
Chronic wounds fail to progress through a typical, orderly, and timely repair sequence due to the underlying aetiology (Bowers and Franco, 2020). Chronic wounds are complicated and are categorised as diabetic foot ulcers (DFUs), vascular ulcers (venous and arterial ulcers) and pressure injuries (Nunan et al, 2014; Frykberg and Banks, 2015). Chronic wounds share specific characteristics like excessive levels of proinflammatory cytokines, matrix metalloproteinases, senescent cells and persistent infection (Frykberg and Banks, 2015). The prevalence of chronic wounds in India is estimated to be 4.5 per 1,000 people (Shukla et al, 2005).
DFUs are complications that can potentially lead to mortality (Khanolkar et al, 2008) and are estimated to remain the most frequent cause of hospitalisation and disability than other long-term diabetic complications. As 85% of lower-limb amputations are preceded by foot ulceration, appropriate management of foot lesions becomes highly important (Palumbo and Melton, 1985). According to one estimate, out of 77 million individuals with diabetes, 25% develop a DFU (Kale et al, 2023). According to national and international guidelines, people with diabetes should have a complete diabetic foot exam at least once a year (National Institute for Health and Care Excellence, 2015). However, surveys indicate that compliance with the standard recommendations of annual foot examinations in patients with diabetes at the primary care level is deficient (Mehndiratta et al, 2020). A systematic review by Jupiter et al (2016) reported a 5-year mortality rate of about 40% in DFU patients. A prospective study observed that 30% of patients present with Wagner Grade 3 DFUs (Muduli et al, 2015).
In a cross-sectional study, out of 1,674 newly diagnosed diabetes patients in India, 4.54% had DFUs (Sinharay et al, 2012). A community-based cross-sectional study of 620 diabetes patients in rural areas of Udupi district, India, reported a 51.8% prevalence of diabetic foot syndrome with advanced age, low socioeconomic status, longer duration of diabetes, and sedentary physical activity as the major risk factors (Vibha et al, 2018).
According to Cavanagh et al (2012), the economic burden for patients range from the equivalent of 6 days of average income for case 1 in the US (uncomplicated 4cm2 plantar ulcer of 6weeks’ duration, classified as PEDIS ([1/4cm2 /1/1/2]), Wagner grade 1, Texas grade 1, stage A) compared to 5.7 years of average annual income for case 2 in India (20 cm2 plantar ulcer of 6months’ duration, classified as PEDIS ([3/20cm2 /3/4/2]), Wagner grade 3, Texas stage D ulcer).
Kumpatla et al (2013) highlighted that patients with foot complications spend four times more than patients without any complications (INR19,020 versus INR4,493), and 81% of the out-of-pocket expenditures for hospital services consisted of personal savings (48%), loans and borrowing (14%), mortgages (8%) and sales of property (11%).
Venous ulcers are the most severe and debilitating outcome of chronic venous insufficiency in the lower limbs, accounting for 80% of lower-extremity ulcerations (O’Meara et al, 2014). Venous leg ulcers (VLUs) are open lesions between the knee and ankle joint (Nelson and Adderley, 2016). The major risk factors are older age, female gender, trauma, deep vein thrombosis and phlebitis (Scott et al, 1995; Abbade and Lastória, 2005; Etufugh and Phillips, 2007). In a tertiary care centre in eastern India, VLUs were predominant (34%) among the patients (n=100) with chronic leg ulcers, followed by arterial ulcer (14%), mixed arterial and venous ulcer (11%; Nag et al, 2020).
In an opinion survey conducted by Das et al (2020), it was identified that only 25.7% of the doctors performed comprehensive clinical examinations and utilised optimal preventive and therapeutic care methods for the management of diabetic foot in India. As DFUs and VLUs lead to long-term complications (Jupiter et al, 2016), adequate patient awareness of the existing treatment options remains necessary.
The present study was conducted among healthcare professionals (HCPs) and patients across India to understand the patient burden and profile of DFUs and VLUs, challenges experienced by the HCPs, and unmet needs in the treatment and management of chronic wounds.
