Foreword
There has been a great deal of debate around diabetic foot ulcers (DFUs) and pressure ulcers (PUs) on the feet of patients with diabetes, in terms of how to define, detect, assess and treat them. The confusion and lack of evidence in differentiating between these two types of foot ulcers, particularly on the heel, can lead to misdiagnosis, which can increase both financial and patient-related costs.
To address and tackle those inconsistencies, the Journal of Wound Care (JWC) has published its first international consensus document, Identifying and treating foot ulcers in patients with diabetes: saving feet, legs and lives. The main objectives of this project were to:
● Provide information on the differences between a DFU and a PU in patients with diabetes
● Help reduce misdiagnosis by providing and discussing assessment guidelines
● Make a difference in practice through improved patient outcomes.
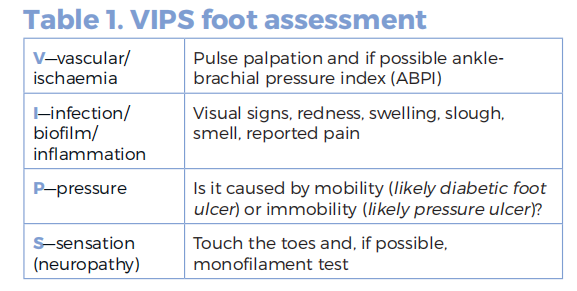
With this in mind, an international panel of ten key opinion leaders from Australia, England, Republic of Ireland, Malaysia, Poland, Portugal, Spain, United Arab Emirates and US met on 1 and 2 March 2018 in London. They discussed the definitions of a DFU and a PU, and concluded that one way to distinguish between them is knowing whether the patient is mobile (usually associated with DFUs) or immobile (normally related to PUs), although this should be considered along with simple assessments for ischaemia and neuropathy. To this end, and given the importance of an early and correct assessment, the mnemonic ‘VIPS’ was suggested:
● V: vascular (ischaemia)
● I: infection (local signs, odour, exudate, slough, inflammation, etc.)
● P: pressure (causes mobility or immobility)
● S: sensation (neuropathy).
The panel also agreed that another key point was that, if the health professional treating the ulcer is unable to perform a full diabetic foot assessment, it is crucial that the patient be referred to a health professional/ department who can. As many members of the professional team would usually come across an ulcer— job titles varying throughout the world—a referral pathway focusing on the referee’s skills rather than their specialties was suggested.
The importance of prevention and the need to follow clear management and treatment strategies, which will vary from centre to centre, were emphasised. The issues around education were also discussed, as well as future research needed. Finally, potential new technologies or alternative therapies that could help treat a DFU or a PU when standard care fails were summarised.
Given the international focus of this document, and the various levels of knowledge among the health professionals that come across a foot ulcer, it was highlighted that this document should be read and implemented in conjunction with the clinician’s local guidelines.
We hope you enjoy this document and that it helps make a difference in practice.
Camila Fronzo and Rachel Webb
Introduction
In developed countries, it has been estimated that the overall incidence of non-healing wounds is approximately 1–2%. 1 Pressure ulcers (PUs) and diabetic foot ulcers (DFUs) are amo ng the most prevalent chronic wounds in many countries.2,3 They are a major global clinical and health economic challenge, which is expected to escalate as the population increases, poor lifestyle leads to increased diabetes and obesity and the population ages.4–6
International expert consensus guidelines recommend, in general terms, similar pathways for the prevention and management of PUs and DFUs.7 Nevertheless, critical differences in the precise delivery of effective care lie within the guidelines, which, if not administered appropriately to the diagnosis, are likely to lead, at best, to slow healing. PUs and DFUs, despite describing clinically different indications, share commonalities in definition, for example, shear and friction, pressure and ischaemia.8 However, they require quite different approaches to management. These differences can lead to patients being managed on the wrong pathway.
This consensus paper addresses these similarities and differences with two key objectives: first, to differentiate between PUs and DFUs with regard to their definition, causes, assessment, diagnosis, management and treatment, and second, to address confusion and lack of evidence when differentiating PUs and DFUs.
Prevalence
Approximately 451 million adults worldwide have diabetes, a figure projected to increase to 693 million by 2045 globally.4 The prevalence of DFUs will also increase in line with this. The lifetime incidence of DFUs is reported to be 25%9 and the global prevalence of DFUs in patients with diabetes is 6.3%,10with wide variation by country.11–15 When PUs occur on the foot, those on the heel are the most common;16,17 the overall PU prevalence in five European countries in 2008 was 18.3%,16 while more than 2.5 million people in the US develop a PU annually,18 where the prevalence across all settings is 12.3%.16 More recent figures suggest the prevalence of PUs in Canada is 26% 19,20 and in Western Australia between 6.3% and 9.5%. 21
Issues around misdiagnosis
Differentiating between a heel wound that is a PU rather than a DFU presents a diagnostic challenge for clinicians. Furthermore, the prognosis, complications and treatment pathways/responsibility of care for PUs and DFUs are different. Risk factors for PUs include diabetes and perfusion,22–24 which should be considered in the formation of PU guidelines.7,25–27 Pressure is a common factor in the formation of both a PU on the foot and DFU, and both are managed in fundamentally the same way by reducing or redistributing the pressure.7,28 However, care pathways for PUs and DFUs are different, reflecting the specific characteristics of the wounds and skill sets required. It is critical to understand the patient clearly, to make an accurate diagnosis and to implement the management strategy appropriate to the wound, particularly where overlap in definitions exists.8 Among nurses caring for DFUs, around 35% may have only minimal knowledge of the diabetic foot.29 Furthermore, PUs and DFUs on the heel may be diagnosed differently, depending on the specialism of the health professional, leading to inappropriate care, particularly in the community setting.8,30 In countries such as the US, where payment for care depends on the identity assigned to the wound, the correct diagnosis may make the difference between receiving, or not, certain types of management and products. 31,32 For example, Apligraf for PU treatment is not even mentioned for reimbursement in the US.33
Cost of misdiagnosis
Incorrect diagnosis leading to an inappropriate care pathway will to lead to financial and patient-related cost. Management of PUs in all health-care systems is costly,34–38 and associated with higher mortality.39–40 Complications in the diabetic foot are among the most serious and costly in patients with diabetes. A third of the total cost of managing diabetes is attributable to DFUs, and these are significantly higher after ulceration compared with patients with diabetes and no foot ulcers.41 If not successfully treated, DFUs often lead to amputations, which involve lengthy stays in hospital.42 In fact, amputation in the diabetic foot is preceded by a DFU in approximately 80% of cases. 43 The cost of a DFU is high in all health-care systems34,44,45 and increases with severity. DFUs are widely recognised to have a major impact on patients’ quality of life (QoL)46,47 and impact on the wider family and friends. QoL is also adversely affected by PUs and any misdiagnosis is likely to exacerbate this.
It is clear that the costs of both PUs and DFUs are high and escalate with severity. Ensuring that the correct diagnosis is made and a care pathway, designed by appropriately-qualified and experienced health professionals, is followed, will help control patient related and health-care-related costs of PUs and DFUs, and provide the greatest probability of success in healing the ulcer and avoiding complications.
This is a working document that addresses general principles and provides guidance designed to minimise the likelihood of misdiagnosis and inappropriate management of PUs and DFUs. It should be read and implemented in conjunction with local guidelines. It brings theory and practice together, and offers areas of reflection that allow the reader to review the information and then decide where and how to use it to underpin their own clinical area. The consensus will inform and enable opportunities for practice change.
