The sixth World Union of Wound Healing Societies (WUWHS) Congress took place on March 1–5, 2022, in Abu Dhabi, United Arab Emirates. The congress featured a Mölnlycke-sponsored workshop titled ‘Surgical incision care – negative pressure wound therapy and advanced dressings: what to use and when’. The workshop was led by an international expert panel and had the following aims:
■ To highlight the importance of postoperative incision care and the associated challenges
■ To discuss the performance requirements from surgical dressings and a closed-incision negative pressure wound therapy (ciNPWT) system
■ To explore the ways in which risk assessment tools can facilitate clinical decision-making.
Importance of post-surgical wound care
Wound infection is a considerable problem worldwide and, despite advances in surgical techniques and wound care practice, awareness of the risk of surgical site infections (SSIs) may not translate into action that could potentially reduce the risk.
Appropriate dressing choices and use of protocols is an element that is integral to managing this risk. Moreover, the importance of post-surgical wound care is often only discussed once surgical wound complications (SWCs) develop, rather than it being a consideration before surgery as a preventative strategy.
Prevention of post-surgical wound complications are multifactorial and include accurate preoperative risk assessment of the patient, optimum surgical and intraoperative techniques, and appropriate post-surgical care. This includes an understanding of the wound dressings available, and which may play a role in reducing the risk of complications. Historically, NPWT was viewed as a treatment option once an incisional site had become infected or dehisced. Now ciNPWT is increasingly being considered as a primary solution to support and promote healing, achieve good-quality repair of the skin, and reduce complications (WUWHS, 2016).
Surgical wound complications (SWCs)
Dr Sandy-Hodgetts introduced the topic of SWCs [Box 1], defined as a disruption to normal incisional wound healing following surgery. It is estimated that 313 million surgeries are conducted annually around the world (Meara et al, 2015). A normal inflammatory response following surgery is to be expected within 72 hours and full closure in the first 6–8 weeks. Despite this, complications can occur such as infection or dehiscence and may be related to patient-related comorbidities, intraoperative and postoperative risk factors related to SWD (SandyHodgetts et al, 2018). SWCs typically occur 7–9 days postoperative, up to and including 90 days postoperative and are commonly managed in both the acute and post-discharge setting (Sandy-Hodgetts et al, 2020).
SWCs have been shown to delay healing and result in considerable morbidity, mortality and related socioeconomic costs (Leaper et al, 2013; Sandy-Hodgetts et al, 2013), which are attributable to several resource implicated factors such as:
■ Extended length of stay
■ Revision surgery
■ Clinical resources required
■ Increased hospitalisation costs.
Preventing SSIs or SWCs goes beyond dressing selection or surgical protocol or procedures to also include the preoperative, intraoperative and postoperative phases [Figure 1]. Dr Sandy-Hodgetts explained that it is necessary for clinicians to keep the patient at the centre of care and to monitor their journey through the preoperative, intraoperative and postoperative phases, including post-discharge from acute care (Sandy Hodgetts et al, 2020).
