
伤口世界
电子邮件地址: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。
- 星期二, 13 1月 2026
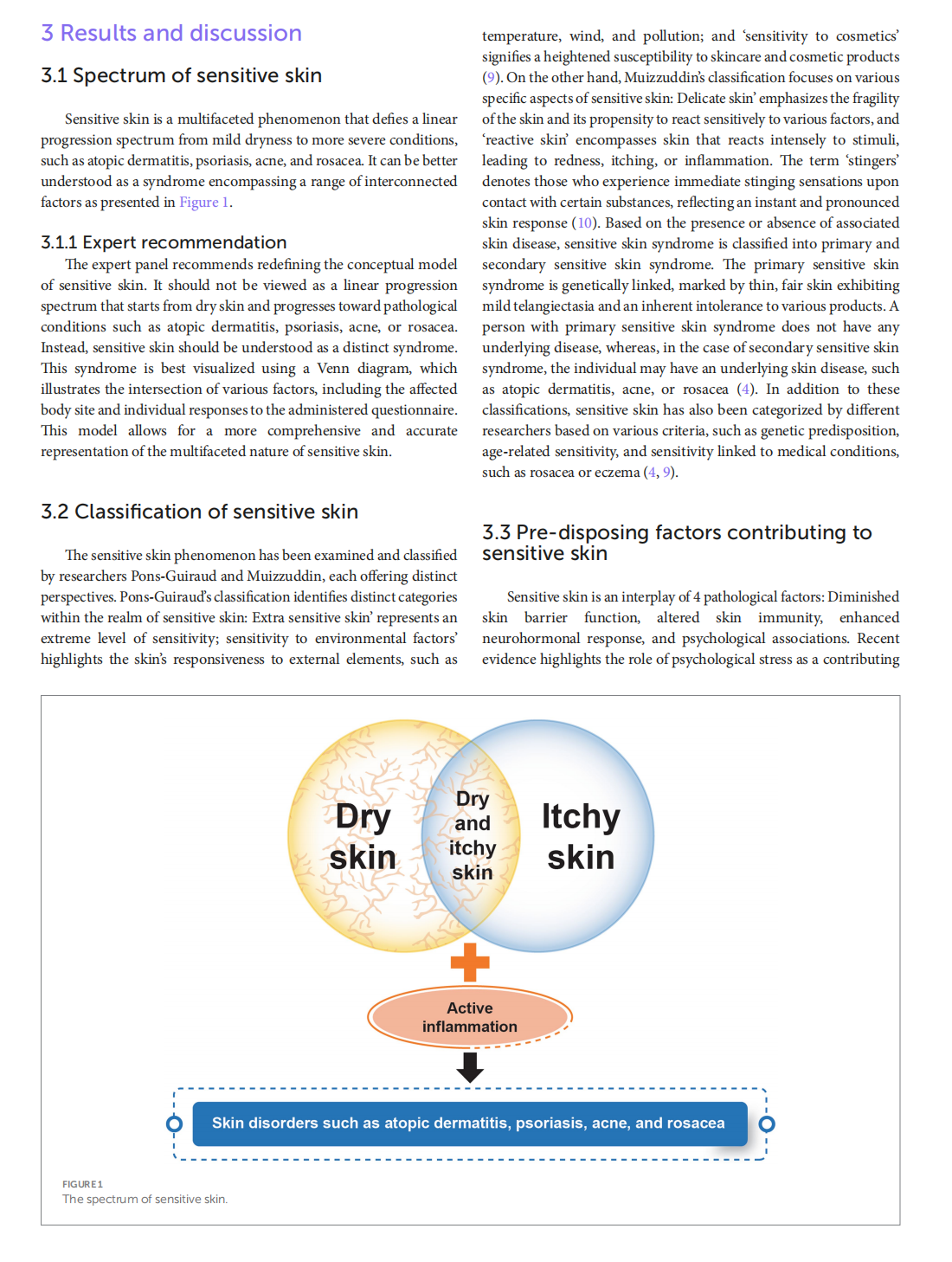
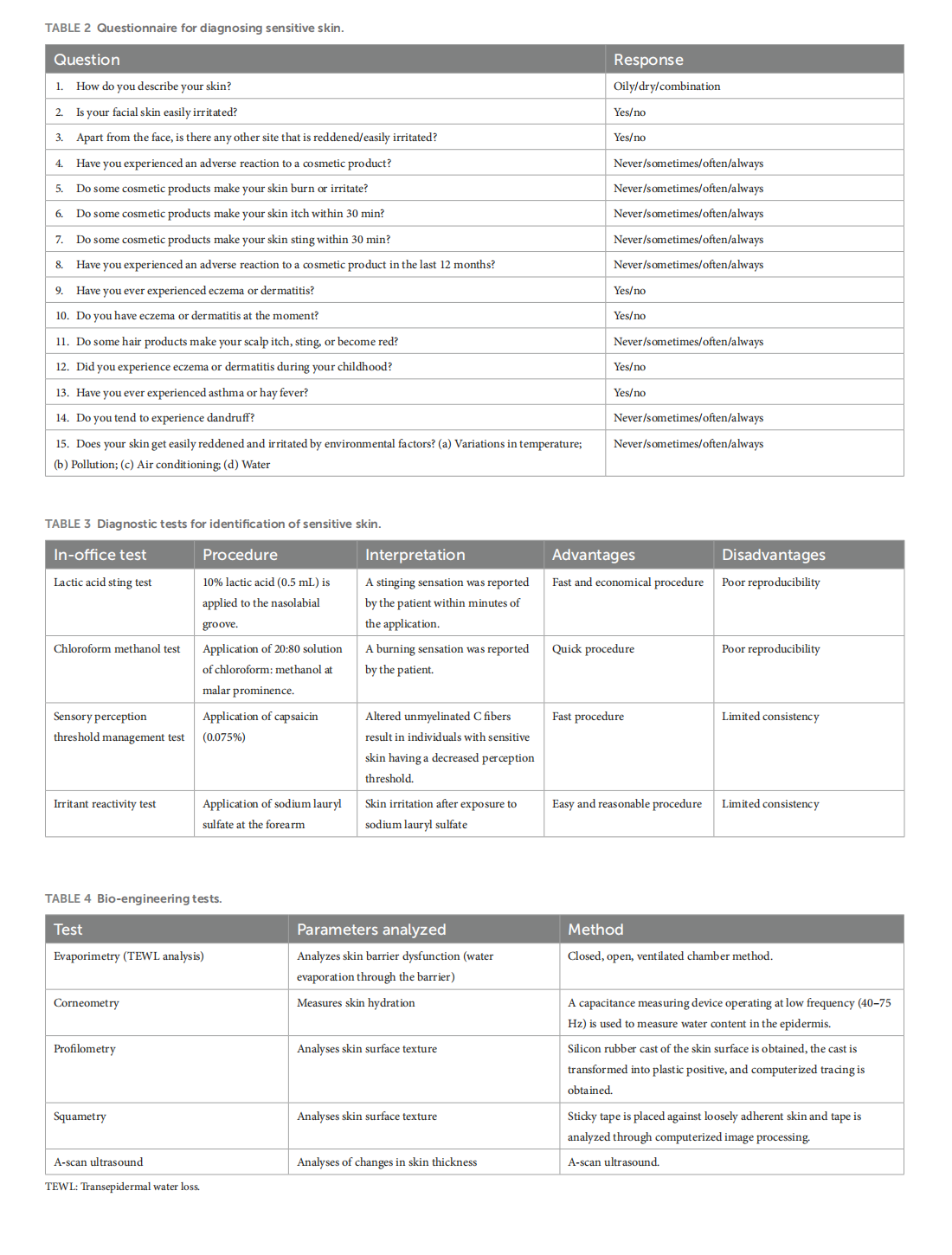
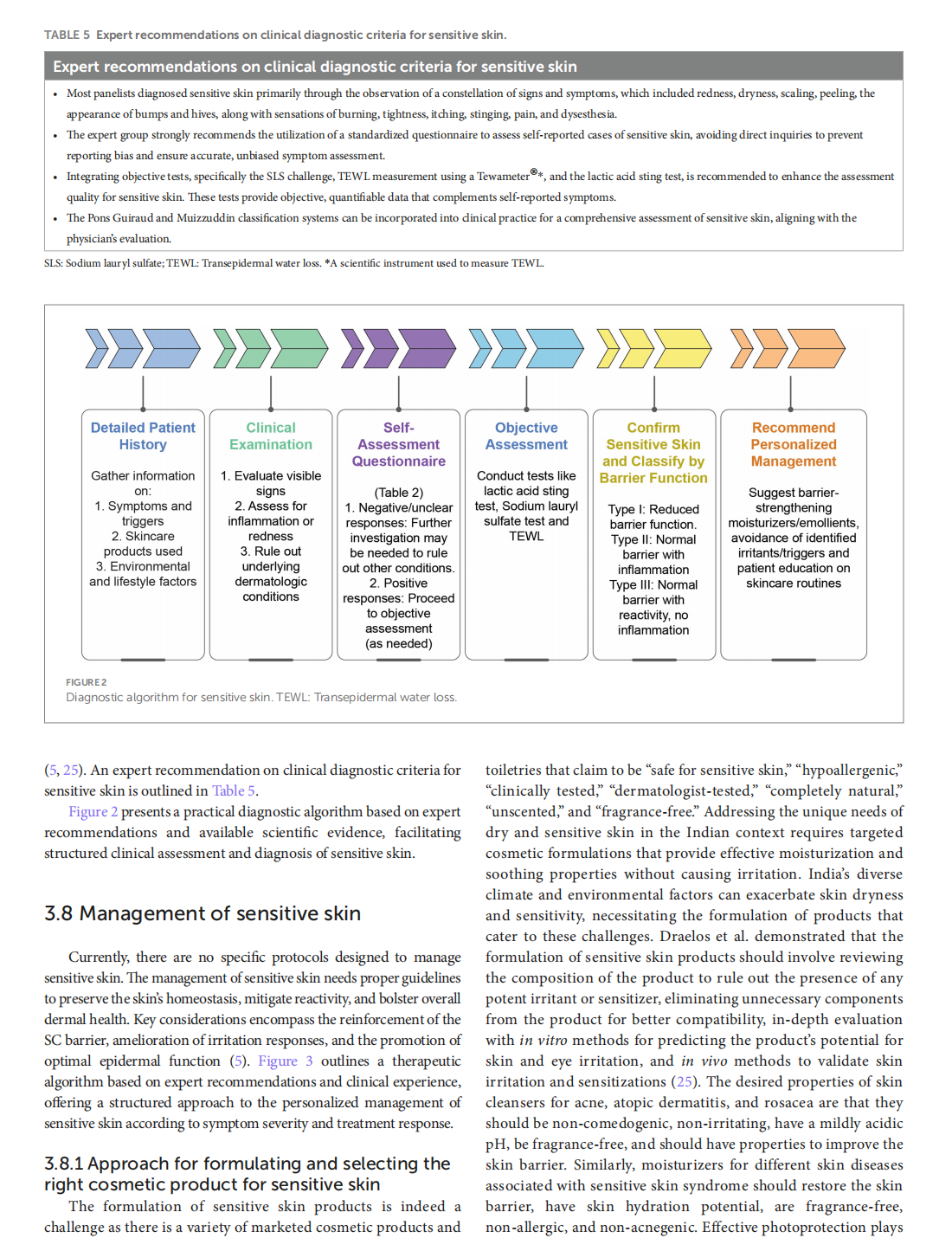