Differentiation between DFUs and PUs
Diabetic foot ulcers (DFUs) and pressure ulcers (PUs) have been defined in detail by a number of expert panels, consensus documents and 7,8,48,49 According to the International Working Group on the Diabetic Foot,49 a DFU is defined as:
‘A full-thickness wound below the ankle in a diabetic patient, irrespective of duration. Skin necrosis and gangrene are also included in the current system as ulcers.
The key elements are the location of the wound and the diagnosis of diabetes. The breadth of this definition means that a PU on the foot in a patient with diabetes is a DFU, as would be any foot wound in a patient with diabeted. 8 A DFU can occur on any part of the foot, including the plantar and dorsal surfaces. A DFU may be neuropathic, ischaemic or a combination of these two factors (known as neuroischaemic), but the three types of DFUs have overlapping pathophysiology.48
A PU is defined by the European Pressure Ulcer Advisory Panel (EPUAP), National Pressure Ulcer Advisory Panel (NPUAP), and Pan Pacific Pressure Injury Alliance (PPPIA) as (Box 1):7
‘A localised injury to the skin and or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear.’
The scope of this definition encompasses skin and tissue damage that results from pressure and/or shear and friction, irrespective of comorbidities. Nevertheless, there is scope for imprecision in the diagnosis and definition of a PU. The EPUAP definition warns us that:
‘A number of contributing or confounding factors are also associated with PUs; the significance of these factors is yet to be elucidated.’
This implies that merely diagnosing a wound as a PU does not necessarily fully describe the ulcer and therefore the care that it should receive. The definition of PU also encompasses those that occur at the end of life, related to Skin Changes at Life’s End or Kennedy Terminal Ulcers,49,50 and PUs that are caused by medical devices such as respirator masks, intubation, catheters, splints, casts, and compression bandaging.8,51
Where heel PUs and DFUs are concerned, there is clear room for overlap in their definitions, if not their precise underlying causes. The consensus panel recognises, in addition to other diagnostic features, that the degree of patient mobility could be a defining characteristic. PUs tend to be associated with immobility; DFUs tend to be associated with mobility. This is not an absolute differentiator. Where a heel PU is related to friction and shear, the patient may have been able to move, resulting in friction. This may be deliberate movement, where the patient tries to reposition themselves, pushing with their heels. However, movement may be passive, where the patient is moved manually by health professionals as part of care. For example, passive friction and shear may be caused by articulating bed frames, used widely in EU hospitals to assist in patient handling, while reducing risk of injury to staff. Involuntary sliding movement of the heel up to 15 or 20cm, which is recognised as a risk for heel injury, occurs when these bed frames are articulated.52 On the other hand, mobility/weight bearing is more prominent in the development of a DFU, where repeated friction and pressure on the foot, as the result of patient walking (ambulating), can cause the trauma component of ulceration.
From the viewpoint of management of the wound, and the patient on the appropriate pathway, the critical factor is accurate assessment and diagnosis, rather than the precise terminology used. Guidelines followed to achieve accurate assessment may be expert consensus guidelines, but they should be used in conjunction with local or national guidelines. The name ascribed to the ulcer is a start point; the factors that underlie the ulcer are the targets for management and must be clearly identified to develop an effective care plan.
Causes of PUs and DFUs
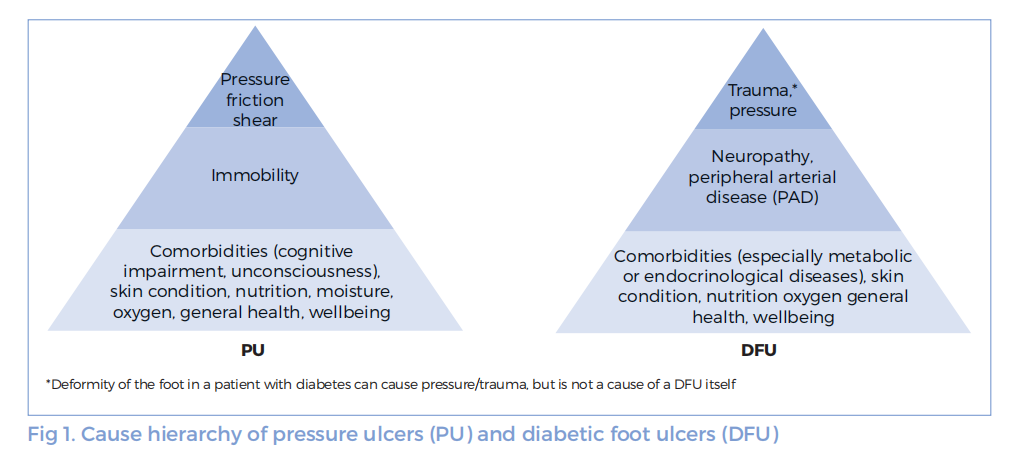
The pathophysiology of a DFU is complex and multifactorial (Fig 1). A patient with type 1 or type 2 diabetes may develop a number of underlying comorbidities that lead to an at-risk foot. At this stage, the foot does not have an active DFU, but is at high risk of forming one. Key factors in the risk of development of DFUs include:43,53
● Peripheral neuropathy, which reduces the ability to sense touch and pain and causes loss of protective sensation
● Foot deformity as a result of damage to the distal nervous system, which leads to small muscle wasting and muscle atrophy. The deformed foot (sometimes referred to as a Charcot deformity) is subject to increased pressure where bony prominences become more pronounced and the protective fat pads under the heels and metatarsal heads shift, exacerbating the harmful effects of pressure
● Autonomic neuropathy, causing loss of sweating that leads to dry skin and callus formation increases pressure locally, and the likelihood of the skin cracking. Autonomic neuropathy also causes increased peripheral blood flow and distended foot veins and a warm, dry foot. This can appear to be a healthy foot when, in fact, it is at risk
● Peripheral arterial disease (PAD) is present in nearly half of patients with diabetes,54 leading to reduced blood supply and tissue ischaemia. PAD is more common in type 2 diabetics than in type 155
● A history of previous DFU or amputation.