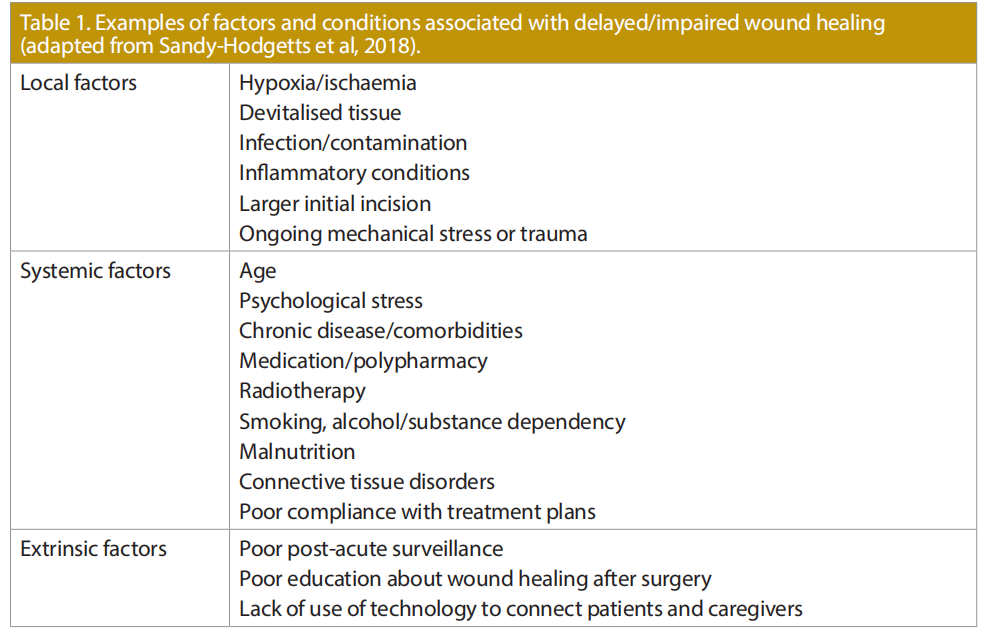
Pre-surgical risk assessment is a key aspect and delegates were signposted to a paper presenting a conceptual framework that outlines the risk factors associated with SWD as identified in the literature (Sandy-Hodgetts et al, 2018; 2020; Table 1). Incorporated within the patient-centric conceptual framework are patient-related comorbidities, and intraoperative and postoperative risk factors related to SWD. It can be used as a guide to implement preventative strategies or using postoperative dressings for incisional management.
Regional considerations
Work has already begun to identify the key dressing criteria required for post-surgical wounds internationally (Morgan-Jones et al, 2019; SandyHodgetts et al, 2020), and regionally in the AsiaPacific region (Morgan-Jones et al, 2021a; SandyHodgetts et al, 2021), Northern Europe region (Morgan-Jones et al, 2021b) and Eastern Europe region (Morgan-Jones et al, 2022).
Several expert panel members agreed that in regard to dressing wear time following surgery, it is important to choose a dressing that can effectively manage the exudate and afford extended wear time in terms of exudate absorbency and retention, as well as sustained mechanical integrity (durability) throughout the intended period of use.
The concept of undisturbed wound healing (UWH) is of particular importance in surgical wounds, as using a dressing with an increased wear time and keeping the dressing in situ can help to reduce the risk of contamination (Morgan-Jones et al, 2019; Sandy-Hodgetts et al, 2021). However, there are cases when promoting UWH is not suitable. Potential indicators that a dressing change is necessary (or preferred) include (Morgan-Jones et al, 2021a; Sandy-Hodgetts et al, 2021):
■ Saturated dressing
■ Dressing leakage
■ Geographical factors — in some areas, patients have to travel long distances and may have limited resources available at home, so prefer their dressing to be changed before discharge
■ Staffing/competency issues — who carries out the dressing change can influence decision-making, depending on the structure and staff being in place to safely change the dressing
■ Social influences and patient preference — the patient may prefer the dressing to be changed.
There are some region-specific considerations in dressing selection and wound healing, including factors around the dressing or cultural considerations (Morgan-Jones et al, 2021a; Sandy-Hodgetts et al, 2021). For example, waterproof dressings are very important in humid/tropical climates as they can prevent the dressing from peeling off (Morgan-Jones et al, 2021a).
Patients travelling long distances should also be a consideration in dressing selection and frequency of dressing changes; it is important that patients can be confident they have the information and resources they need when they are far from the hospital, so that they are able to self-manage their surgical wounds at home (Morgan-Jones et al, 2021a).
Product availability across differing geographic regions can present issues for dressing choices in clinical management, as not all dressings are widely available in all care settings. Cost is also a consideration. However, when selecting an appropriate dressing type, the total costs of care should be considered in tandem with the individual dressing or unit price (Morgan-Jones et al, 2021a; Sandy-Hodgetts et al, 2021).
Patient-related factors
In terms of patient-related factors, the expert panels members agreed that patient comfort is very important, and that the patient should be provided with information on all aspects of their treatment (Morgan-Jones et al, 2019; 2021a; 2021b; Sandy-Hodgetts et al, 2021; MorganJones et al, 2022). A healthy rapport and trusting relationship should also be built with the patient. Optimising patient-related risk factors that are modifiable or non-modifiable is key in terms of risk assessment and dressing selection (Sandy-Hodgetts et al, 2018; 2019; 2020; 2021). Reducing the risk of SWCs through use of rigorous clinical guidance, such as the World Health Organization (WHO) Global Guidelines on the Prevention of Surgical Site Infection (WHO, 2016) or the Enhanced Recovery After Surgery Protocol (ERAS, 2016) is integral to improving wound healing outcomes in clinical practice.