Methods
Selection of HCPs and patients
This observational, cross-sectional survey was conducted in two phases. The first phase of the survey was conducted from June 2022 to July 2022 among HCPs, across India. The five specialities of the HCPs (diabetology, general surgery, podiatric surgery, plastic surgery and vascular surgery) were decided, considering the role of these specialists in the treatments of DFUs and VLUs. The sample was designed to cover more diabetologists and general surgeons, as there are fewer other specialities (plastic, podiatric and vascular surgeons) in India that treat DFU and VLU. Although the study’s intention was circulated among a larger group of doctors, the survey was conducted among 100 HCPs who showed interest in the initial questionnaire.
A total of 20 qualitative interviews were conducted via Microsoft Teams, and the remaining 80 responses were received from the digital survey. A survey link was shared with the doctors, and the responses were collected in the portal. The qualitative and survey responses were compiled and used for further analysis.
The study’s second phase was conducted during September–November 2022 with patients with DFUs and VLUs across India. Patients were selected randomly by the HCPs who participated in the survey.
Survey questionnaire
A pre-defined, structured and self-administered questionnaire assessed the chronic wound patient’s journey perception. Both open- and close-ended questions were included in the survey questionnaire across different categories [Supplementary Table 1]. The questions related to the referral pathway were surveyed only among the diabetologists and general surgeons.
Statistical analysis and ethical considerations
Descriptive statistics were used to present the responses of the HCPs and the patients. The distribution of the responses was presented as numbers and proportions. A graphical presentation was used to depict the survey results, as appropriate. The survey was conducted following the protocol and principles of the Declaration of Helsinki. De-identified and aggregated survey results were analysed to maintain the anonymity of HCPs. Written informed consent was obtained from the patients. Ethical approval was not sought for this non-interventional survey research.
Results
HCPs and patient profiles
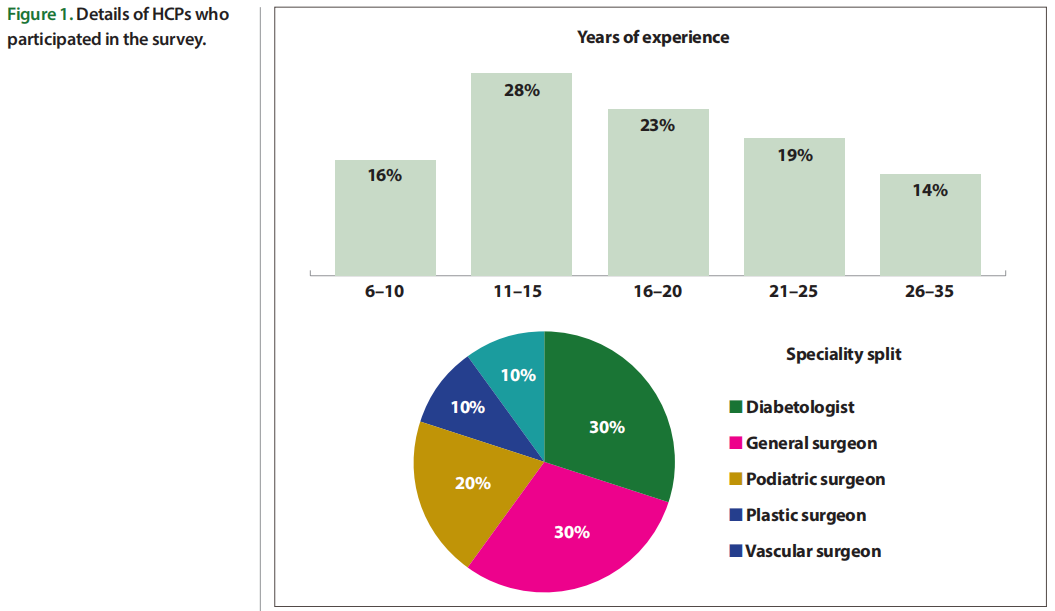
A total of 100 HCPs participated in the survey; most respondents were from south India (37%). Most were diabetologists and general surgeons, followed by podiatric surgeons[Figure 1].
A total of 25 DFU patients and five VLU patients participated in the survey; most respondents were from south India (74%) and 80% were men. About 83% of the patients had DFUs, and 17% had VLUs. Among the 25 DFU patients, 40% were >70 years, and 60% of the VLU patients were 40–50 years old.