Older patients who have had diabetes for longer and male patients are at higher risk of DFU formation. When one or more of these underlying causes are overlaid with pressure and trauma from footwear or other sources, skin damage can lead to ulceration.56 Infection is not regarded as a cause of DFUs, but a consequence of it.43 Once an at-risk foot has skin damage, without the correct care, the wound can deteriorate rapidly as the tissue becomes hyperinflammatory, leading to the overexpression of powerful tissue-destructive proteinases and reactive oxygen species (ROS).57–59 Amputation in the diabetic foot is preceded by a DFU in approximately 80% of cases.43
The pathway to PU formation comprises three well documented key factors: pressure, friction and shear (Fig 1). A period of immobility is a fourth component. Patients may be bed-bound with comorbidities, elderly with end-stage conditions, immobile from spinal cord injury or during surgery. Moisture alone will not lead to PU formation,7 but in combination with pressure, and/or friction and shear, it is associated with ulcer formation. Shear is recognised by the NPUAP as a primary cause of PUs.60 Moisture increases friction between the skin and a surface, such as a bed sheet, 61 which causes tissue deformation when the different layers of skin move tangentially relative to each other as the patient moves. These forces may damage tissue directly62 or cause injury to superficial skin structures when a patient moves on a bed surface.63 Friction and shear predict the development of PUs in adult critical care patients.64 Tissue shear forces may cause cell damage and death more rapidly, over a period of minutes, than pressure alone.65 Pressure over bony prominences in an immobile patient directly damages deep tissue by compression and restriction of blood flow, leading to tissue death and ulceration. In contrast to shear forces, pressure acts over longer time periods, measured in hours.66 Pressure over bony prominences may be three to five times higher than other tissues, and this is doubled by shear forces.67,68 Pressure over bony prominences does not occur in isolation from shear forces and as tissue is deformed by compression, shear forces also form around the deformation. As with DFUs, the physical aetiology of PUs leads to uncontrolled expression of tissue destructive hyperinflammation that breaks tissue down, resulting in ulceration.57–59
Risk factors for the development of heel PUs69 include: a previous or current heel PU, indicative of reduced tissue tolerance; diabetes and peripheral neuropathy; stroke or cerebrovascular accident (CVA), restricting the patient’s ability to move; paralysis; hip fracture and dragging injuries resulting from knee replacements; dementia and cognitive impairment; PAD reducing tolerance to mechanical forces; leg spasms, Parkinson’s disease or tremors causing heel rubbing; agitated heels; leg oedema, which may compromise capillary flow and reduce tissue tolerance; and frequent sliding on the bed or chair. Also at risk of developing a PU are patients with diabetes, those undergoing surgical procedures longer than two hours, 24 those admitted to a nursing home after transfer from hospital compared with transfer from the community,23 patients at the end of life 22 and those using a medical device.70–72
Summary
There are similarities as well as important differences between a PU on the heel and a DFU.8 The risk and causative factors coincide in several areas, including pressure, shear forces, and peripheral blood supply. Furthermore, heel PUs and DFUs may appear similar on clinical examination and assessment. A difference in causation is immobility/mobility. A patient with diabetes and a heel ulcer may not be recognised as having a DFU; clinically, the ulcer may be confused with a non-diabetic heel PU if the correct assessment is not conducted.
Assessment, referral and the multidisciplinary team
Correct assessment of the patient to identify the ulcer aetiology, independent of the terminology used to describe it, is critical to allocating the correct care pathway. An ulcer on the heel may be described as a PU, but if the patient has diabetes, it must be assessed as a DFU. This ensures that not only is the wound itself treated effectively, but also the underlying causes are clearly identified and managed and the correct guidance is given to the patient and their carer(s)/family. For example, a heel ulcer in a patient with diabetes, if managed as a PU, is highly unlikely to receive the required multidisciplinary team (MDT) approach which is recommenced for a DFU and will be at risk of complications, deterioration and amputation, all of which could have been avoided if the correct care pathway was followed.
Having identified the condition, the next step is referral to the health professional and/or team that is best qualified to manage the patient. The assessment should identify the key clinical and patient characteristics to be managed and indicates the skill sets required to address them. In the case of a DFU, referral to an MDT is the optimal pathway.
When a patient presents with a heel ulcer, the first step should be to exclude the possibility of diabetes and that it is therefore a DFU.8 If necessary, this step can be taken in the absence of the patient’s notes. Where no diagnosis of diabetes has been made, two clinical signs that differentiate between a PU and a DFU should be evaluated:
● Presence of diabetic peripheral neuropathy (DPN), leading to loss of protective sensation
● Reduced arterial blood supply (ischaemia)
Furthermore, mobility/immobility can help differentiate between a DFU and PU. If any of these signs (DPN, ischaemia, mobility) are present, then the patient should be directed to the DFU care pathway for further assessment. If these signs do not suggest that the patient has a DFU, the patient may follow the PU pathway. The following section provides guidance on simple tests for identifying the presence or absence of DPN and reduced blood supply in the patient’s feet, and to assess mobility.
Before the ulcer is assessed, the patient history should be taken according to local practice.
Assessment of diabetic peripheral neuropathy
Several tests are available for assessing the presence and severity of DPN. Diagnosis of DPN is made by determining presence or absence of sensation in the foot. The equipment required to conduct the tests varies between the simple and the highly complex, where access to power supplies is required.
Toe Touch Test: The simplest test, which requires no specialist equipment, is the Toe Touch Test or the Ipswich Touch Test (IpTT).73,74 The sensitivity (78.3%) and specificity (93.9%) are high. The test is always at hand, simple to conduct, safe to do, quick and easy to perform, and easily learned. It can be administered effectively by family and non-specialist carers after training.
The test is conducted by lightly touching the tips of the first, third and fifth toes and the dorsum of the hallux of both feet with the index finger, and noting whether or not the patient can feel or sense the touch. It is important that the index finger touch is light, without pushing, prodding, tapping or poking, to avoid the patient feeling the test by sensing movement or force. To ensure the patient is unaware of the point of touch, he or she should be blindfolded or shielded from viewing the test. If the patient cannot feel the touch on two or more sites out of eight, a diagnosis of reduced sensation is made. If the test indicates potential DPN, the patient should be referred for monofilament testing, where available.
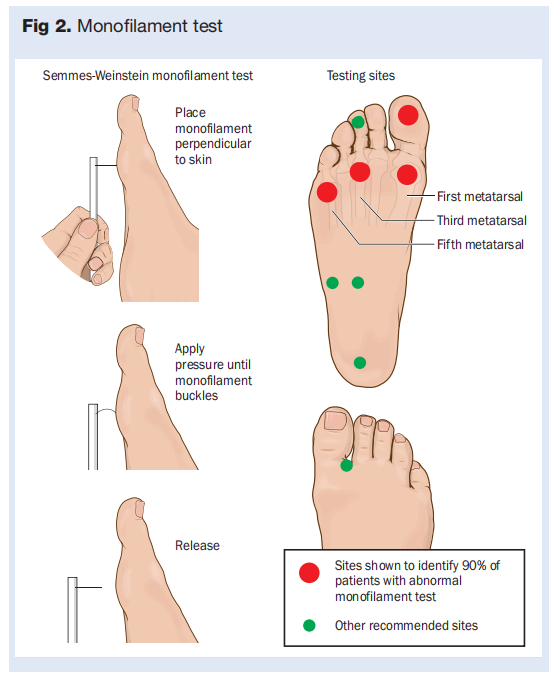
Nylon monofilament test: the next simplest test uses a monofilament nylon fibre, the Semmes Weinstein monofilament, which bends or buckles when subjected to a force of 10g when pressed against a surface.75 Different versions of the equipment used to conduct this test are available. The simplest is a short moulded plastic handle with the monofilament attached perpendicularly at one end. Other versions comprise a reusable handle with replaceable monofilaments.
The patient is introduced to the sensation by touching an area such as the hand or inside of the wrist. The monofilament is then applied to the tips and metatarsal heads of the first, third, and fifth toes75 or the tips of the toes and the halluces (Fig 2).76 The test should be conducted in such a way that the patient cannot see when the monofilament is applied to the skin to ensure fidelity. The monofilament is applied to the skin in a non-rhythmic pattern to rule out the possibility of the patient predicting when the test is being done. The patient should indicate if they can sense the monofilament. If the monofilament cannot be felt on any one site abnormal sensation in the foot has been detected. However, sensitivity increases when up to four plantar sites are tested. 75 Each monofilament must be rested for 24 hours after 10 applications75,77 and replaced when bent or depending on the manufacturer, after 70–90 applications to ensure that the filament has not weakened.78 It should be noted that different monofilaments perform differently.77 Those that meet the requirement for buckling at 10g force should be used. In busy clinics, it may be necessary to have more than one monofilament available to account for the need to rest the device. A further test based on the principle of the Semmes-Weinstein hair is the von Frey’s hairs test, which enables the practitioner to determine the threshold of touch sensation by using hairs that buckle at different forces.
