
Fatality rates from burn wound infection and sepsis have decreased with the advances in infection control measures for burn units and the application of topical antimicrobial agents (Revathi et al, 1998). However, infections remain one of the most common serious complications from burn injury, and approximately 75% of deaths related to burn injuries are associated with infection (Appelgren et al, 2002; Heggers et al, 2002; Norbury et al, 2016).
The incidence of beta-haemolytic Streptococcus in burn wounds varies (Bang et al, 1999). Streptococcus pyogenes has been associated with the most serious infections in burn patients, leading to severe cellulitis, sepsis and graft failure. Studies have confirmed that S pyogenes produces extracellular toxins, increasing the depth and severity of the burn wound. Its pathogenesis can be attributed to the cell membrane M-protein and capsule of this species, which inhibits phagocytosis through polymorphonuclear leucocytes (Moses et al, 1997). Surface structures, such as the M protein family, the capsule and a number of adhesion molecules (including fibronectin, vitronectin collagen-binding proteins and lipoteichoic acid) allow the microorganism to colonise the skin and mucus membranes (Bisno et al, 2003; Gillespie, 2004).
Burn wounds infected with S pyogenes may exhibit the clinical surgical scarlet fever, inflammatory infiltration boundary and excretion of thin pus. Although S pyogenes may not produce an intense systemic response after it infects the donor sites or burns wounds, it typically causes the grafts of those burn sites to slough off, leading to graft failure. Thus, superficial wounds in donor sites may become deep or cause full-thickness skin loss because of this infection. Most S pyogenes infections occur within a week after the burn injury, leading to the prescribing of penicillin G to patients in the early post-burn stages (Xiao and Xu, 2015). However, this is not recommended. While it may reduce burn wound infections, colonisation or both, it does not decrease mortality and may increase the risk of selecting resistant microorganisms such as methicillin‐resistant Staphylococcus aureus (MRSA; Avni et al, 2010; Barajas-Nava et al, 2013).
Using a topical antimicrobial agent is normal practice to treat burn wound infections and improve burn injury outcomes. The therapeutic management of burns involves cleansing, debridement and wound dressing (Cartotto, 2017). However, no consensusis has been reached about optimal antibiotics to control infection or improve wound healing (Wasiak et al, 2013; Norman et al, 2017).
Aim
Although silver sulfadiazine offers a broader antimicrobial spectrum than mupirocin and fusidic acid, few studies have explored its
This study aimed to evaluate the 1% silver sulfadiazine antimicrobial activity against S pyogenes and compare it with 2% mupirocin and 1% fusidic acid cream. antimicrobial action against S pyogenes.
Methods
Bacterial strains
We studied eight S pyogenes strains isolated from eight adult patients admitted to the Hospital Provincial de Rosario, Santa Fe, Argentina. The isolates were recovered from burn wounds of six patients, and from the blood culture of two patients and identified using the Vitek System (bioMérieux, La Balme Les Grottes, France). The bacterial isolates were recoveredin different periods (with a difference of 1 to 2 months), which allows the authors to assume that they are not epidemiologically related. The bacterial strains were stored at −70 °C in a preservative medium and subcultured one or two times on blood agar plates.
Topical antimicrobial agents
The topical agents evaluated were 1% silver sulfadiazine (Platsul-A, Soubeiran Chobet, Buenos Aires, Argentina), 2% mupirocin, and 1% fusidic acid.
Silver sulfadiazine is a combination of sodium sulfadiazine and silver nitrate, and it is the most commonly used topical antibiotic agent for both ambulatory and hospitalised burn patients. This agent is an excellent broad-spectrum antibacterial and has been shown to reduce the inflammatory response to burn injury, decrease bacterial colonisation, and provide a firm eschar for easier wound management (Church et al, 2006; Salvador Sanz et al, 2011).
Fusidic acid is a selective antibiotic that reaches a high antimicrobial concentration in the deep skin layers after topical application on both intact and damaged epidermis. It is available in several topical formulations (Bonamonte et al, 2014).