Patient load and patient profile Characteristics of patients seen by HCPs
The average number of patients seen by the HCPs per month was 333, with the average number of patients with chronic wounds 64 (19%); DFU 41 (64%) and VLU 15 (23%). Most of the patients were direct walk-ins.
Profile of DFU patients
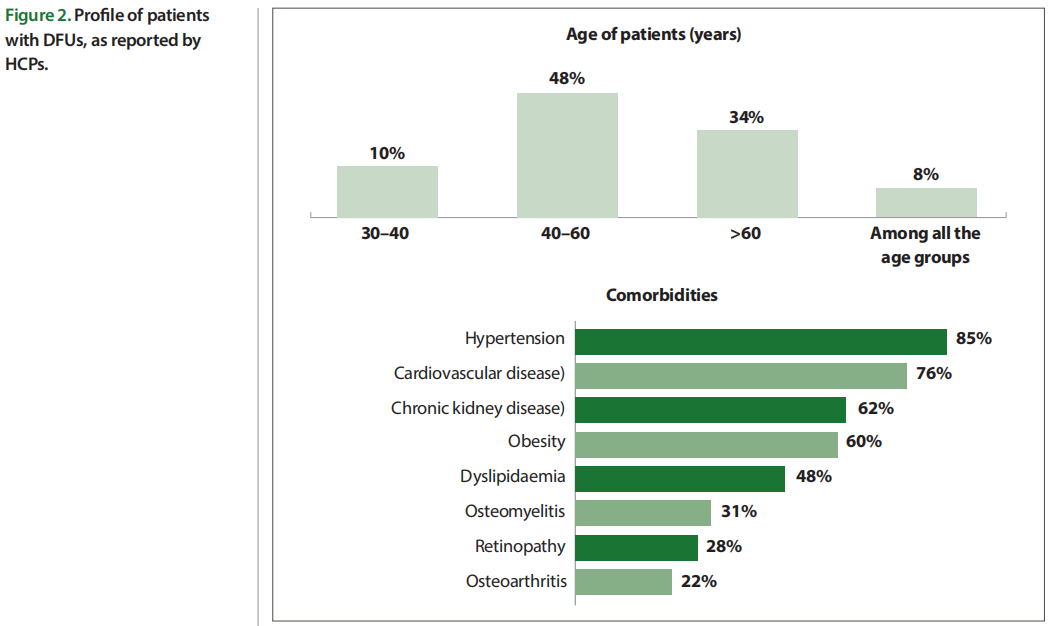
Among the DFUs seen by HCPs, 40% were new cases, while 60% were follow-up cases. The HCPs observed that 48% of the DFU patients were 40–60 years of age [Figure 2]. The three major comorbid conditions in DFU patients were hypertension (85%), cardiovascular disease (76%) and chronic kidney disease (62%) [Figure 2]. The top three problems seen in DFU patients and as reported by HCPs, were non-healing wounds (85%), infected wounds (76%) and discharge from the wound (65%).
Similarly, DFU patients who participated in the survey reported that infected wounds (72%), discharge from the wound (48%), pain (44%) and swollen feet (44%) were their top issues. It was observed that 32% of the DFU patients developed symptoms within 1–2 years, and 76% of the DFU patients visited doctors within 1 week of the presentation of the symptoms.