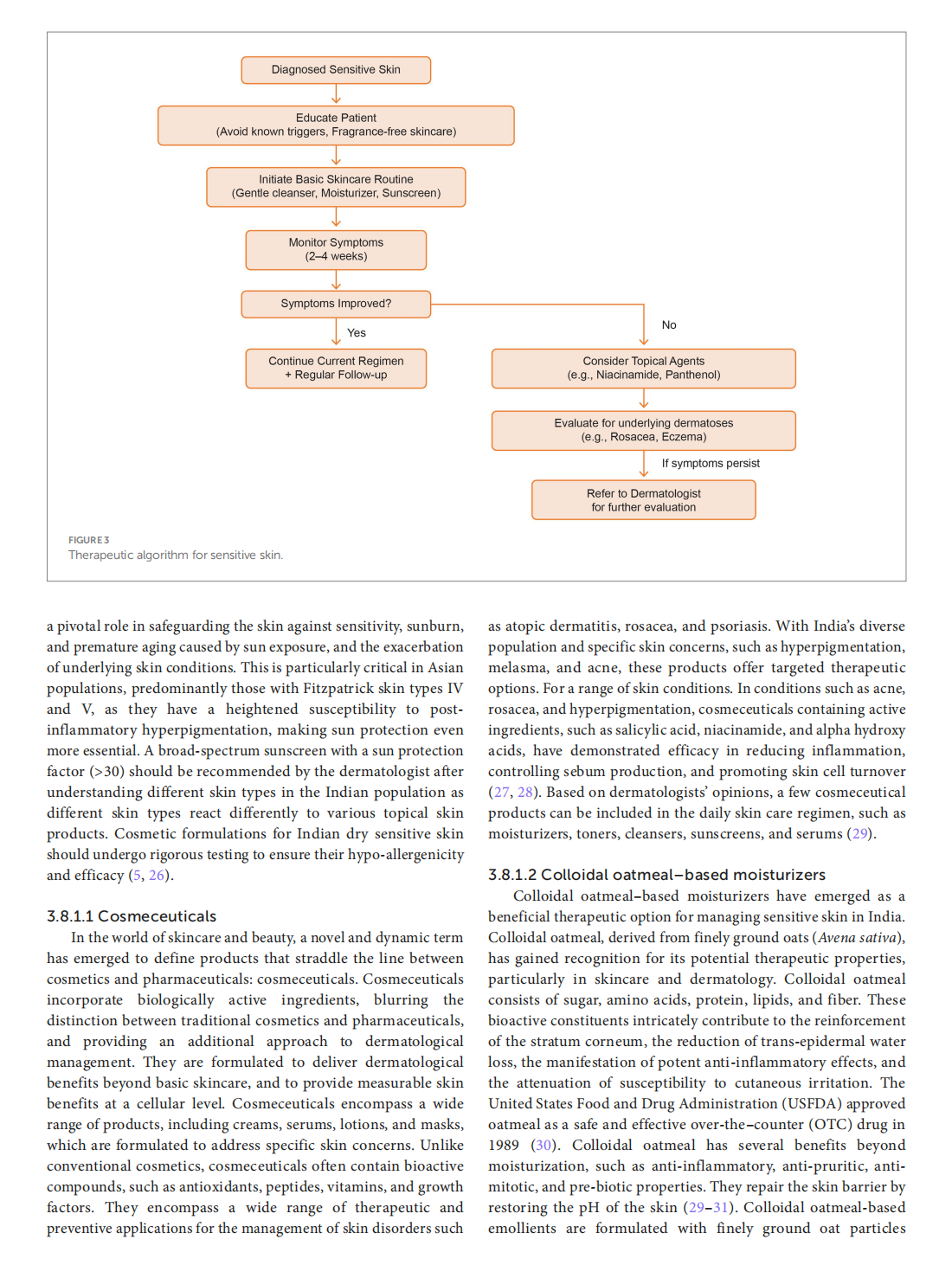
Spectrum of sensitive skin in India: a collaborative expert position statement




This article is excerpted from the 《Frontiers in Medicine》 by Wound World