Mupirocin has potent inhibitory activity against S pyogenes, staphylococci, and MRSA. Although primarily marketed for nasal decontamination, mupirocin has increasingly been used as a topical agent in burn units (Church et al, 2006; Jagdale et al, 2020).
Susceptibility testing of topical antimicrobial agents
Susceptibility testing of topical antimicrobial agents was conducted using agar well diffusion (AWD) assays (Nathan et al, 1978). Agar plates were inoculated with the test organism and 6 mm wells were cut. The wells were filled with 250 μl of antimicrobial solutions, and all plates were incubated overnight at 35°C. The diameters of the clear zones around the antimicrobial-containing wells were measured after incubation. Results >8 mm indicate the susceptibility of the tested bacterial strain to antimicrobial agents.
Minimum bactericidal concentration
Topical antimicrobial agents with an inhibition diameter >8 mm were analysed to identify their antimicrobial activity against S pyogenes. First, each topical agent was diluted with Mueller Hinton broth (MHB), in a range of 0.0001% to 1% (v/v). Then, 1ml of an S pyogenes inoculum (106UFC/ml) was added to the MHB, and controls without antimicrobial agents were prepared. The samples were incubated and shaking at 37°C for 24 hours. Then, 1 ml of bacterial inoculum was harvested from the tubes and plated onto sheep blood agar (Clinical and Laboratory Standards Institute, 2020). Three independent assays determined minimum bactericidal concentration (MBC) values (that is, the lowest concentration at which the antimicrobial agent killed the bacterial inoculum (Levison, 2004).
Statistical analysis
The mean inhibition diameter and the mean MBC were determined for each strain and each antimicrobial agent. Student’s t-test was conducted to estimate the statistical differences between groups of strains. A P-value <0.001 was considered statistically significant.
Results
AWD assays
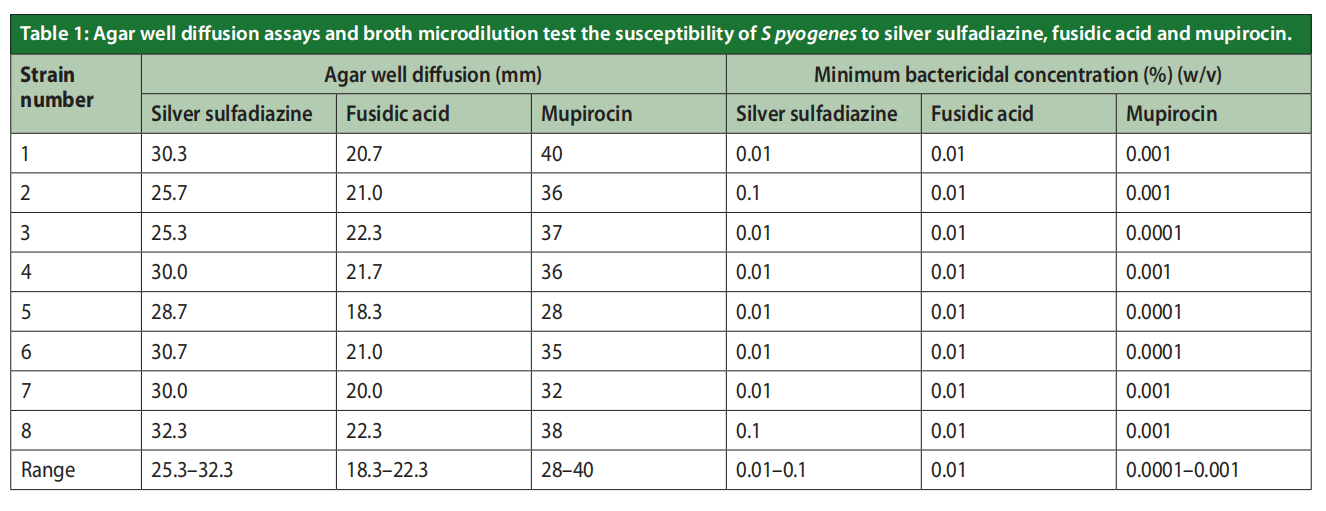
Eight S pyogenes isolates were obtained from clinical samples of eight patients. Table 1 and Figure 1 show the inhibition diameters obtained from the AWD assays for the eight strains. The results show that all tested S pyogenes isolates were susceptible to silver sulfadiazine (mean inhibition diameters: 25.3mm and 32.3mm), mupirocin (mean inhibition diameters: 28mm and 40mm), and fusidic acid (mean inhibition diameters: 18.3mm and 22.3mm). The inhibition diameters were significantly smaller (p<0.001) for fusidic acid.