Profile of VLU patients
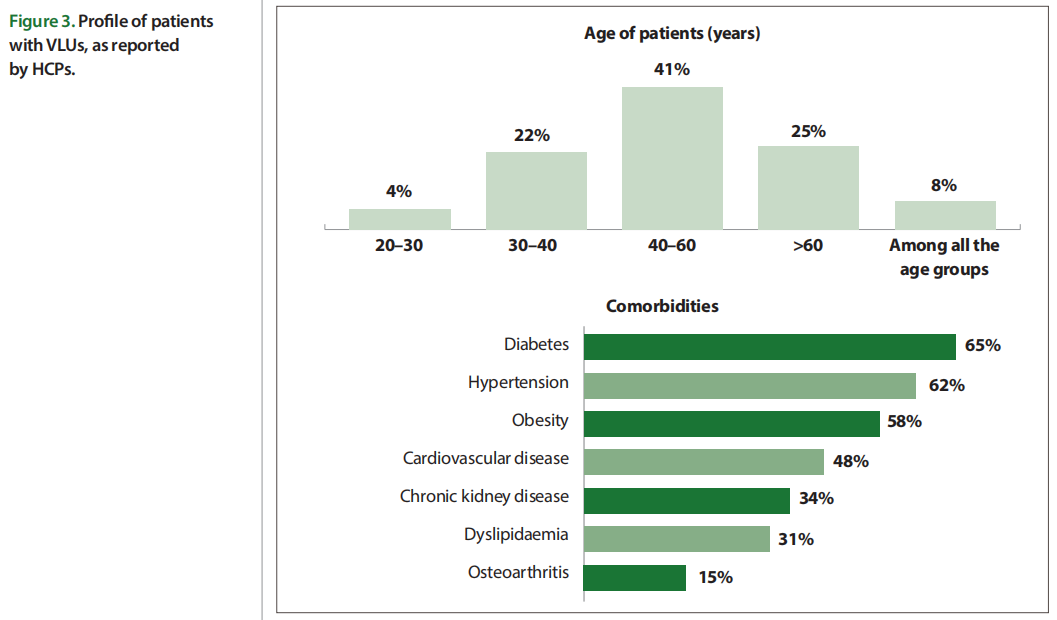
Among the VLU cases seen by the HCPs, 42% were new cases and 58% were follow-up cases. HCPs reported that 41% of VLU patients were 40–60 years of age [Figure 2]. The common comorbidities observed in VLU patients were diabetes (65%), hypertension (62%) and obesity (58%) [Figure 2]. It was observed that 81% of the patients had a history of varicose veins and 48% had deep vein thrombosis. The top three problems seen in VLU patients were non-healing wounds (72%), swelling/oedema (68%), and discolouration of the skin (66%). VLU patients in the survey reported that discharge from wounds (80%), pain (80%), and non-healing wound (60%) were their primary complaints.
About 40% of the VLU patients experienced symptoms for 3-6 months, and another 40% experienced them for 2-4 years. Nearly 80% of the VLU patients visited doctors within one week of symptom presentation, 60% visited the local doctors for the initial management of symptoms, and 40% followed home treatment.
Diagnosis of DFU and VLU
HCPs reported that the most common diagnostic tests recommended for DFU were arterial Doppler ultrasonography (88%) and X-ray (87%), while venous Doppler ultrasonography was mostly recommended for the diagnosis of VLU. Venography was mainly prescribed by vascular surgeons (60%), followed by diabetologists (53%) for the diagnosis of VLU.
The patients reported that the diagnostic tests recommended to them during primary treatment of DFUs were X-rays (56%), MRI (28%), and blood tests (17%), while for VLU diagnosis, X-rays were recommended. Only five HCPs mentioned DFUs to the patients and none of the HCPs mentioned VLUs to the patients.
Misdiagnosis
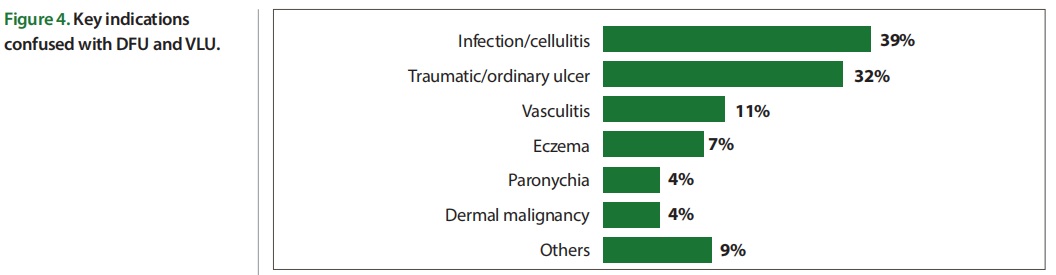
It was believed by 71% of the HCPs that there was a misdiagnosis of DFUs and VLUs at the primary care level. Furthermore, 93% of respondents believed that misdiagnosis led to a delay in the diagnosis of DFUs and VLUs. The time lapse between the appearance of symptoms and the correct diagnosis was 5 weeks. DFU and VLU were commonly misdiagnosed as regular infections or wounds by physicians at the primary level [Figure 4].