- 星期一, 12 1月 2026
Medical Cannabis for the Treatment of Migraine in Adults: A Review of the Evidence



This article is excerpted from the《Frontiers in Neurology》by Wound World

- 星期五, 09 1月 2026
Integrative population pharmacokinetic/ pharmacodynamic analysis of nemonoxacin capsule in Chinese patients with community-acquired pneumonia


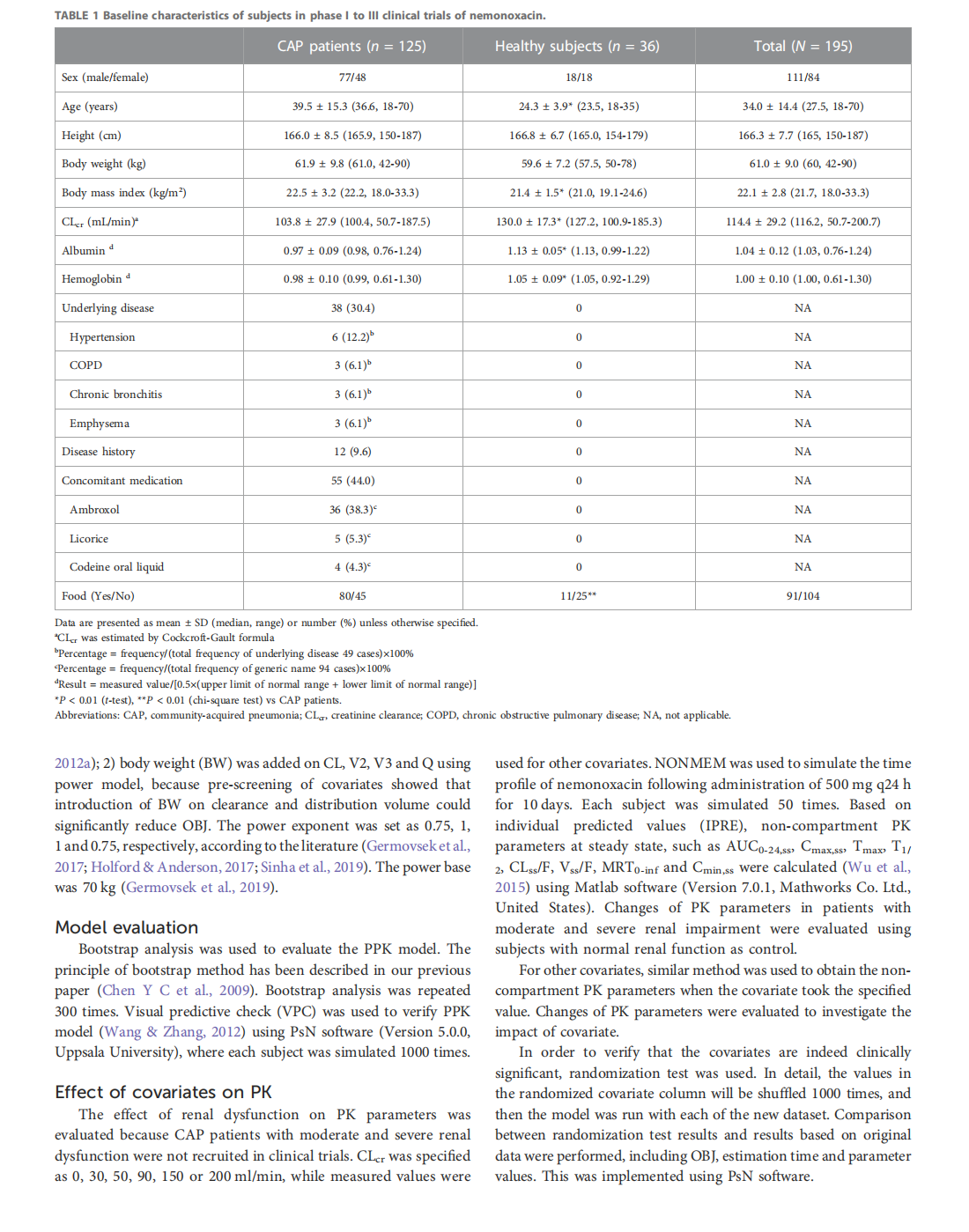