MBC tests
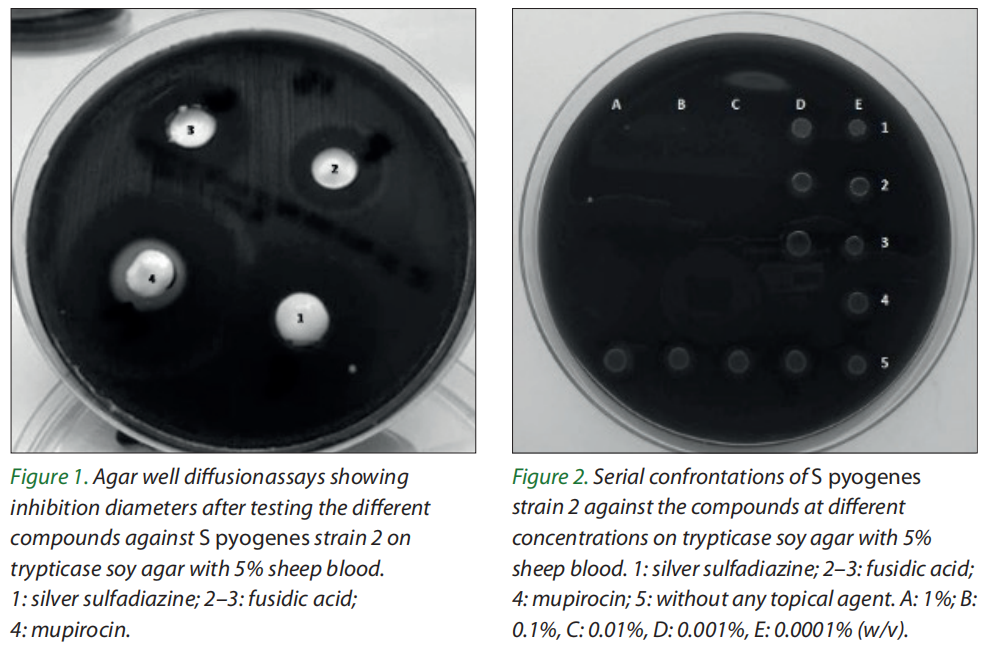
MBC ranged from 0.01 to 0.1% (w/v) for silver sulfadiazine, from 0.0001 to 0.001% (w/v) for mupirocin, and from 0.01 to 0.1% (w/v) for fusidic acid [Figure 2].
Discussion
Effective treatment with a topical antimicrobial reduces the microbial load on the open burn wound surface and reduces the risk of infection. The selected topical antimicrobial should inhibit microorganisms recovered from wound surveillance cultures of burn patients and infections acquired in hospital burn units. (Church et al, 2006). Nosocomial infections are caused by several microorganisms, so the antimicrobial agent with the broadest spectrum should be used against microorganisms (Glasser et al, 2010).
Fusidic acid has good in vitro activity against staphylococci, including both methicillinsensitive and -resistant strains, beta-hemolytic streptococci, and Corynebacterium spp. It is also effective against Gram-positive anaerobes, such as Clostridium difficile, Clostridium perfringens and Peptostreptococcus spp (Marian et al, 2020).