The patients reported that diabetologists and orthopaedic surgeons made the correct diagnosis of DFU. However, only 40% of general physicians could diagnose DFUs correctly. Almost 60% of the general physicians misdiagnosed VLUs as regular wounds/bacterial infections and only 20% of the general physicians could correctly diagnose VLUs.
To reduce misdiagnosis, measures that need to be initiated by the HCPs include seeking medical opinion and investigation for timely diagnosis (57%) and conducting a Doppler study early in the examination (6%). The measures that are expected from the pharmaceutical companies include creating awareness among HCPs and patients (54%), training physicians in primary wound care (6%), and organising continuous medical education (6%). Apart from misdiagnosis, the other factors that were responsible for delayed diagnosis of DFU and VLU include lack of awareness among HCPs and patients (55%), patient resistance (48%), unaffordability (22%) and delayed reference (22%).
Referral pathway
The deciding factors for diabetologists and general surgeons to treat on their own include a mild or early form of the disease (58%), the clinical status of the patient (47%), and no/ less comorbidity (38%). Diabetologists and general surgeons treated 75% of DFU and 61% of VLU cases, and 25% of DFU and 39% of VLU cases were referred to other specialities. The primary factors considered for the referral pathway include advanced/severe cases (97%), unavailability of advanced diagnostic tools (70%), and the presence of other comorbidities (35%). The patients reported that they were referred to specialists by their primary HCPs.
Stages of DFU and VLU of referred patients
HCPs reported that most DFU patients were referred with ulcerated (stage 3) or infected feet (stage 4). Patients with necrotic feet (stage 5) were referred to plastic surgeons. VLU patients who had discharge from wounds or visible wounds were considered for reference. General surgeons were referred for skin discolouration and itching (stage 3). Similarly, patients reported the progression of wounds/infections before they visited the specialists.
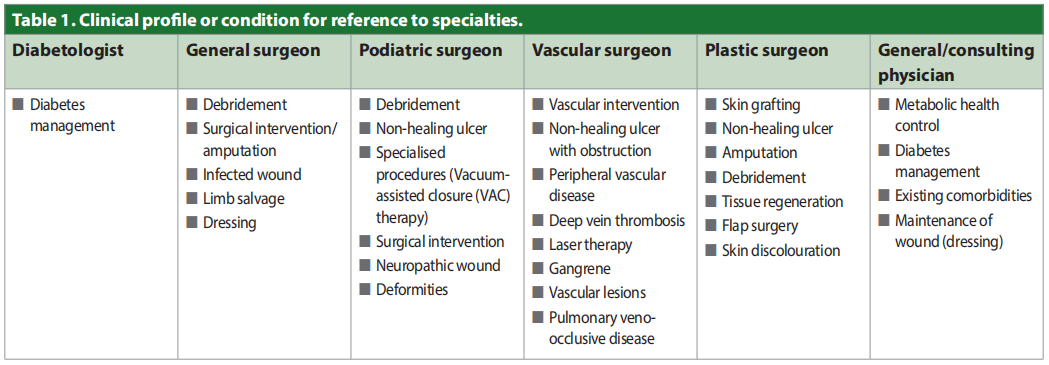
Clinical profile or condition in which reference was made to specialities
Patients were usually referred to other specialities for existing health issues and management of wounds [Table 1].
Treatment approach
Treatment guidelines
For the management and treatment of DFU and VLU, 57% of the HCPs followed the Diabetic Foot Society of India guidelines, and 53% followed the hospital protocol {Supplementary Table 2].
Treatment preferences
Dressings and drugs were the standard therapies offered to DFU patients. Offloading was practised more by podiatric surgeons (58%) and debridement by plastic surgeons (61%). The standard therapies offered to VLU patients were dressing and compression. Leg elevation was practised more among general (71%) and plastic surgeons (73%).