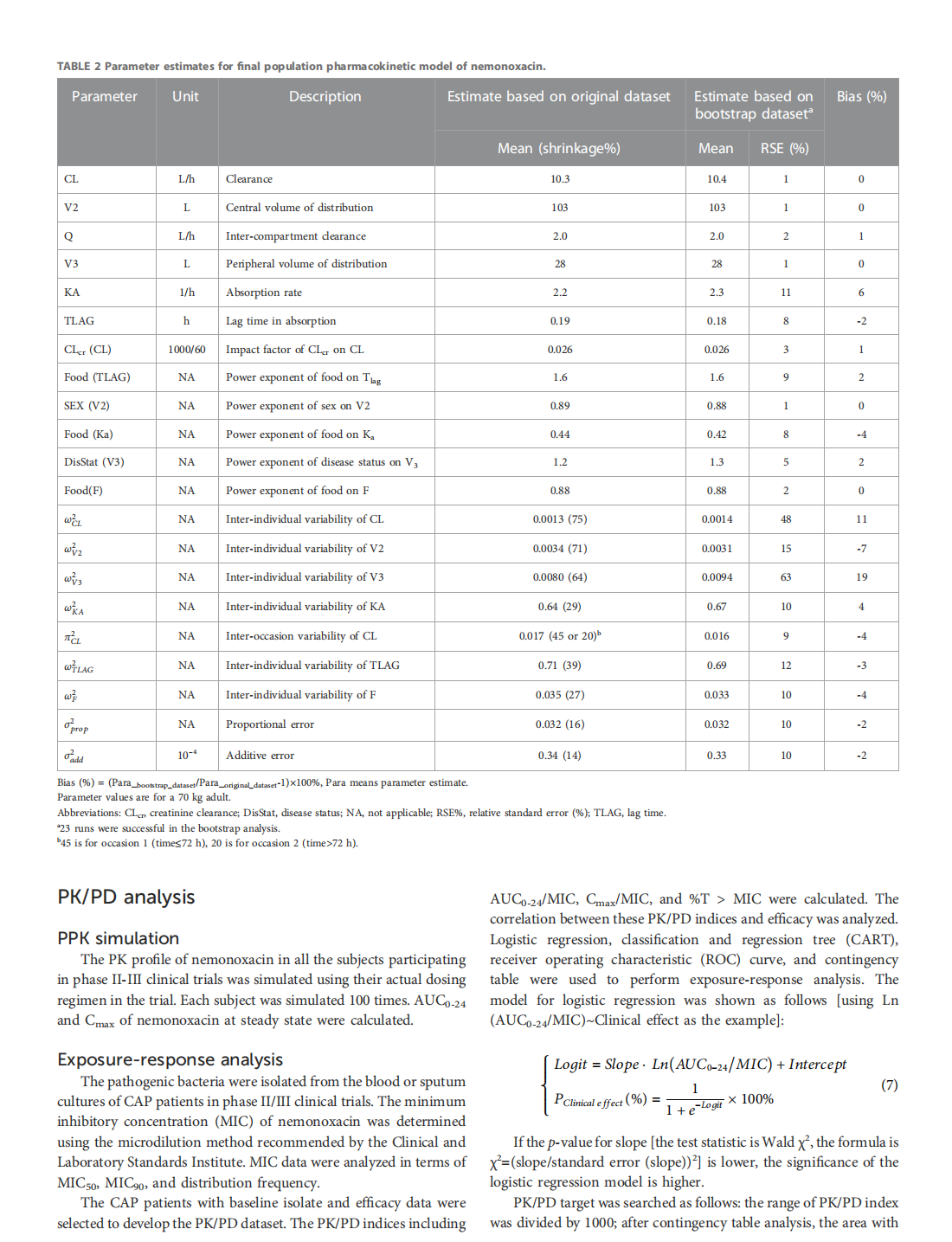

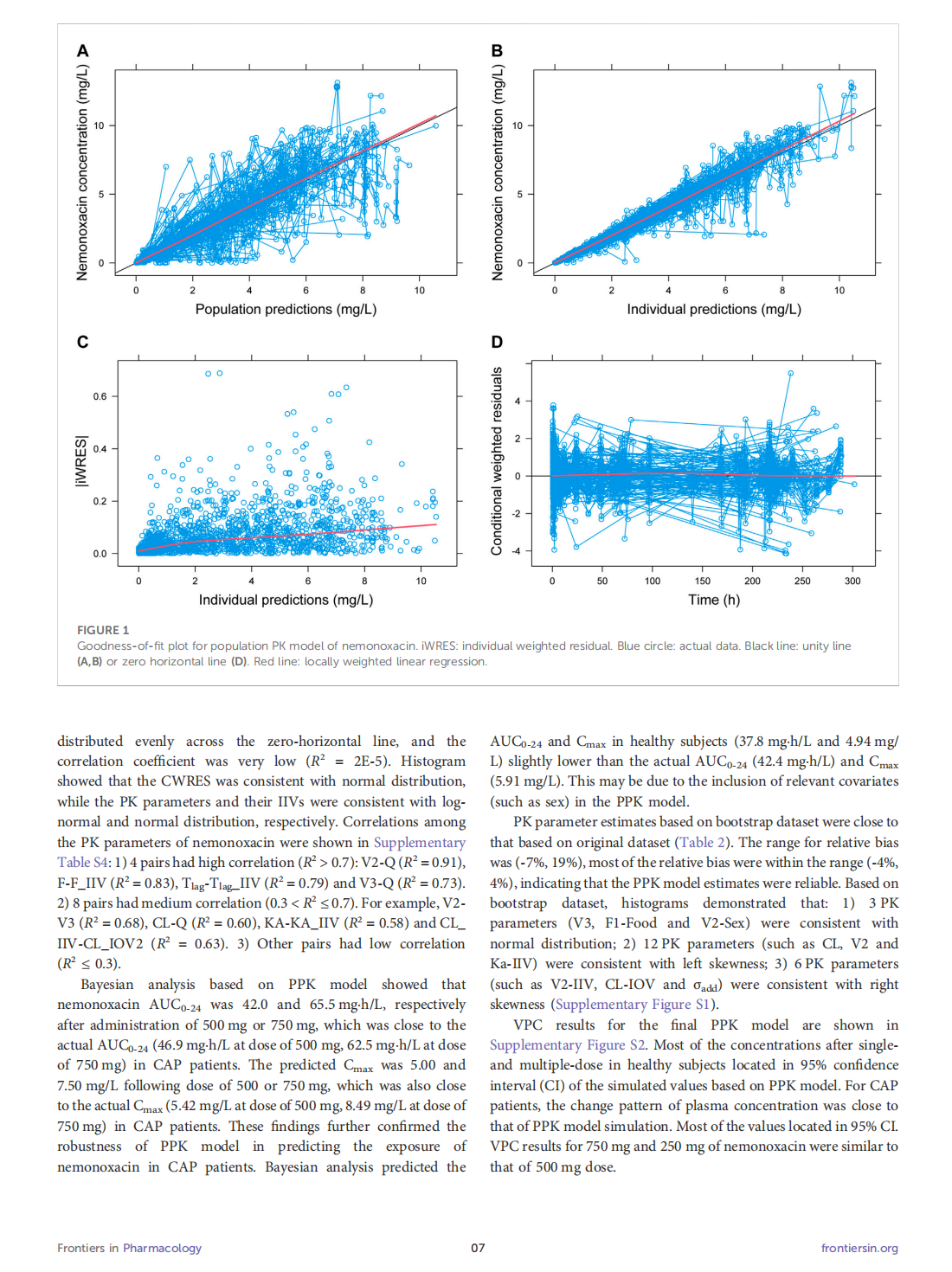

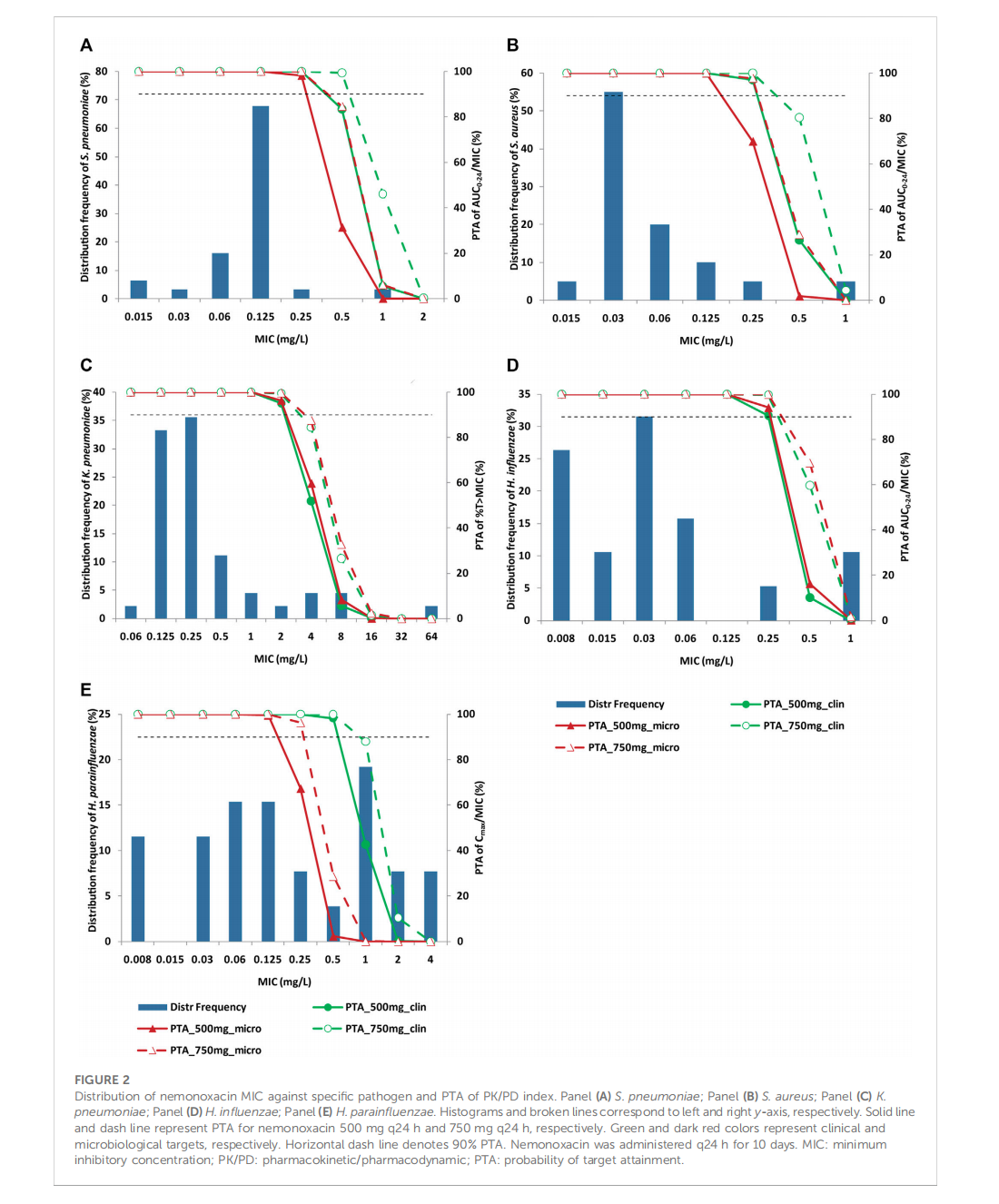
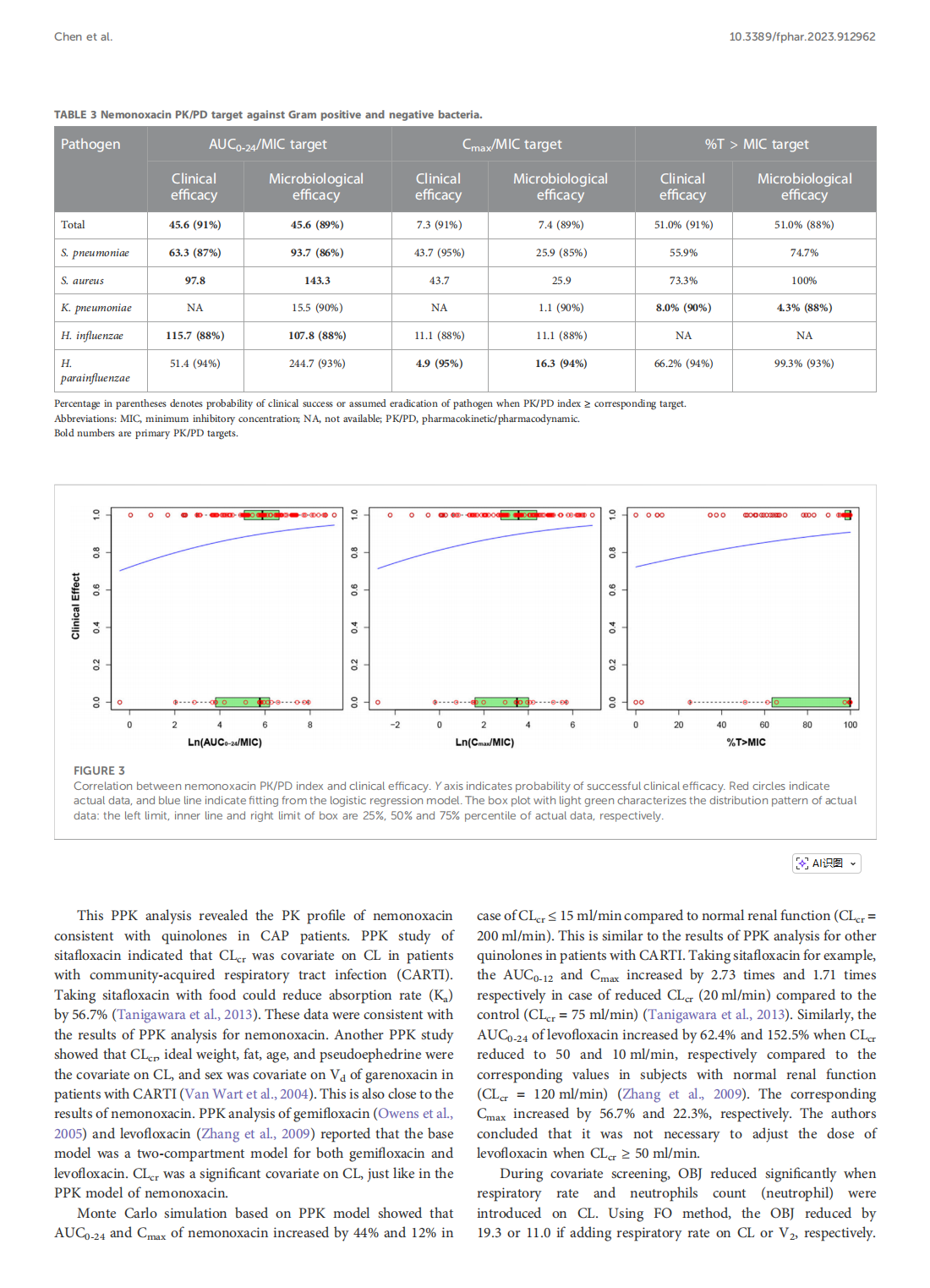
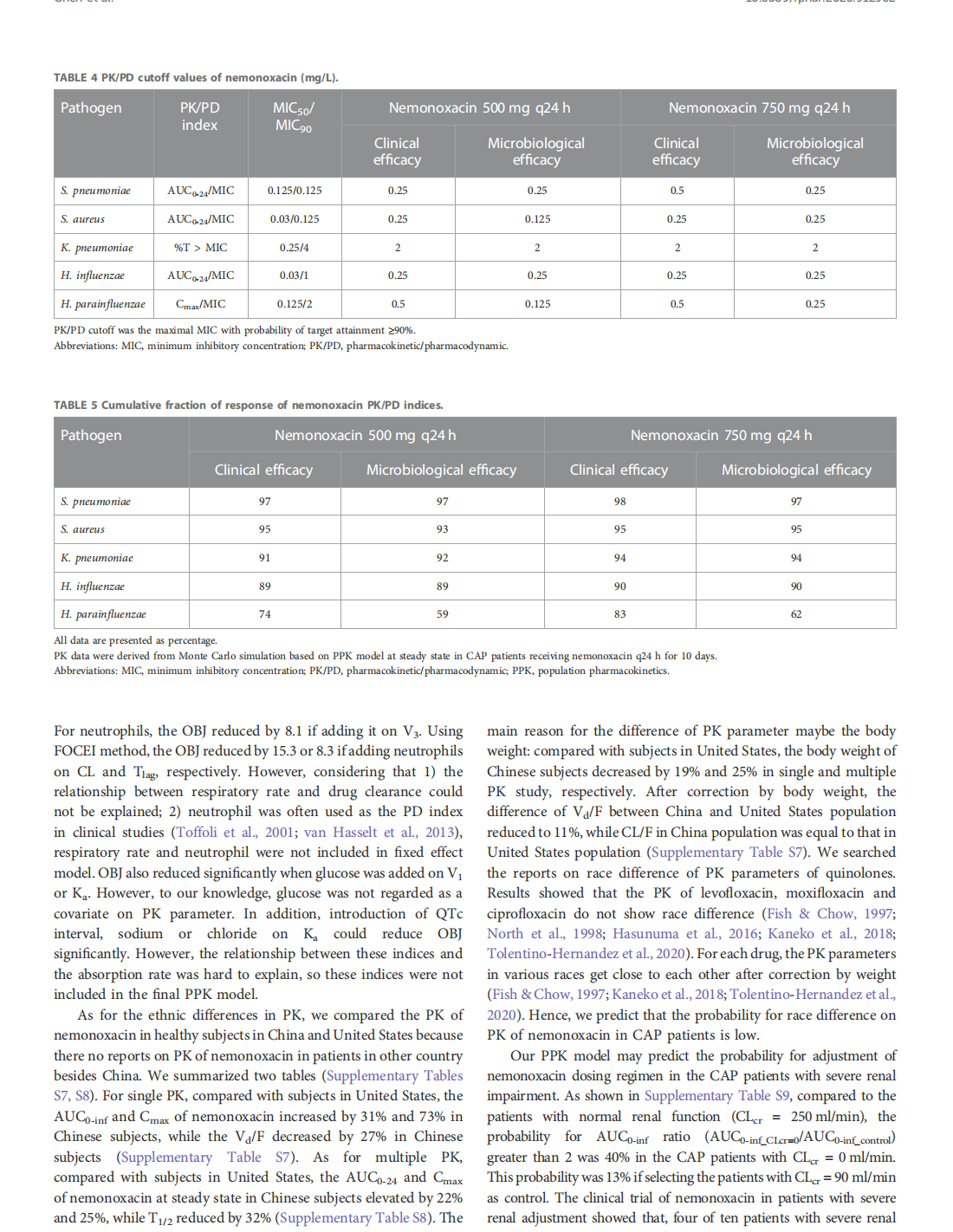