Vibration perception threshold (VPT): the simplest to-use vibration-related device for assessing loss of sensation is a tuning fork with a specific frequency of vibration, 128 Hz. In one version of the test,79 the tuning fork is set vibrating by striking it on the palm of the hand for 40 seconds. As with the monofilament test, it is then applied to the hand or wrist. The test on the foot is conducted on the dorsal surface of the great toe on the bony prominence just proximal to the nail bed. The patient indicates whether the vibration is sensed and when the vibration has subsided and stopped. The test is repeated on the same foot and then the other foot in a non-predictable sequence.
An alternative to the tuning fork method is a small, battery-powered, hand-held device, the VibraTip.80 This device has been reviewed by the UK National Health Service body that develops guidance on new medical device technologies, the Medical Technologies Advisory Committee (MTAC), and is recommended for identifying peripheral neuropathy in the diabetic foot.81 It is used in the same way as the tuning fork.
Other methods to determine diabetic peripheral neuropathy: simple manual and complex electromechanical devices are available to identify DPN.82 Manual devices include the tactile circumferential discriminator, which detects the ability of the patient to discriminate two points applied close together on the skin, and a test that uses ball bearings of increasing diameters to identify which is the smallest that the patient can feel. A number of electromechanical devices are available to measure VPT. Examples are Biothesiometer, Neurothesiometer, Maxivibrometer, Vibrameter, Vibratron and the CASE IV system.82 These require access to power and may be unsuitable for use in many locations.
Ankle reflexes: absence of ankle reflexes is associated with an increased risk of foot ulcer formation in patients with diabetes. 83 The test requires a tendon hammer, which is used to strike the Achilles tendon. The health professional performing the test dorsiflexes the foot to put the tendon on stretch before striking with a hammer. Absence of a reflex is abnormal and indicates the need for further assessment.
Vascular status assessment
Several tests are available for assessing the presence and severity of reduced blood supply, which is indicative of possible ischaemia. Initial assessment may be done using simple tests that require no or minimal equipment, or by equipment of increasing complexity and greater discriminatory potential. In order to ensure that the patient is directed to the optimal care pathway, it is necessary to conduct only simple tests. Where vascular issues and reduced blood supply are suspected, the patient should be referred for specialist vascular assessment. Simple tests that require no or minimal equipment include:
Pulse palpation:84–86 Where other methods of identifying vascular issues and ischaemia are not available, palpation of dorsal pedal pulses allows initial screening and requires no equipment. In this test, the health professional assesses the pulse in the posterior and anterior tibial arteries by palpation. The posterior tibial pulse is palpated just behind the medial malleolus. The anterior tibial pulse should be palpated at the ankle, at the midpoint between the two malleoli, not more distally in the foot, where it lies deeper. The dorsal most prominence of the navicular bone is marked. Pulse palpation is evaluated by using two fingers, the index and middle fingers of the dominant hand. The posterior tibial is felt posterior to the medial malleolus of the tibia. For the dorsalis pedis, feel on the dorsum of the foot, lateral to the extensor tendon of the great toe.
Note: a diabetic foot with neuropathy and no ischaemia may present with a warm limb and bounding pulses.83 In this case, do not rely only on pulse palpation for differentiating between a PU and a DFU, but use all assessment outcomes as a set to inform the decision. Furthermore, PAD can still be present, despite the presence of a palpable pulse.
Ankle-brachial pressure index (ABPI): ABPI involves the ratio of systolic pressures in the brachial artery at each elbow and systolic pressures in the posterior tibial and dorsalis pedis arteries at each ankle.ABPI is calculated for each leg separately. ABPI is conducted with the patient in the supine position (lying down). Evidence states 10 minutes of supine rest as a minimum before pressure measurement is recommended, to allow equaling of the vascular beds which determine arterial pressure.87,88 The sphygmomanometer cuff is placed around the ankle above the malleolus. The location may vary slightly from anywhere from just above the malleolus to 2.5cm above the malleolus, depending on which guidelines are followed. Where the ABPI is recorded ≤0.9,89 the patient should be referred for further specialist vascular assessment, using more sensitive methods.
Patients with diabetes may have hardening of the arteries and medial arterial calcification (MAC) in the lower leg and foot, which reduces the compressibility of the arteries. The presence of MAC is known to reduce the compressibility of the vessel and can lead to false elevation of the ABPI. This makes ABPI interpretation in diabetes populations difficult. Health professionals should be aware that the ABPI should not be used as a stand-alone screening tool in diabetic populations, but in conjunction with other testing methods. Health professionals should consider using other non-invasive, vascular tools, such as hand-held Doppler auscultation alongside ABPI to aid accurate identification of PAD. Where the ABPI is measured as ≥1.3, further tests, such as a toe-brachial index (TBI), should be performed and if this is not possible, the patient should be referred for vascular assessment.
Note: diabetes involves the medium lumen and therefore the ABPI might not be accurate and a TBI is better.
Toe-brachial Index (TBI): TBI represents an alternative diagnostic tool in patients with diabetes and PAD. Digital arteries are usually less affected by calcifications, which provides insight into the microvascularity of the smaller vessels of the foot. TBI is obtained by dividing the toe systolic pressure by brachial systolic pressure. Since toe pressures are generally about 60% that of brachial pressures, prognosis is relatively good when toe systolic pressure is >50mmHg.90 TBI>0.7 is considered within normal limits, TBI≤0.7 is an indication of PAD and TBI≥1 was an indictaion of distal arteries calcification.
Doppler ultrasound: assessing the sound waves from a hand-held Doppler can provide information about the condition of the arteries and blood flow. The Doppler machine provides an audible sound or visual tracing, which is created from the movement of blood in the vessel. PAD can change the sound and shape of the waveforms. A triphasic sound/waveform indicates healthy arterial flow. The third sound within the triphasic wave form comes from the dichrotic notch, which is formed from the elastic recoil within the artery. As the elasticity within the artery reduces, this can affect the production of this sound/wave; this represents a biphasic tone, which is an indication of arterial hardening, but not occlusive PAD. A monophasic wave form formed though a signal sound/ wave is indicative of the presence of PAD.
The first test should be pulse palpation. Furthermore, ABPI could be false in patients with arterial calcification. If the patient does not have a pulse and has ulceration, refer, where possible, to a vascular specialist (or relevant health professional) for a full assessment.
Patient assessment
In most cases, the health professional who conducts the initial assessment of a patient with a heel ulcer is the ‘wound care navigator’ (WCN).91 Referral to the WCN may have been made by a general practitioner or other primary care practitioner, a nurse, or the patient may have self-referred. The wound skill level of the WCN with respect to wound management may be high—as with a podiatrist, wound, ostomy and continence nurses (WOCN) in the US, tissue viability nurse (TVN) in the UK, TVN or advanced nurse practitioner in Ireland or a nurse with advanced wound care knowledge in other parts of Europe.
The extent of patient management undertaken by the WCN should be in line with their skill level, with referral further through the health-care system, according to the patient’s clinical needs. Minimally, the WCN should be trained to conduct the initial steps required to assess the patient and to conduct the tests required, based on the ulcer characteristics. Local or national guidelines should be consulted to ensure that optimal care is delivered. In general, the steps are:
1 Record patient history: including: patient characteristics, such as age and sex, relevant medical history, current medications and previous ulceration or amputation. The health professional should specifically ask about diabetes; the patient may disclose that they have diabetes or may not know, if it is undiagnosed. A family history of diabetes, especially type 2, is important. Record the duration and type of diabetes if it is known. Record the lower limb condition—hairs, temperature, colour, skin conditions, such as hyperceratosis. Also, note how the ulcer is being managed at the point of presentation, for example, whether the patient is using offloading of any sort.