The initial international expert panel (MorganJones, 2019) identified the six properties of the ‘ideal’ post-incisional dressing that cannot be met by traditional island or film pad dressings — only advanced dressings. The other expert panels have since updated the requirements to the following (Morgan-Jones et al, 2021a; 2021b; 2022):
■ Flexible (not impede the patient’s movement), providing elasticity to avoid pulling the skin or blistering (e.g. particularly over joints)
■ Well-fixed to the skin on application once the skin is dry after being disinfected and remains adhered if there is sweating (more issue of abdomen)
■ Absorbent of wound exudate (retain/lock in the fluid; no exudate leakage should occur from the dressing to the periwound skin)
■ Protective of the surrounding skin to reduce the risk of blistering or irritation and provide patient comfort, with minimal discomfort or pain during dressing removal
■ Waterproof to provide a good seal/barrier function and enable the patient to shower
■ Eliminate dead space between the wound bed and wound dressing where necessary to avoid exudate pooling
■ Easy to use and remove by patients and all care staff to ensure consistent care
■ Transparent dressing borders to allow for observation of the surrounding skin.
Delegates were asked to consider their ideal postoperative incision dressing and the post-surgical dressing practices in their locality (i.e. average dressing wear time, whether the principles of UWH are in place and how findings from the expert panels may impact their clinical practice).
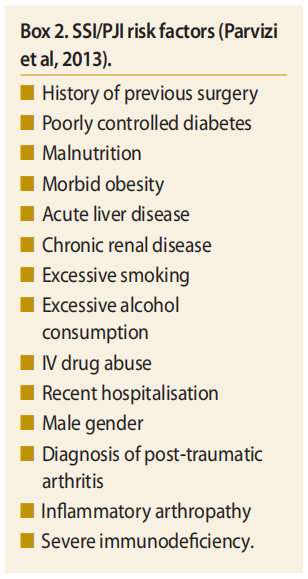
The International Surgical Wounds Complications Advisory Panel (ISWCAP) have published a Best Practice Statement for the early identification and prevention of surgical wound complications and highlights the need for preoperative risk screening (Sandy-Hodgetts et al, 2020). Additionally, the International Consensus on periprosthetic joint infection (PJI; Parvizi et al, 2013) have considered risk factors for SSI/PJI [Box 2], yet more work is needed to optimise patients prior to surgery.
Building on the International Consensus, a surgical site event risk assessment (SSERA) project was carried out with an international panel who met to consider the key risk factors for SSI following orthopaedic surgery, along with their interpretation of the relative importance of each risk factor. The consensus panel was assisted through an evidence-based review of relevant publications. A robust evidenced based risk assessment (minimal, low, medium and high risk) and stratification model for predicting SSI following orthopaedic surgery was created. The proposed risk calculator is an initial ‘work in progress’ and will be modified through future consensus group meetings and review of supportive literature that both validates and possibly invalidates some of the assumptions.
Rhidian Morgan-Jones explained that preoperative risk assessment and optimisation in the UK can certainly be improved and should include the:
■ Skin/soft tissues factors (e.g. scars, inflammation, ulceration, vascularity)
■ Previous surgeries
■ Patient factors (e.g. comorbidities, smoking, diabetes, BMI)
■ Operation factors (e.g. type, complexity, length of surgery and the surgical position).
Currently, the UK is taking steps towards a revision network to ensure that surgery is performed in the most appropriate centre and by the best possible surgeon for the task, which will have a significant impact on patient outcomes (British Orthopaedic Association, 2020).
NPWT or advanced dressings: what to use and when
Dressing selection and the protocol of using the chosen dressing type (such as the frequency of dressing changes) will heavily influence the post-surgical management and should ideally enable early patient mobilisation. Dressing wear time can vary according to surgery type, local protocol and clinician choice; however, a standardised protocol for dressing changes can include near-saturation (not stained), occurrence of leakage around the dressing and clear cellulitis. If these are not observed, the principles of UWH should be adhered to.