While the mupirocin spectrum of action includes Gram-positive bacteria and some Gramnegative bacteria (Khoshnood et al, 2019), neither mupirocin nor fusidic acid are effective against Pseudomonas aeruginosa, Enterobacteriaceae, and some anaerobes. Therefore, these antibiotics are not an option that should be considered in burn wounds, due to the high prevalence of P aeruginosa in burn units and increased bacterial resistance to these compounds (Foster, 2017). Considering its antimicrobial activity, silver sulfadiazine is a suitable alternative to treat S pyogenes infection.
This study evaluated the antimicrobial activity of 1% silver sulfadiazine against S pyogenes and compared it to 2% mupirocin and 1% fusidic acid creams, using AWD and MBC methods to confirm the inhibitory action of the three antimicrobial agents. While there are no defined cutoff values for inhibition diameters in AWD assays, we obtained precise, easy-to-read diameters for the topical agents. Although the antimicrobial agents’ complexity makes it difficult to standardise test conditions, we confirmed the inhibitory effect of three tested agents against S pyogenes. The results obtained with the MBC tests were consistent with the inhibition diameters observed with the AWD assays. Even though our tests confirm the presence of bactericidal activity in these agents, further pharmacodynamic and pharmacokinetic studies must be conducted to assess their clinical efficacy and antibacterial activity in vivo (Pankey and Sabath, 2004).
Many physicians prescribe fusidic acid to patients because it is a topical anti-infective choice with a low risk of contact sensitisation. In addition, its systematic use prevents bacteria from developing cross-resistance to other antibiotics. Fusidic acid is effective in vitro against S aureus, Staphylococcus epidermidis and S pyogenes.
Alsterholm et al (2010) tested the effect of fusidic acid on S pyogenes, with results of a 10 µg/ ml MIC for fusidic acid as part of a cream, a 6.25µg/ ml MIC for fusidic acid alone, and a 500µg/ml MIC for the entire cream. Leclercq et al (2000) reported that fusidic acid was moderately active against Streptococci after evaluating its effectiveness against 242 strains of Streptococci isolated from soft tissue and skin infections. They obtained MIC levels ranging from 8µg/ml to 16µg/ml, with only two strains displaying MICs for fusidic acid ≥64mg/l.
Nevertheless, the use of topical fusidic acid is firmly discouraged because of the spread of a fusidic acid-resistant clone of S aureus associated with impetigo (Simor et al, 2007; Elston, 2009; Shittu et al, 2009). Although mupirocin is effective against Gram-positive skin flora, such as S aureus (Dai et al, 2010), its effectiveness as an antimicrobial agent is diminished with the development of resistant strains (Hogue et al, 2010; Vázquez et al, 2019).
Our results show that silver sulfadiazine has similar efficacy against S pyogenes as mupirocin and fusidic acid. This topical antimicrobial inhibits the development of the major microorganisms responsible for wound and burns infections, such as S aureus, MRSA, S epidermidis, beta-hemolytic Streptococcus, P aeruginosa, Escherichia coli and other enterobacteria (Snelling et al, 1978; Koo et al, 1989; Nagesha et al, 1996; Palmieri and Greenhalgh, 2002; Olhan et al, 2005; Hussain and Ferguson, 2006; Casabonne et al, 2015). In addition, studies demonstrated the effectiveness of the antimicrobial activity of 1% silver sulfadiazine cream for decreasing colonisation rates in burn wounds (Heyneman et al, 2016; Norman et al, 2017). In many burn centres, silver sulfadiazine is the standard topical antibiotic used to treat burn wounds. Despite its widespread use, its efficacy against S pyogenes has not been properly researched. However, the susceptibility of S pyogenes to mupirocin and fusidic acid is well documented.
Conclusion
Our study demonstrated that silver sulfadiazine has remarkable antibacterial activity against S pyogenes. Due to its broad antimicrobial spectrum, silver sulfadiazine is a suitable alternative to control wounds and burn infections.
Conflicts of interest
The authors declare no conflict of interest.
Funding
This study was funded by Soubeiran Chobet S.R.L., Buenos Aires, Argentina.