2 Assess the wound characteristics: including location (plantar, heel, metatarsal head(s), instep, dorsal, lateral), size, depth, including presence of underlying function, edge and periwound appearance, exudate type, visual appearance, pain, presence of infection and surrounding cellulitis and redness. Skin condition (whether it is dry, atrophic, and/or there are fissures/ cracks) and temperature (a dramatic drop in skin temperature from proximal to distal along the lower limb) can be a sign of poor blood flow. Assess the foot for callus and deformity, which increase local pressure, for example, hammer toes, prominent metatarsal heads and Charcot deformity. Amputation should also be recorded. Assess between the nails and toes for signs of fungal infection. PUs on the foot are usually located on the heel.
When assessing a wound, the acronym MEASURE may be useful.92 The acronym stands for:
M: measure size
E: exudate amount (none, scant, moderate, heavy) and characteristics (serous, sanguinous, pustular, or combinations)
A: appearance, necrotic (black), fibrin ( firm yellow),slough (soft yellow), or granulation tissue (pink and healthy versus red and friable—easy bleeding, unhealthy)
S: suffering pain
U: undermining, measured in centimetres and position in the ulcer recorded
R: re-evaluate
E: edge (hyperkeratotic, macerated, normal).
3 Identify the degree of patient mobility: if the patient is bedbound or relatively immobile, it is likely that the ulcer is a PU, whereas if a patient is reasonably mobile, it is more likely that the ulcer is a DFU. Attention should be made to the activity and mobility elements of the risk assessment tool used in the specific practice setting.
4 Assess DPN and/or blood supply using the test best suited to the equipment and skills available: this may be a simple test requiring no equipment, such as pulse palpation and the Toe Touch Test.
5 Refer the patient to the appropriate care pathway based on the overall outcomes of the assessment: these pathways should be described by local guidelines. Note: if the patient identifies as diabetic, this may be enough to lead to a referral; however, a full assessment will aid with referral urgency.
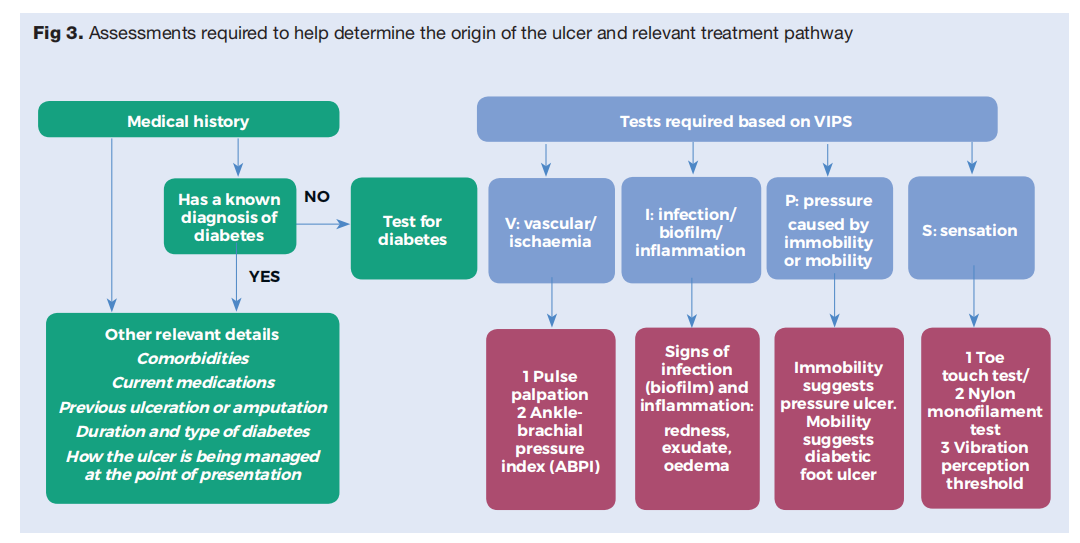
The consensus panel decided that a useful guide to the key aspects required for the assessment of an ulcer on the foot of a diabetic patient is the mnemonic ‘VIPS’ (Table 1, Fig 3):
● V: vascular/ischaemia
● I: infection/biofilm/inflammation
● P: pressure
● S: sensation/neuropathy
Grading systems
The effective care of the ulcer depends on clear and accurate diagnosis and description of the condition. Where the skill level is appropriate, management may be conducted by the WCN, or the patient may be referred to an appropriate health professional/service.
Many grading systems for PUs and DFUs have been published by expert groups or institutes. The healthcare provider may have developed a local grading system, which should be used if available. Where a local or national grading system is not available, a grading system developed by expert consensus or other developer should be used. Grading systems assume a level of skill to recognise and differentiate the scoring parameters and must be administered by appropriately-qualified staff.
PU grading systems
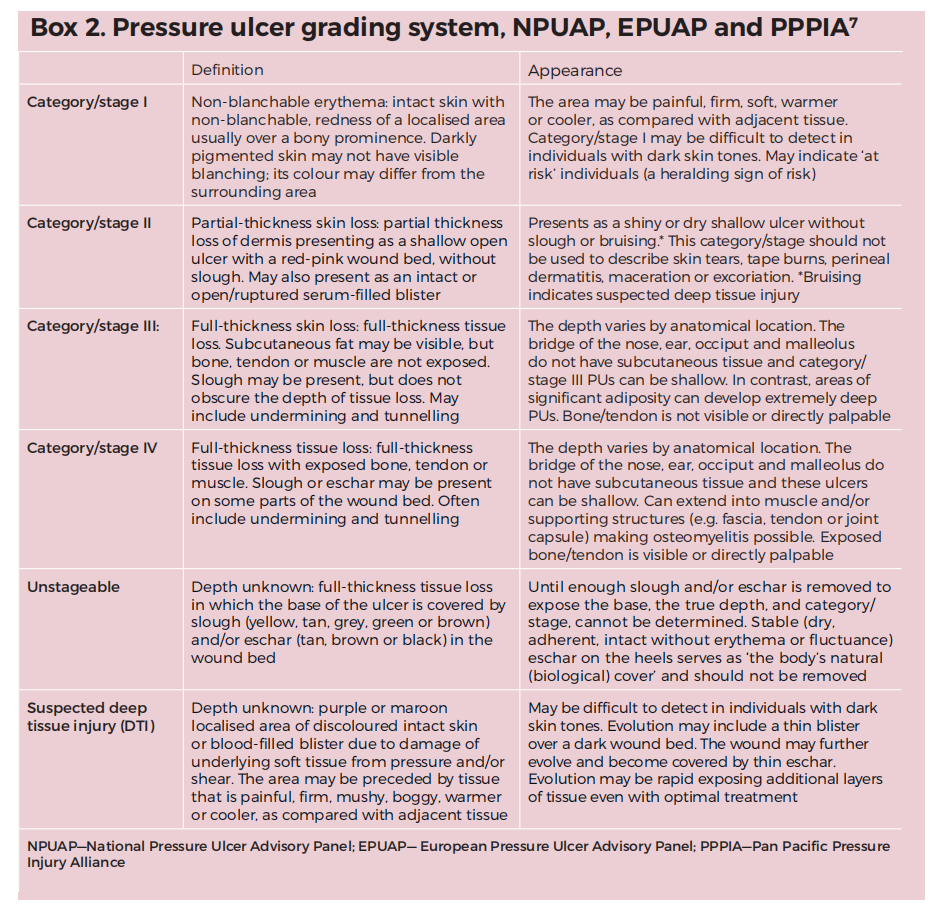
The most widely used grading system for PUs is that prepared by the NPUAP, EPUAP and PPPIA.7 The term ‘pressure ulcer’ has recently been subject to review. The NPUAP in the US has proposed adoption of a new term, pressure injury (PI). This document continues to use the term pressure ulcer. The NPUAP, EPUAP and PPPIA grading system is based on the depth of the PU and the extent of tissue involvement, and assigns a PU to ‘categories’ or ‘stages’ as shown in Box 2.