Delegates considered what drives the surgeon’s choice of a dressing (i.e. habit, training, experience, bias, cost, research, availability of dressing choices in the relevant care centre, delegation and the patient/wound). The ‘ideal’ dressing properties outlined above were identified as the key factors as they put the patient and their wound at the centre of the decision-making process (e.g. absorbency and retention, no dead space between the dressing and wound bed, flexible dressing materials, waterproof, long wear time, good adhesion and comfort during wear and removal). These properties are also ideal for orthopaedic/surgical wounds, helping with early mobilisation and discharge and reduced complications.
The final presentation by Amit Gefen reflected on the design requirements from an effective single-use NPWT system. NPWT is a well-established method that employs a suction pump, tubing and an absorptive dressing. The therapy removes excess exudate and promotes healing in both acute and chronic wounds. The benefits of NPWT have been extensively reported in the literature such as (WUWHS, 2016):
■ Protecting incisions from external contaminations
■ Holding the closed incision edges together, in synergy with the sutures that provide the primary closure
■ Reducing seroma and haematoma fluid collection
■ Improving perfusion
■ Reducing oedema.
The biomechanics of NPWT for incision wounds
From a biomechanical perspective, NPWT has an important role in managing closed incisions following surgery. If only primary closure is applied by means of surgical sutures, considerable mechanical stress concentrations develop in the skin and underlying soft tissues around the focal points of the suture insertion sites (Katzengold et al, 2018; Orlov and Gefen, 2022). When NPWT is applied after primary closure, and once it participates in the mechanical closure system, it applies continuous joining forces and shares the effort of the sutures in the closure of a surgical incision (Katzengold et al, 2018; Orlov and Gefen, 2022).
Types of single-use NPWT systems
In terms of the design concept of NPWT, two types of single-use NPWT systems are currently available to treat surgical wounds: canister-based and canisterless, also known as ‘canister-free’. Both types of single-use NPWT systems manage the wound exudate through a multilayer wound dressing, connected to a pump unit by a tube for creating and inducing the negative pressure in the wound bed via the dressing. In canister-based systems, fluid from the wound is managed between the dressing and a canister, which collects excess exudate and infectious substances. In canisterless systems, the fluid is managed only by the dressing and therefore dependent on the moisture vapour transmission rate of the dressing for fluid management (Henriksson, 2021).
This works if there is low exudation or fast evaporation from the dressing, or both. However, for medium to highly exuding wounds, and/or if evaporation is slow (e.g. due to humid ambient conditions), there may be a near saturation state forming in the dressing, which causes substantial pressure losses in the wound bed, and so the NPWT system will no longer deliver the intended pressure to the surface of a wound. When this occurs, there is no more effective sharing between the closure efforts of the NPWT system and the sutures. Accordingly, once such pressure losses occur, the focal stress levels around the sutures rise, again forming a stress concentration state around the wound that would be similar to a situation where there is no NPWT in place (Orlov and Gefen, 2022).
Performance of a canister-based versus a canisterless system
In a recent paper, Orlov and Gefen (2022) investigated the performance of a canister-based versus a canisterless single-use NPWT system, each with a different negative-pressure setting and technology for fluid management. A sophisticated computational (finite element) modelling framework considering the surgical incision, sutures and single-use NPWT system and a laboratory bench-test for simulated clinical use were developed. A pre-clinical study conducted in a porcine model for closed incision treated by means of single-use NPWT was further performed.
After analysing the results from all these different research modalities, Orlov and Gefen (2022) noted that a greater (absolute) negativepressure level and its continuous, consistent delivery through a controlled fluid management technology, by removing excess fluid from the dressing into a canister, provides far superior biomechanical performances in terms of sharing the closure efforts between the sutures and NPWT and, consequently, the quality of the repaired tissue improves.
Specifically, the current comprehensive and rigorous experimental-computational study demonstrated that the above conditions are more likely to result in better stiffness and strength properties of the repaired skin (Orlov and Gefen, 2022).
Conclusion
This workshop explored the choice of dressings for post-incisional wound care, properties of the ‘ideal’ dressing, risk assessment for orthopaedic surgery and the ideal requirements from an effective ciNPWT system.