References
1. Alsterholm M, Karami N, Faergemann J (2010) Antimicrobial activity of topical skin pharmaceuticals – an in vitro study. Acta Derm Venereol 90(3): 239–45
2. Appelgren P, Bjornhagen V, Bragderyd K et al (2002) A prospective study of infections in burn patients. Burns 28(1): 39–46
3. Avni T, Levcovich A, Ad-El DD et al (2010) Prophylactic antibiotics for burns patients: systematic review and meta analysis. BMJ 340: c241
4. Bang RL, Gang RK, Sanyal SC et al (1999) Beta-haemolytic Streptococcus infection in burns. Burns 25(3): 242–6
5. Barajas-Nava LA, López-Alcalde J, Roqué i Figuls M et al (2013) Antibiotic prophylaxis for preventing burn wound infection. Cochrane Database Syst Rev (6): CD008738
6. Bisno AL, Brito MO, Collins CM (2003) Molecular basis of group A streptococcal virulence. Lancet Infect Dis 3(4): 191–200
7. Bonamonte D, Belloni Fortina A, Neri L, Patrizi A (2014) Fusidic acid in skin infections and infected atopic eczema. G Ital Dermatol Venereol 149(4): 453–9
8. Church D, Elsayed S, Reid O et al (2006) Burn wound infections. Clin Microbiol Rev 19(2): 403–34
9. Cartotto R (2017) Topical antimicrobial agents for pediatric bums. Burns Trauma 5: 33
10. Casabonne C, Aquili V, González A, Balagué C (2015) In vitro activity of silver sulfadiazine against nosocomial methicillin-resistant Staphylococcus aureus isolates. Revista Argentina de Quemaduras 25(4): 6–10 [in Spanish]
11. Clinical and Laboratory Standards Institute (2020) Performance Standards for Antimicrobial Susceptibility Testing M100-S 30ed
12. Dai T, Huang YY, Sharma SK et al (2010) Topical antimicrobials for burn wound infections. Recent Pat Antiinfect Drug Discov 5(2): 124–51
13. Elston DM (2009) Topical antibiotics in dermatology: emerging patterns of resistance. Dermatol Clin 27(1): 25–31
14. Foster T (2017) Antibiotic resistance in Staphylococcus aureus. Current status and future prospects. FEMS Microbiol Rev 41(3): 430–49
15. Gillespie SH (2004) New tricks from an old dog: streptococcal necrotising soft-tissue infections. Lancet 363(9410): 672–3
16. Glasser JS, Guymon CH, Mende K et al (2010) Activity of topical antimicrobial agents against multidrug-resistant bacteria recovered from burn patients. Burns 36(8): 1172–84
17. Heggers JP, Hawkins H, Edgar P et al (2002) Treatment of infections in burns. In: Herndon DN, ed, Total Burn Care. Saunders, London: 120–69
18. Heyneman A, Hoeksema H, Vandekerckhove D et al (2016) The role of silver sulphadiazine in the conservative treatment of partial thickness burn wounds: a systematic review. Burns 42(7): 1377
19. Hogue JS, Buttke P, Braun LE, Fairchok MP (2010) Mupirocin resistance related to increasing mupirocin use in clinical isolates of methicillin-resistant Staphylococcus aureus in a pediatric population. J Clin Microbiol 48(7): 2599–600
20. Hussain S, Ferguson C (2006) Best evidence topic report. Silver sulfadiazine cream in burns. Emerg Med J 23(12): 929-32
21. Jagdale SC, Kothekar PV (2020) Development of emulgel delivery of mupirocin for treatment of skin infection. Recent Pat Antiinfect Drug Discov 15(2): 137–56
22. Khoshnood S, Heidary M, Asadi A et al (2019) A review on mechanism of action, resistance, synergism, and clinical implications of mupirocin against Staphylococcus aureus. Biomed Pharmacother 109: 1809–18