Preferred mode of treatment for DFU and VLU
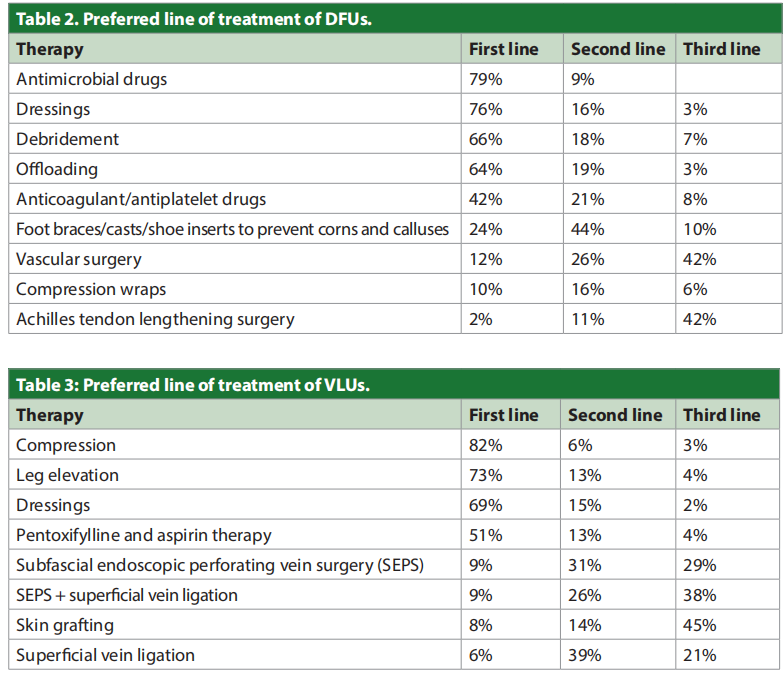
The preferred first line of therapy for DFU was antimicrobial therapy, dressings, debridement, and offloading; for VLU, it was compression, leg elevation, and dressings [Tables 2 and 3].
The patients reported that the primary treatment recommended for DFUs were dressing (56%), surgery (amputation; 48%) and medication (48%). For VLU, the treatment included antibiotic therapy (80%), dressing (40%) and compression (20%).
Choice of treatment and patient adherence
HCPs reported that the choice of treatment depended on the severity of the wound (91%), the presence of comorbidities (85%), and the cost of therapy (84%). The primary factors influencing patient compliance included socioeconomic (literacy, affordability; 86%), patient-related understanding of disease (79%), and disease conditions (symptoms/severity; 77%).
The average treatment duration for DFUs and VLUs was 9 weeks and 11 weeks, respectively. The patients reported similar timelines (DFUs <3 months, VLUs <3 months). The average patient dropout percentage for DFUs and VLUs was 26% and 30%, respectively (the duration for patients to drop out from treatment was 4weeks). Some of the factors leading to patient dropout included the long duration of treatment (74%), high cost of treatment (71%) and poor understanding of the disease (71%).
Challenges and measures
The primary challenges faced by HCPs included less awareness among patients (89%), nonadherence to treatment duration (72%), and delayed treatment (65%). The challenges faced by patients and caregivers included the high cost of treatment (82%), poor knowledge and understanding of the disease, and prolonged treatment (71%). A total of 39% of HCPs offered concessions on the total treatment cost and counselled the patients on the importance of resting, taking medicine as prescribed and dressing changes. Patients felt that awareness and affordable treatment options would make the treatment more accessible.
DFU patients reported that the treatment and wound care that were suggested to them at home were cleaning wounds (48%), offloading shoes (44%) and less walking (40%), while VLU patients reported less walking (60%), oil massage (40%) and keeping the dressing dry (40%). In 32% of the DFU patients, there was a recurrence of wounds due to patients’ lack of knowledge, uncontrolled diabetes and poor blood circulation. Almost 40% of the VLU patients experienced recurrence due to lack of knowledge and improper compression stocking.
To overcome the unmet needs, participating HCPs insisted on employing measuressuch as focusing on patient education (66%), increasing the availability of cost-effective products and drugs (55%), and increasing the availability of medication (14%). According to 55% of the participating HCPs, the need for cost-effective and fast-healing products remained the commonest measure that requires immediate attention.
Discussion
The current survey analysed how HCPs and patients perceive chronic wounds. The misdiagnosis of the disease, delayed referrals, high treatment cost, and accessibility to healthcare centres were identified as primary barriers to managing chronic wounds in Indian settings.
