points, if they measure at all. The data appears to show that clinicians, if they are re-assessing wounds at four weeks and find no improvement, simply change the dressing regime without investigating the reason behind the nonhealing wound trajectory. Clearly, the wound should be reassessed to ensure optimal healing potential. If care has been fully optimised, adjunctive therapy should be considered as opposed to simply applying different dressing technology. Recent National Diabetic Foot audit data (NHS Digital, 2023) in the UK has shown that while there has been a decrease in the number of unhealed ulcers at week 12, the number remains stubbornly above 40% (Figure 1). Despite expert assessment at first presentation and treatment of the DFU with what would be perceived as good standard of care, there still remains a significant proportion of unhealed DFU at 12 weeks.
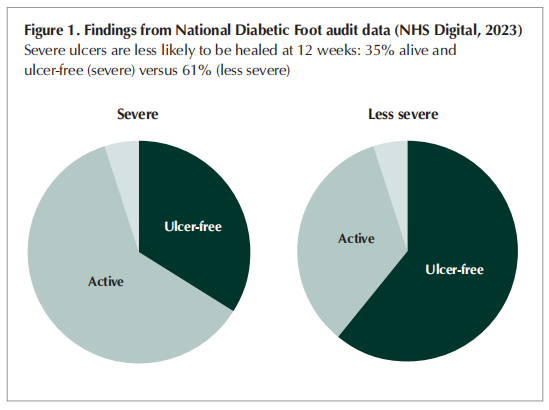
Second, of the more severe ulcers, 61% are unhealed at 12 weeks. Severity of ulceration is determined via the SINBAD score (Ince et al, 2008). The simple score based on these variables: Site, ischaemia, neuropathy, bacterial infection, and depth (SINBAD). This proves useful in predicting ulcer outcome and severity. SINBAD scores of 0–2 indicate a less severe ulcer, while a SINBAD score of 3 or more indicates a more severe ulcer.
Could this number of unhealed ulcers be reduced by embedding the four-week rule into all patient journeys? Employing the four-week rule could result in earlier identification of nonhealing DFU. This could have a significant impact on patient outcome, as wounds that remain open are at increased risk of infection, hospitalisation and possible amputation. Healing is a race against time, and longer wound duration brings increased healing challenges. This becomes even more significant in severe ulcers, as they are at much higher risk of infection and amputation if unhealed by 12 weeks (NHS digital, 2023).
A call to action
It’s clear to me from my personal discussions and the evidence in the literature that the answer to my initial question of ‘The four-week rule: are we letting our patients down?’ is YES. Time is NOT on the side of the DFU patient. While we objectively assess wounds, our patients deserve a sense of urgency in their care and a critical decisions in choices of when to apply more technology when they are not responding to the standard of care.
There are a number of minor changes that could make large differences when put into practice:
1. Measure wounds as accurately as possible. While the use of a simple ruler is not perfect, it does provide a threshold. Over time consider employing more accurate measurement systems.
2. Consider embedding the four-week rule into normal practice. At minimum, measure wounds on presentation and then again at 4 weeks.
3. A simple four-week check to check progress. This does not replace regular reviews and regular assessment, but instead acts as a formal progress point.
4. If the area of the wound has not reduced by 50 % at this four-week point, reassess all current treatments, and consider the use of adjunctive technologies.
Remember most changes are not ‘big bangs’ but a series of small incremental steps that add up to significant change. Make incremental progress, change comes by the centimetre not by the kilometre!
References
1. Chadwick P, McCardle J, Mohamud L et al (2015) Appropriate use of topical haemoglobin in chronic wound management: consensus recommendations. The Diabetic Foot Journal 18(3): 142–6
2. Fletcher J, Dhoonmoon L, Chadwick P et al (2020) Use of oxidised regenerated cellulose (ORC) and collagen dressings (PROMOGRAN Prote-ase Modulating Matrix and PROMOGRAN PRISMA Wound Balancing Matrix) to kickstart the treatment of chronic wounds. The Diabetic Foot Journal 23(1):62–9
3. Frykberg R, Andersen C, Chadwick P et al (2023) Use of topical oxygen therapy in wound healing. J Wound Care 32(S8B):S3– S30. https://doi.org/10.12968/jowc.2023.32.sup8b.s1
4. Guest JF, Ayoub N, McIlwraith T et al (2015) Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open 5:e009283. https://doi.org/10.1136/ bmjopen-2015-009283
5. Guest JF, Ayoub N, Mcilwraith T et al (2017) Health economic burden that different wound types impose on the UK’s National Health Service. Int Wound J 14(2):322–30. https:// doi.org/10.1111/iwj.12603
6. Guest JF, Fuller GW, Vowden P (2020) Cohort study evaluating the burden of wounds to the UK’s National Health Service in 2017/2018: update from 2012/2013. BMJ Open 10(12):e045253. https://doi.org/10.1136/bmjopen-2020-045253
7. Ince P , Abbas G, Lutale JK et al (2008) Use of the SINBAD classification system and score in comparing outcome of foot ulcer management on three continents. Diabetes Care 31(5):964–7. doi: 10.2337/dc07-2367
8. International Working Group on the Diabetic Foot (IWGDF 2023) Guidelines (2023 update) - IWGDF Guidelines
9. NHS Digital (2023) National Diabetes Foot Care Audit. https:// tinyurl.com/53ew9z4y
10. Sheenan P, Jones P et al (2003) Percent change in wound area of diabetic foot ulcers over a 4-week period is a robust predictor of complete healing in a 12-week prospective trail. Diabetes Care 26(6):1879–82 https://doi.org/10.2337/ diacare.26.6.1879
11. Warriner R, Snyder RJ, Cardinal MH et al (2011) Differentiating diabetic foot ulcers that are unlikely to heal by 12 weeks following achieving 50%percent area reduction at 4 weeks. Int Wound J 8(6):632–7. https://doi.org/10.1111/j.1742- 481x.2011.00860.x
This article is excerpted from the 《The Diabetic Foot Journal Vol 26 No 2 2023》 by Wound World.