23. Koo DS, Zhen S, Zhen ZD (1989) Assessment of topical therapy of the burn wound with silver sulfadiazine after its use for 15 years in a burn unit. Burns 15(3): 193–6
24. Leclercq R, Bismuth R, Casin I et al (2000) In vitro activity of fusidic acid against streptococci isolated from skin and soft tissue infections. J Antimicrob Chemother 45(1): 27–9
25. Levison ME (2004) Pharmacodynamics of antimicrobial drugs. Infect Dis Clin North Am 18(3): 451–65
26. Marian E, Tita B, Duteanu N et al (2020) Antimicrobial activity of fusidic acid inclusion complexes. Int J Infect Dis 101: 65–73
27. McAdam AJ (2016) Essential microbiology for wound care. In: Edwards-Jones V (ed). Clinical Infectious Diseases. Oxford University Press, Oxford
28. Moses AE, Wessels MR, Zalcman K et al (1997) Relative contributions of hyaluronic acid capsule and M protein to virulence in a mucoid strain of the group A Streptococcus. Infect Inmunol 65(1): 64–71
29. Nagesha CN, Shenoy KJ, Chandrashekar MR (1996) Study of burn sepsis with special reference to Pseudomonas aeruginosa. J Indian Med Assoc 94(6): 230–3
30. Nathan P, Law EJ, Murphy DF, MacMillan BG (1978) A laboratory method for selection of topical. Burns 4(3): 177–87
31. Norman G, Christie J, Liu Z et al (2017) Antiseptics for burns. Cochrane Database Syst Rev (7): CD011821
32. Norbury W, Herndon DN, Tanksley J et al (2016) Infection in burns. Surg Infect 17(2): 250–5
33. Olhan Ragonha AC, Ferreira E, de Andrade D, Rossi LA (2005) Microbiological evaluation of 1% silver sulfadiazine dressings. Rev Lat Am Enfermagem13(4): 541–21 [in Portuguese]
34. Palmieri TL, Greenhalgh DG (2002) Topical treatment of pediatric patients with burns: a practical guide. Am J Clin Dermatol 3(8): 529–34
35. Pankey GA, Sabath LD (2004) Clinical relevance of bacteriostatic versus bactericidal mechanisms of action in the treatment of Gram-positive bacterial infections. Clin Infect Dis 38(6): 864–70
36. Revathi G, Puri J, Jain BK (1998) Bacteriology of burns. Burns 24(4): 347-49
37. Salvador Sanz JF, Novo Torres A, Lorda Barraguer E et al (2011) Comparative study on the effectiveness of a dressing of nanocrystalline silver opposite to the use of silver sulfadiazine in the treatment of burned patients. Cir Plást Iberolatinoam 37(3): 253–66 [in Spanish]
38. Shittu AO, Udo EE, Lin J (2009) Phenotypic and molecular characterization of Staphylococcus aureus isolates expressing low- and high-level mupirocin resistance in Nigeria and South Africa. BMC Infect Dis 9: 10
39. Simor AE, Stuart TL, Louie L et al (2007) Mupirocin-resistant, methicillin-resistant Staphylococcus aureus strains in Canadian hospitals. Antimicrob Agents Chemother 51(11): 3880–6
40. Snelling CF, Ronald AR, Waters WR et al (1978) Comparison of silver sulfadiazine and gentamicin for topical prophylaxis against burn wound sepsis. Can Med Assoc J 119(5): 466–70
41. Vázquez NM, Cáceres Guidó P, Fiorilli G, Moreno S (2019) Emerging mupirocin resistance in methicillin-resistant Staphylococcus aureus isolates at a tertiary care children’s hospital in Argentina. Arch Argent Pediatr 117(1): 48–55
42. Wasiak J, Cleland H, Campbell F, Spinks A (2013) Dressings for superficial and partial thickness burns. Cochrane Database Syst Rev (3): CD002106
43. Xiao G, Xu W (2015) Infections in burns. In: Yang Z (ed) Chinese Burn Surgery. Springer, Dordrecht: 57–87
This article is excerpted from the Wounds International 2022 | Vol 13 Issue 2 by Wound World.