In our study, HCPs reported that 48% of DFU patients were 40–60 years of age. Our findings contradict the findings of a single-centre study from India (Muduli et al, 2015), which reported 54% of DFU patients aged 51–70 years. HCPs participated in this survey reported that most of the DFU patients were referred with stage 3 or infected feet. Similarly, Muduli et al (2015) reported that 30% of patients presented with Wagner grade 3 DFU. Only eight DFU patients presented to the clinic within 5days of the onset of symptoms, and 66% of the patients presented after one month from the onset of symptoms. However, in this study, 76% of the patients visited the local doctors within 1week of symptom presentation.
In the current study, 93% of HCPs believed that misdiagnosis led to a delay in the diagnosis of DFU. Lack of awareness among HCPs and patients was a prime factor for the delay in the diagnosis of DFU and VLU. Similarly, in an Indian study (Muduli et al, 2015), it was identified that lack of awareness about diabetes, poor treatment compliance, delay in diagnosis and late presentation to tertiary care centres were the factors that led to the occurrence of DFU at an earlier age.
In the present study, HCPs reported that drugs and dressings were the preferred first line of therapies for DFU, and one of the crucial factors for reference of DFU was the unavailability of advanced diagnostic tools. In a systematic review conducted by Musuuza et al (2020), it was identified that initiation of a multidisciplinary team care model for DFU resulted in a reduction in major amputations in 94% (31 of 33) of studies. Early effective treatment can reduce complications like amputations and mortality and improve the quality of life of DFU patients (Yazdanpanah et al, 2015).
Among the VLU patients of this study, 41% of the patients belonged to the 40-60 age group category. Similarly, in a prospective, multicentre, cross-sectional study, almost half of the patients were aged between 50 and 70 years (Rai et al, 2018).
In the current survey, compression was the first line of therapy for VLUs. A survey conducted among UK healthcare professionals showed that 40% would omit or reduce compression therapy as a pain management strategy for VLU (Atkin and Martin, 2020). Another survey identified that registered nurses who treat patients with VLUs used a variety of compression systems (Oates and Adderley, 2019).
The recommendations derived from the current survey can help reduce the overall health burden. Conducting frequent counselling sessions with the patients can help reduce their reluctance, improve timely diagnosis and aid in managing comorbidities. Although several wound care products are available, the need for adapted and fast healing products remains inevitable for the management of chronic wounds. Also, early treatment initiation can help faster wound healing with lower treatment costs.
Conclusion
This study sheds light on the challenges faced by healthcare professionals and patients in the management of chronic wounds in India. The high treatment cost and limited accessibility to healthcare centres emerge as major obstacles. Early diagnosis and referral are crucial in preventing misdiagnosis and improving patient outcomes. HCPs’ adherence to treatment guidelines and patient education are pivotal in successful wound management. Addressing unmet needs through cost-effective and fast-healing products can improve patient compliance. By focusing on awareness, affordability and timely interventions, clinicians can enhance the chronic wound patient’s journey, reduce the burden and promote better wound healing outcomes in India.
Acknowledgments
Medical writing support in the development of this paper was provided by THB c/o Sekhmet Technologies Pvt. Ltd., Gurugram, Haryana, India.
Declaration of interest
All authors have no conflicts of interest to report for this work.