DFU grading systems
A number of grading systems for DFUs exist. The most commonly-used systems are SINBAD, Wagner, University of Texas, Wound Ischaemia and Foot Infection (WIfI) and PEDIS. In general, the grading of DFUs is based on the size of the ulcer and the presence or absence of DPN, PAD and infection, although the detail of how this is achieved by each system varies. Where they exist, clinicians should use local grading systems. Where no local system is available, one of the existing systems should be adopted, according to local preference.
SINBAD93 is an acronym for: site; ischaemia;
neuropathy; bacterial infection; area; and depth. Each parameter is allocated a score of either ‘0’ or ‘1’ according to the system shown in Box 3 and the total score for the DFU is calculated. Higher scores indicate greater severity.
University of Texas: assesses the DFU on two parameters and provides an alphanumeric score that is a combination of the two, as shown in Box 3.
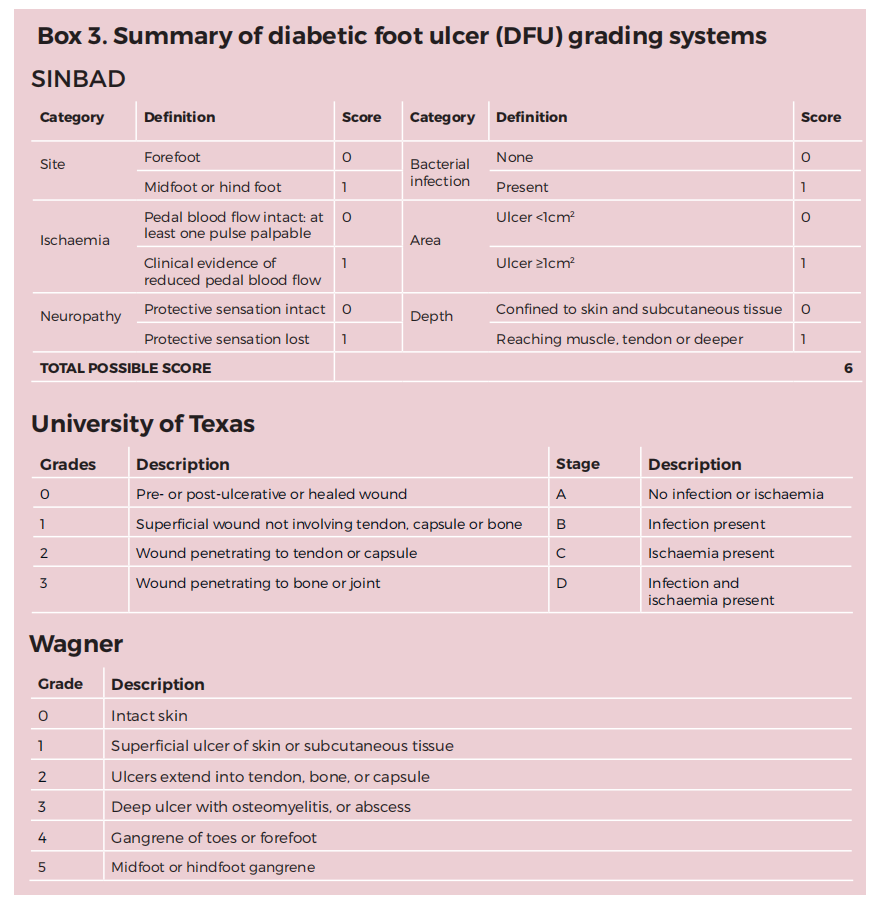
Wagner94,95 uses six definitions that incrementally describe a DFU by the degree of severity (Box 3).
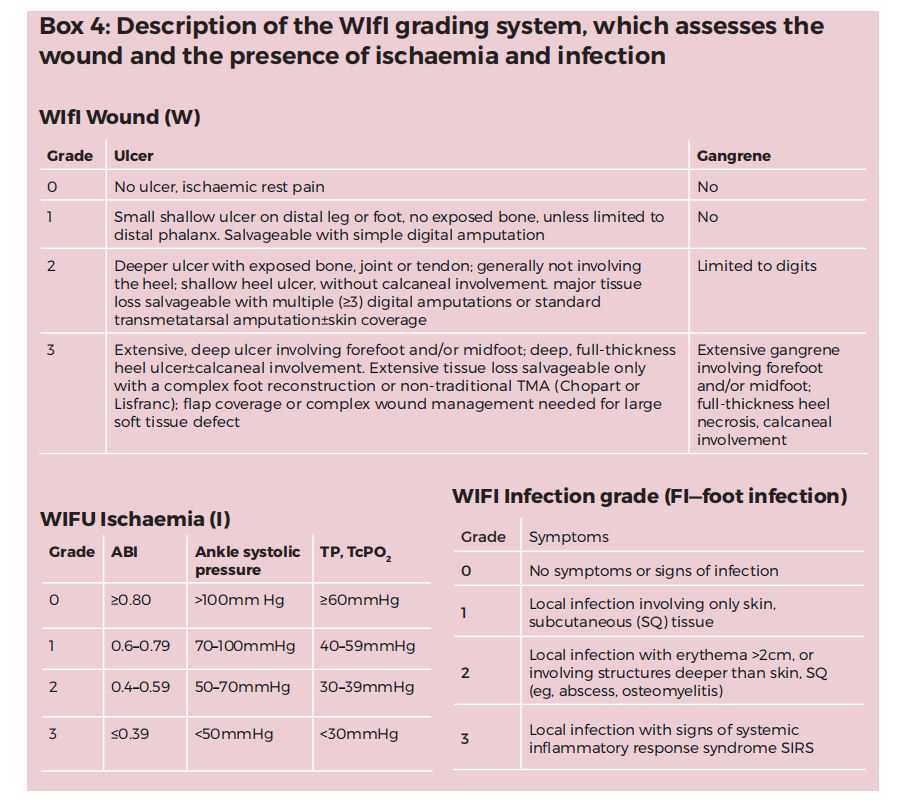
Wound Ischaemia and Foot Infection (WIfI):96 developed to assess patients with critical limb ischaemia. WIfI assesses the wound, ischaemia, and foot infection and assigns a score to the ulcer. The WIfI system correlates well with outcomes for wound healing and amputation..97 The scoring system is shown in Box 4.
PEDIS: developed by the IWGDF to use strict criteria that are applicable worldwide.98 It was created primarily for use in research and, as such, is unlikely to be used widely in the management of DFU, outside research.98
Risk assessment
Risk assessment estimates the level of risk that a patient will develop a new ulcer or a recurrent ulcer and, in the case of DFU, progress to amputation. It is recommended that risk assessment be conducted for all patients who currently do not have an ulcer, or who have a healed ulcer, in order to identify where prevention strategies should be focused. Where local guidelines are available for conducting risk assessment, these should be used. Where local or national guidelines are not available, there are a number of risk assessment tools or instruments that may be used.