This article is excerpted from the《Frontiers in Pharmacology》by Wound World

- 星期四, 08 1月 2026
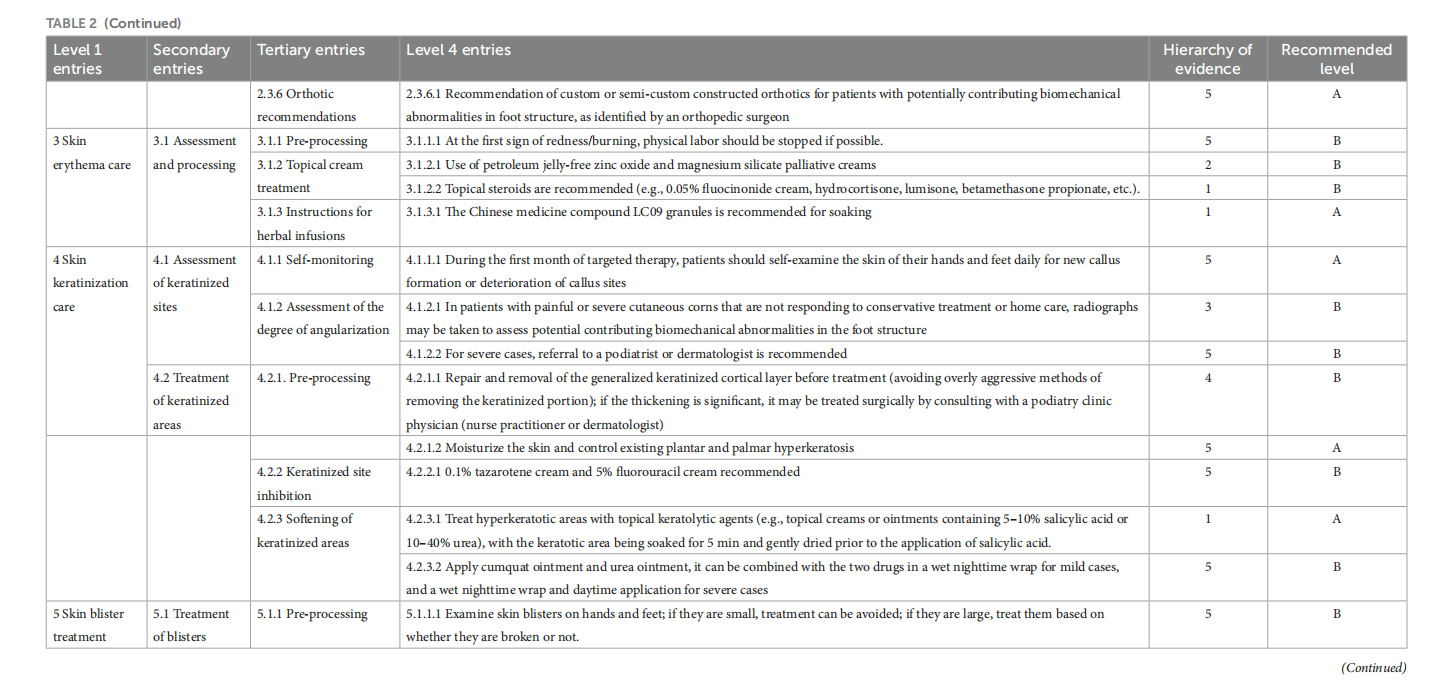
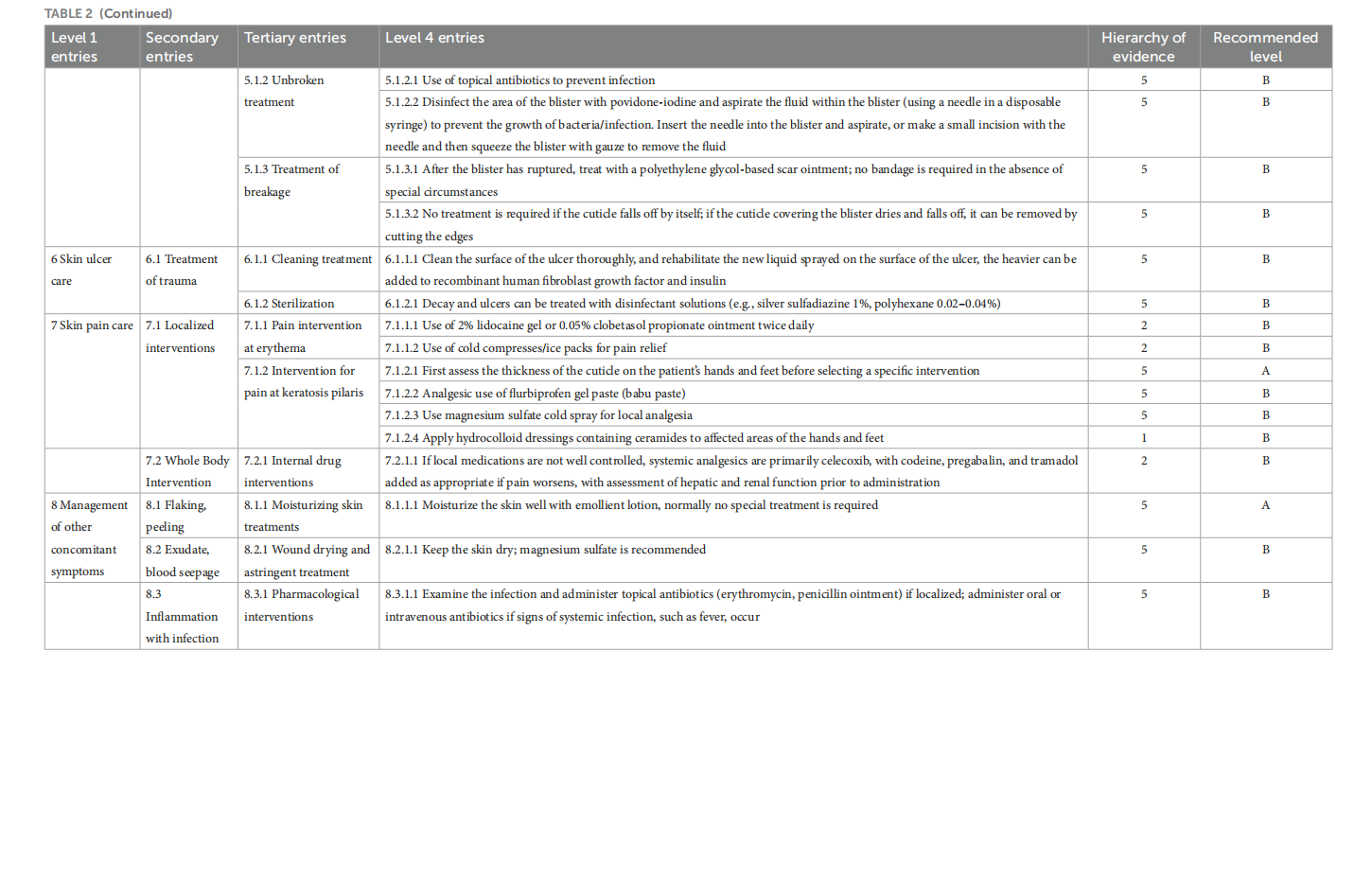
Construction of a management and prevention