A key message is that patients deserve optimum levels of care during and after their surgical journey; however, advanced dressings are required to meet the needs of the patient and clinician. An accurate, evidence-based risk assessment that has been sufficiently validated for clinical use must be carried out by clinicians to identify patients who are at greater risk of developing SWCs and therefore may be suitable for ciNPWT.
Following this, a system should be used that is fit for purpose and is able to deliver appropriate clinical management of the incision site throughout the intended period of application.
This meeting report has been supported by an unrestricted educational grant by Mölnlycke Health Care.
References
1. British Orthopaedic Association (2020) Investigation and Management of Prosthetic Joint Infection in Knee Replacement. Available at: https://bit.ly/3L2B2dK (accessed 10.05.2022)
2. ERAS Society (2016) Enhanced Recovery After Surgery. Available at: https://erassociety.org/ (accessed 10.05.2022)
3. Henriksson AS (2021) Single use negative pressure wound therapy (suNPWT) system with controlled fluid management technology — an evaluation of preformance. Wounds International 12(4): 62–8
4. Katzengold R, Topaz M, Gefen A (2018) Dynamic computational simulations for evaluating tissue loads applied by regulated negative pressure-assisted wound therapy (RNPT) system for treating large wounds. J Tissue Viability 27(2): 101–13
5. Leaper D, Tanner J, Kiernan M (2013) Surveillance of surgical site infection. J Hosp Infect 83(2): 83–6
6. Meara JG Leather AJ Hagander L et al (2015) Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet 386(9993): 569–624
7. Morgan-Jones R et al (2019) Incision Care and Dressing Selection in Surgical Wounds: Findings from an International Meeting of Surgeons. London: Wounds International
8. Morgan-Jones R et al (2021a) Incision Care and Dressing Selection in Surgical Wounds: Findings from an International Meeting in the APAC Region. London: Wounds International
9. Morgan-Jones R et al (2021b) Incision Care and Dressing Selection in Surgical Incisions Wounds: Findings from an International Meeting of Surgeons from Northern Europe. London: Wounds International
10. Morgan-Jones R et al (2022) Incision Care and Dressing Selection in Surgical Incision Wounds: Findings from an International Meeting of Surgeons from Eastern Europe. London: Wounds International
11. Orlov A, Gefen A (2022) The potential of a canister-based single-use negative-pressure wound therapy system delivering a greater and continuous absolute pressure level to facilitate better surgical wound care. Int Wound J doi: 10.1111/iwj.13744
12. Parvizi J, Gehrke T, Chen AF (2013) Proceedings of the International Consensus on Periprosthetic Joint Infection. Bone Joint J 95-B (11): 1450–2
13. Sandy-Hodgetts K, Carville K, Leslie GD, Lewin G (2013) Determining risk factors for surgical wound dehiscence: A review of the literature. Int Wound J doi:10.1111/ iwj.12088
14. Sandy-Hodgetts K, Carville K, Leslie GD (2018) Surgical wound dehiscence: a conceptual framework for patient assessment. J Wound Care 27(3): 119–26
15. Sandy-Hodgetts K, Carville K, Santamaria N (2019) The Perth Surgical Wound Dehiscence Risk Assessment Tool (PSWDRAT), development and prospective validation in the clinical setting. J Wound Care 28(6): 332–44
16. Sandy-Hodgetts K et al (2020) International Best Practice Recommendations for the Early Identification and Prevention of Surgical Wound Complications. London: Wounds International. Available online at: www. woundsinternational.com (accessed 10.05.2022)
17. Sandy-Hodgetts K, Cao L, Doozhang C, Hyun LS et al (2021) Post-surgical incision care across the Asia Pacific; current perceptions and practice. Wounds International 12(3): 63–9
18. World Health Organization (2016) Global Guidelines on the Prevention of Surgical Site Infection. Available at: https:// www.who.int/gpsc/ssi-prevention-guidelines/en/ (accessed 10.05.2022)
19. World Union of Wound Healing Societies (2016) Consensus Document. Closed Surgical Incision Management: Understanding the Role of NPWT. London: Wounds International. Available at: www.woundsinternational. com (accessed 10.05.2022)
This article is excerpted from the Wounds International 2022 | Vol 13 Issue 2 by Wound World.