Pressure ulcer risk assessment Many risk assessment tools have been developed for PU. Examples include the Braden Scale and Waterlow. 99 PU risk assessment should be a combination of a structured assessment based on a tool and clinical judgement. 7 Good clinical judgement requires experience in risk assessment; if there is any doubt, at least one other person should carry out the assessment. Risk assessment should be conducted and documented as soon as possible after a patient is referred or presents, and no later than six hours after arrival. It should be repeated, especially if there is a change in the patient’s condition, or for PUs. PUs in hospital inpatients should be assessed daily, if possible.100
Factors reported to increase the risk of PU formation include poor skin condition, an existing PU, immobility, poor nutritional status, higher or lower than average BMI, female sex, greater age, incontinence and increased skin moisture, comorbidities such as cachexia and organ failure, PAD, anaemia, motor and sensory impairment, spinal injury, and diabetes. Most risk assessment tools are based on these risk factors and assign a score to the patient which identifies the risk category for PU formation in the patient. A risk factor for heel PU in particular is a degree of mobility that allows the patient to move themselves, for example, on a bed, or the presence of leg spasms, Parkinson’s disease or tremors causing heel rubbing, agitated heels, and frequent rubbing by sliding on a bed or chair. Articulated bed frames can also increase risk of heel PU.
Skin inspection is a critical step in PU prevention and should be performed regularly. The skin should be inspected within six hours of admission to a hospital and daily thereafter. All skin sites susceptible to PU formation should be assessed for pain or discomfort reported by the patient and the skin should be checked for:
● Skin integrity in areas of pressure
● Colour changes or discolouration. Non-blanchable erythema may present as colour changes or discolouration, particularly in darker skin tones or types
● Variations in heat, firmness and moisture ( for example, because of incontinence, oedema, dry or inflamed skin).
Use finger palpation to determine whether erythema or discolouration (identified by skin assessment) is blanchable. A simple test to assess redness is to place a transparent plastic disc over the skin as it is depressed. Blanchable redness is identified by the skin losing redness which returns when the pressure is released and blood reperfusion occurs. Nonblanchable redness does not lose its red colouration and indicates development of inflammation in the skin. Where available, diascopy may be used to evaluate skin.7
Developments in skin assessment include new methods to assess pathological change in at-risk skin. Where skin changes that may lead to PU formation have started, the tissue becomes inflamed. Early inflammatory changes include extravascular fluid accumulation in the matrix of skin which are not visible to the naked eye. This fluid is called subepidermal moisture (SEM). The assessment method measures an electrical property of skin—impedance— which changes with SEM.101,102 A device to measure SEM is commercially available and can detect potentially damaging skin changes up to five days before they are visible to the eye. Where available, the use of this device should be considered.
DFU risk assessment
All patients diagnosed with diabetes who develop peripheral neuropathy are at risk of DFU formation and should be managed according to local, national or international guidelines. The IWGDF has issued guidance on prevention of DFU based on assessing risk posed by DPN, foot deformity, PAD and history of foot ulceration. The associated screening frequency is recommended (Table 2). Risk assessment for progression of ulceration to amputation is covered by the WIfI assessment tool.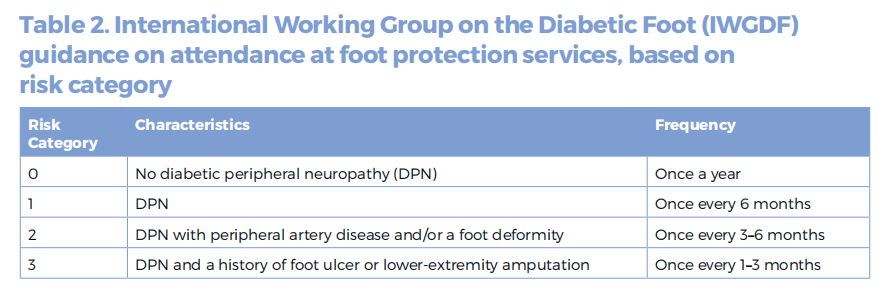
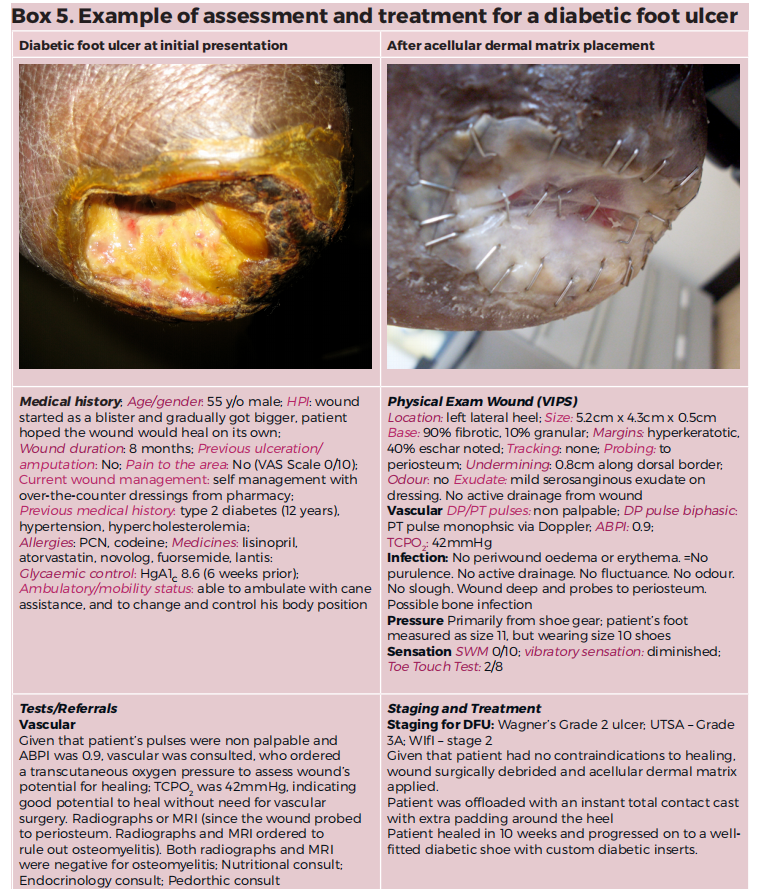
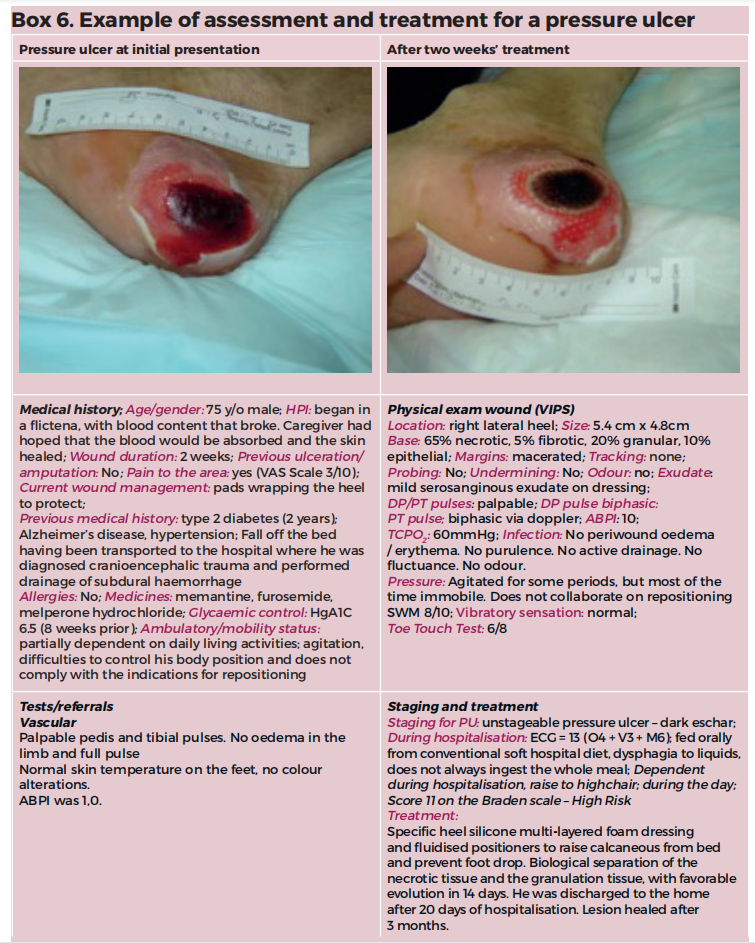
Every patient with diabetes and an ulcer should have a health professional perform a simple assessment in order to determine if a vascular assessment is required. For example, if a nurse was able to feel a pulse palpation, that should be enough to rule out the possibility of an ischaemic condition. However, if the wound fails to heal or there is any doubt, the patient should be referred for further non-invasive testing e.g. TBI and ABPI. Boxes 5 and 6 are examples of case study assessments of patients with diabetes and foot ulceration.