program for targeted therapy-induced hand-foot skin reaction
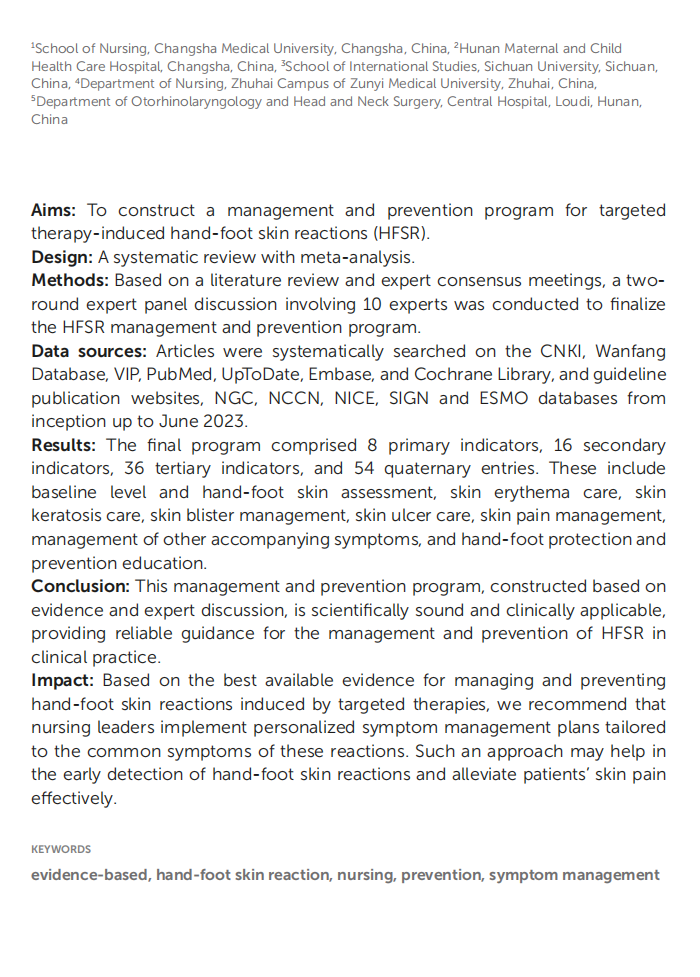


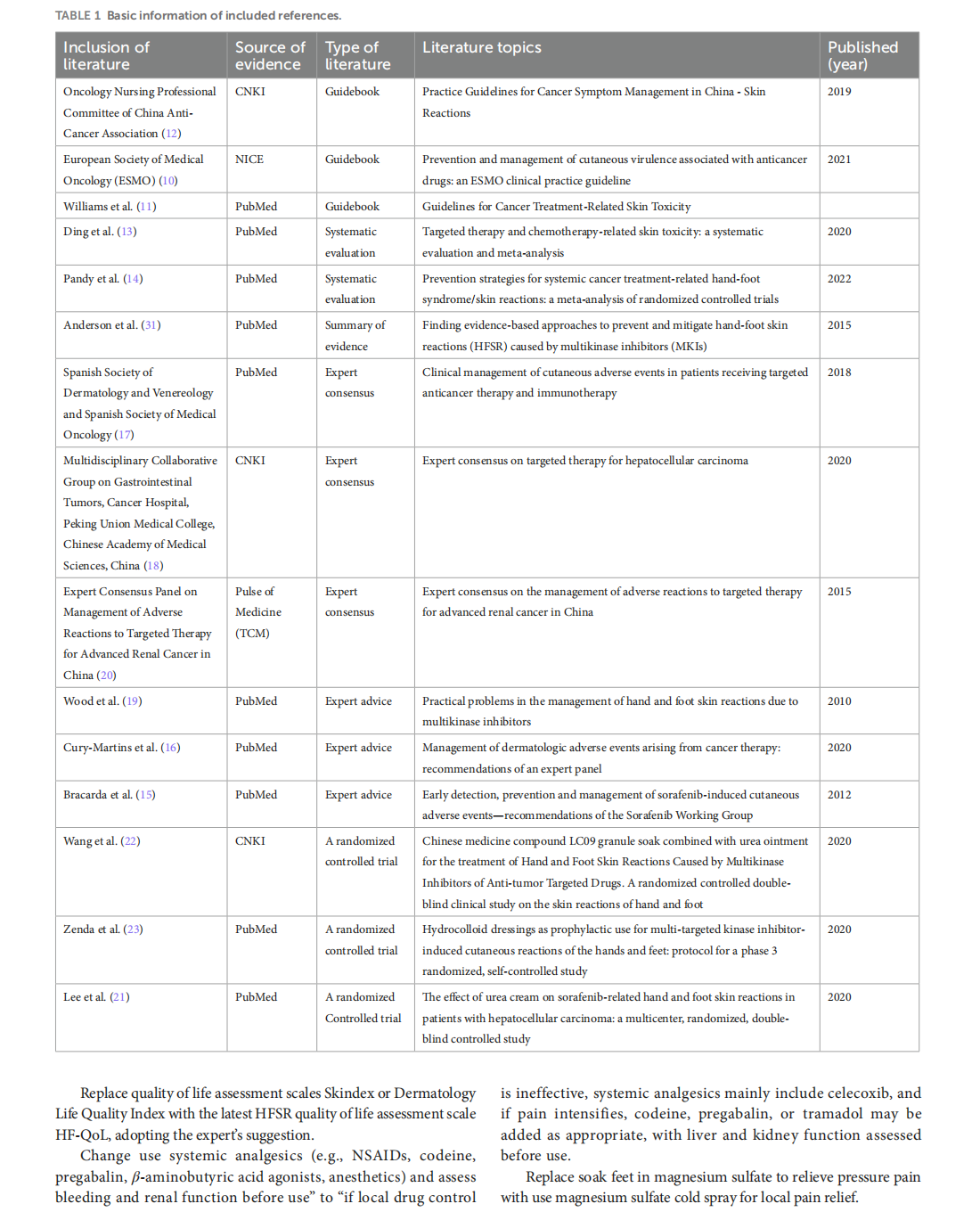




This article is excerpted from the《Frontiers in Oncology》by Wound World