References
1. Abbade LP, Lastória S (2005) Venous ulcer: epidemiology, physiopathology, diagnosis and treatment. Int J Dermatol 44(6): 449–56
2. Atkin L, Martin R (2020) An audience survey of practice relating to pain in the management of chronic venous leg ulcers. Br J Community Nurs 25(Sup12): S20–4
3. Bowers S, Franco E (2020) Chronic wounds: evaluation and management. Am Fam Physician 101(3): 159–66
4. Cavanagh P, Attinger C, Abbas Z et al (2012) Cost of treating diabetic foot ulcers in five different countries. Diabetes Metab Res Rev 28(Suppl 1): 107–11
5. Das A, Pendsey S, Abhyankar M, Malabade R (2020) Management of diabetic foot in an Indian clinical setup: an opinion survey. Cureus 12(6): e8636
6. Etufugh CN, Phillips TJ (2007) Venous ulcers. Clin Dermatol 25(1): 121–30
7. Frykberg RG, Banks J (2015) Challenges in the treatment of chronic wounds. Adv Wound Care (New Rochelle) 4(9): 560–82
8. Jupiter DC, Thorud JC, Buckley CJ, Shibuya N (2016) The impact of foot ulceration and amputation on mortality in diabetic patients. I: From ulceration to death, a systematic review. Int Wound J 13(5): 892–903
9. Kale D, Karande G, Datkhile K (2023) Diabetic foot ulcer in India: aetiological trends and bacterial diversity. Indian J Endocrinol Metab 27(2): 107
10. Khanolkar MP, Bain SC, Stephens JW (2008) The diabetic foot. QJM 101(9): 685–95
11. Kumpatla S, Kothandan H, Tharkar S, Viswanathan V (2013) The costs of treating long-term diabetic complications in a developing country: a study from India. J Assoc Physicians India 61(2): 102–9
12. Mehndiratta A, Mishra SC, Bhandarkar P et al (2020) Increasing identification of foot at risk of complications in patients with diabetes: a quality improvement project in an urban primary health centre in India. BMJ Open Qual 9(3): e000893
13. Muduli IC, PP A, Panda C, Behera NC (2015) Diabetic foot ulcer complications and its management – a medical college-based descriptive study in Odisha, an eastern state of India. Indian J Surg 77(Suppl 2): 270-4
14. Musuuza J, Sutherland BL, Kurter S et al (2020) A systematic review of multidisciplinary teams to reduce major amputations for patients with diabetic foot ulcers. J Vasc Surg 71(4): 1433–6.e3
15. Nag F, Chatterjee G, Ghosh A, De A (2020) Clinicoetiological evaluation of chronic leg ulcer in a tertiary care center of eastern India. Indian J Dermatol 65(6): 49–9
16. National Institute for Health and Care Excellence (2015) diabetic foot problems: prevention and management. NICE, London
17. Nelson EA, Adderley U (2016) Venous leg ulcers. BMJ Clin Evid 2016: 1902
18. Nunan R, Harding KG, Martin P (2014) Clinical challenges of chronic wounds: searching for an optimal animal model to recapitulate their complexity. Dis Model Mech 7(11): 1205–13
19. O’Meara S, Al-Kurdi D, Ologun Y et al (2014) Antibiotics and antiseptics for venous leg ulcers. Cochrane Database Syst Rev 2014(1): CD003557
20. Oates A, Adderley U (2019) Survey of registered nurses’ selection of compression systems for the treatment of venous leg ulcers in the UK. J Tissue Viability 28(2): 115–9
21. Palumbo PJ, Melton LJ (1985) Peripheral vascular disease and diabetes. Diabetes in America 2: 401–8
22. Pankhurst CJW, Edmonds ME (2018) Barriers to foot care in patients with diabetes as identified by healthcare professionals. Diabet Med 35(8): 1072–7
23. Rai R, Shenoy MM, Viswanath V et al (2018) Contact sensitivity in patients with venous leg ulcer: A multicentric Indian study. Int Wound J 15(4): 618–22
24. Scott TE, LaMorte WW, Gorin DR, Menzoian JO (1995) Risk factors for chronic venous insufficiency: a dual casecontrol study. J Vasc Surg 22(5): 622–8
25. Shukla VK, Ansari MA, Gupta SK (2005) Wound healing research: a perspective from India. Int J Low Extreme Wouds 4(1): 7–8
26. Sinharay K, Paul UK, Bhattacharyya AK, Pal SK (2012) Prevalence of diabetic foot ulcers in newly diagnosed diabetes mellitus patients. J Indian Med Assoc 110(9): 608–11
27. Vibha SP, Kulkarni MM, Kirthinath Ballala AB et al (2018) Community based study to assess the prevalence of diabetic foot syndrome and associated risk factors among people with diabetes mellitus. BMC Endocr Disord 18(1): 43
28. Yazdanpanah L, Nasiri M, Adarvishi S (2015) Literature review on the management of diabetic foot ulcer. World J Diabetes 15;6(1): 37–53
This article is from the Wounds International 2023 | Vol 14 Issue 4 by Wound World.