Referral
Following assessment and identification of the most likely type of ulcer, the patient should be referred as early as possible to the appropriate care pathway. It is important that the correct clinical procedures and competencies are brought to bear on the wound. Often, those will not necessarily reside in a specific health professional. The pathway that provides the optimal care, irrespective of the person who delivers
Procedures and competencies potentially required for a PU are infection management, nutrition management, debridement, pressure relief, friction and shear management, medicines, and surgery. the care, should be followed.
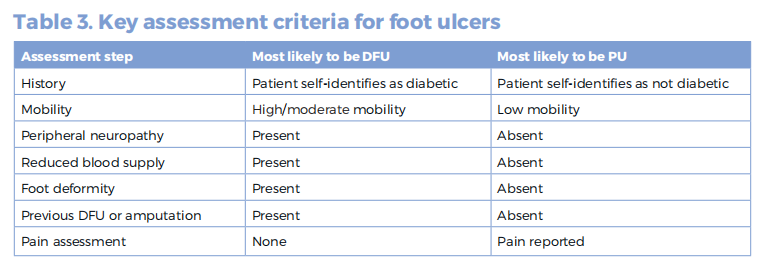
In the case of a DFU, the guidelines recommend referral to an MDT in order to manage the complexity of a patient with diabetes and a wound. Patients managed by an MDT have better outcomes than those not managed in this way.91 Guidelines recommend that referral should take place promptly and within 24 hours of identification of a DFU.28 Evidence suggests that this rapid referral does not happen in the majority of cases.103–105 Correcting referral intervals is likely to be a major contributor to shortening the time-to-heal for a DFU and avoiding progression to amputation. Procedures and competencies in an MDT for a DFU are wound care, infection management, nutrition management, debridement, pressure relief, friction and shear management, and surgery. Table 3 shows the key assessment factors for PUs and DFUs.
Emergency referral
Emergency referral is required when the patient suffers from a severe infection, according to Infectious Diseases Society of America (IDSA) guidelines and there is a high risk to the patient’s life. This is especially important where there is deep soft-tissue infection, necrotising soft-tissue infection, acute limb ischaemia and osteomyelitis with systemic signs ( fever, tachycardia, tachypnea, leucocytosis. etc).
The multidisciplinary team
An MDT, which may also be known as an interdisciplinary team, is a group of specialists with all the skill sets appropriate to the management of a specified condition. An example is a surgical team, comprising theatre staff, nursing, anaesthesiology, surgeons, ICU practitioners and so on. The critical point is that, whatever structure is in place, the patient should receive the best multidisciplinary care for the wound. A characteristic of an MDT is effective communication to ensure delivery of integrated care to the patient. Patients managed by an MDT tend to have better outcomes than those not managed by one.91 The constitution of an MDT varies worldwide91,106 and generally they are associated with the acute care setting rather than the community. Nevertheless, a patient in the community who meets the guidelines for management by an MDT, perhaps because of a change in status of the wound, should be referred to one. In the case of DFU, the IWGDF recommends an MDT should have three levels of the following structure and skills:
● Level 1: general practitioner, podiatry, diabetic nurse
● Level 2: diabetologist, surgeon (general, orthopaedic or foot), vascular specialist, endovascular interventionist, podiatrist and diabetic nurse, in collaboration with a shoe-maker, orthotist or prosthetist
● Level 3: a level 2 foot centre that specialises in diabetic foot care, with multiple experts from several disciplines, each specialised in this area working together, that acts as a tertiary reference centre.
The ASEAN guidelines recommend the following competencies in a DFU MDT: surgery for diabetic foot problems; diabetology; diabetes nursing; podiatry; tissue viability or wound management; specialist competencies including vascular surgery, radiology, clinical microbiology, nephrology and cardiology.
Many DFUs in Europe are overseen by podiatrists who make the clinical decision to refer the patient to the full MDT. Some countries stipulate that patients are managed by physicians who make the decisions on the care plan and referrals. MDTs with responsibility for the management of any chronic or acute wound are being set up in Malaysia.
To treat patients with a diabetic foot ulcer successfully, quality parameters of the facility’s structure, treatment procedures and the patient outcome are needed. Structural quality is based on the qualifications of staff and the facility’s spatial conditions, as well as a minimum of equipment. The application of available guidelines and documentation systems, as well as the establishment of a team approach between the facility’s staff and other experts involved (vascular specialist or surgeon, orthopaedic surgeon, radiologist, podiatrist, orthopaedic shoemaker etc.), are the requirements of procedural quality. Outcome quality includes: wound healing rate and time, rate of amputation (major and minor), vascular intervention (bypass surgery, percutaneous transluminal angioplasty), death rate, clinical admission. In Germany, a certification system was established in 2005; there is a clear link and rules for responsibility, from general practitioner (GP) to diabetologist and finally specialised centres. Centres are available in all regions of Germany. A similar system was established in Belgium.
Competencies required may also include: infection control, infection management and microbiology, wound care, total contact casting (TCC), physiotherapy, occupational therapy, nutrition and patient education. Some countries may not have practitioners with a functional title such as podiatrist. However, the functional name is less important than the availability of the skills of a podiatrist. In many European countries, the US and Australia, podiatrists are the main practitioners who manage patients with DFU daily and who refer to the MDT, but this is not always the case. The key competencies of a podiatrist in an MDT include:
● Vascular and neuropathy assessment
● Identifying foot deformities and joint mobility range
● Foot care (removal of calluses, nail care)
● Diagnosis and management of infection through prescription of antibiotics and surgical intervention, especially for osteomyelitis
● Prophylactic and conservative surgery in some countries for the correction of the deformity
● Off-loading
● Prevention of the recurrence or re-ulceration through insoles and therapeutic shoes
● Surgical and sharp debridement.
PUs are most often managed by nursing staff, who refer to the appropriate clinical staff as required, but this is not usually under the auspices of a formal MDT. In the absence of a formal MDT, PUs are managed by an interdisciplinary group of practitioners. This panel recommends considering creating an MDT for managing PUs. An example of the membership is provided by the AHRQ.18
This article is excerpted from the JOURNAL OF WOUND CARE n SUPPLEMENT C ONSENSUS DOCUMENT VOL 27, NO 5, MAY, 2018 by Wound World.