- 星期三, 07 1月 2026
Multi-omic approach to decipher the impact of skincare products with pre/postbiotics on skin microbiome and metabolome

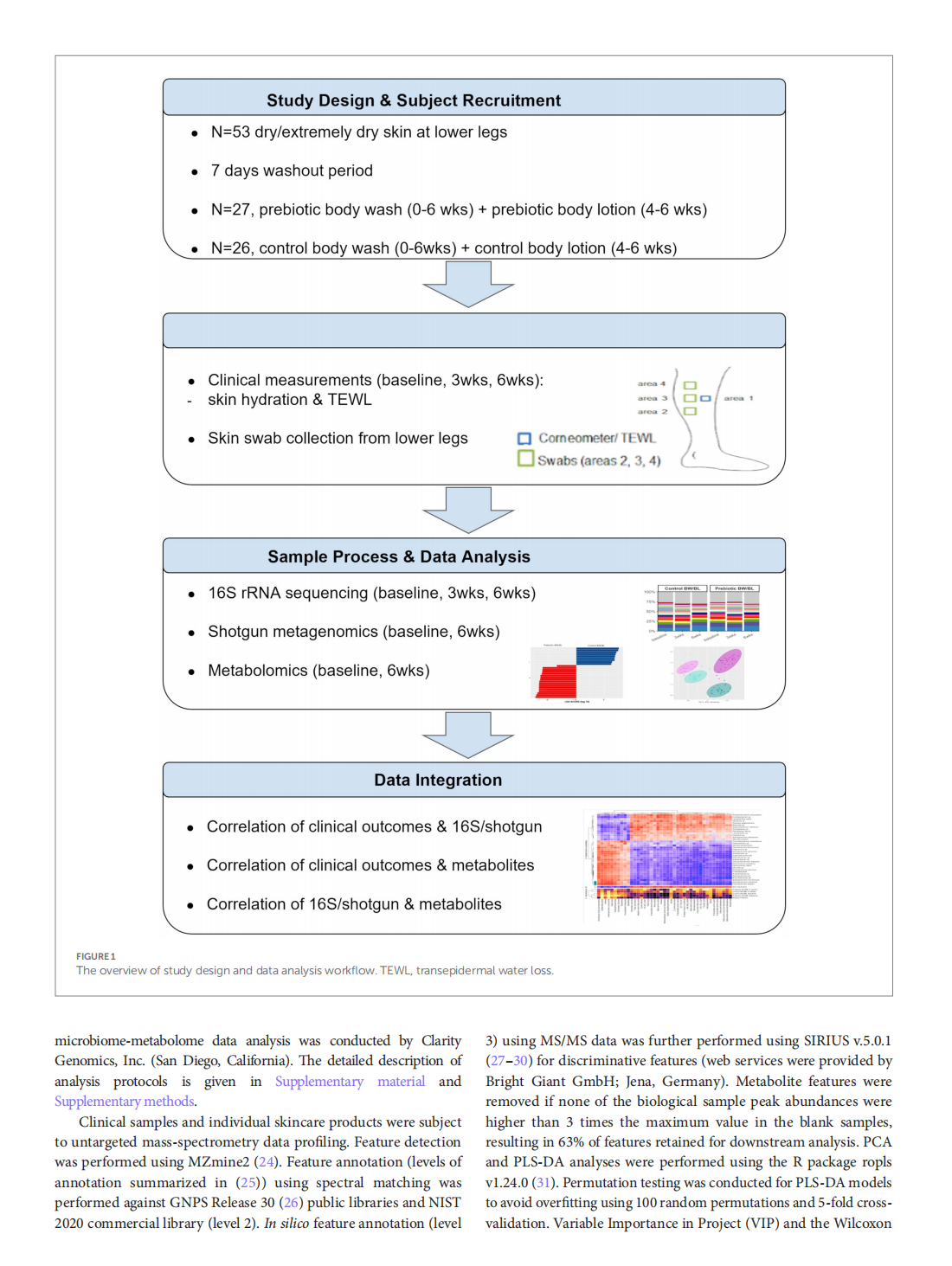
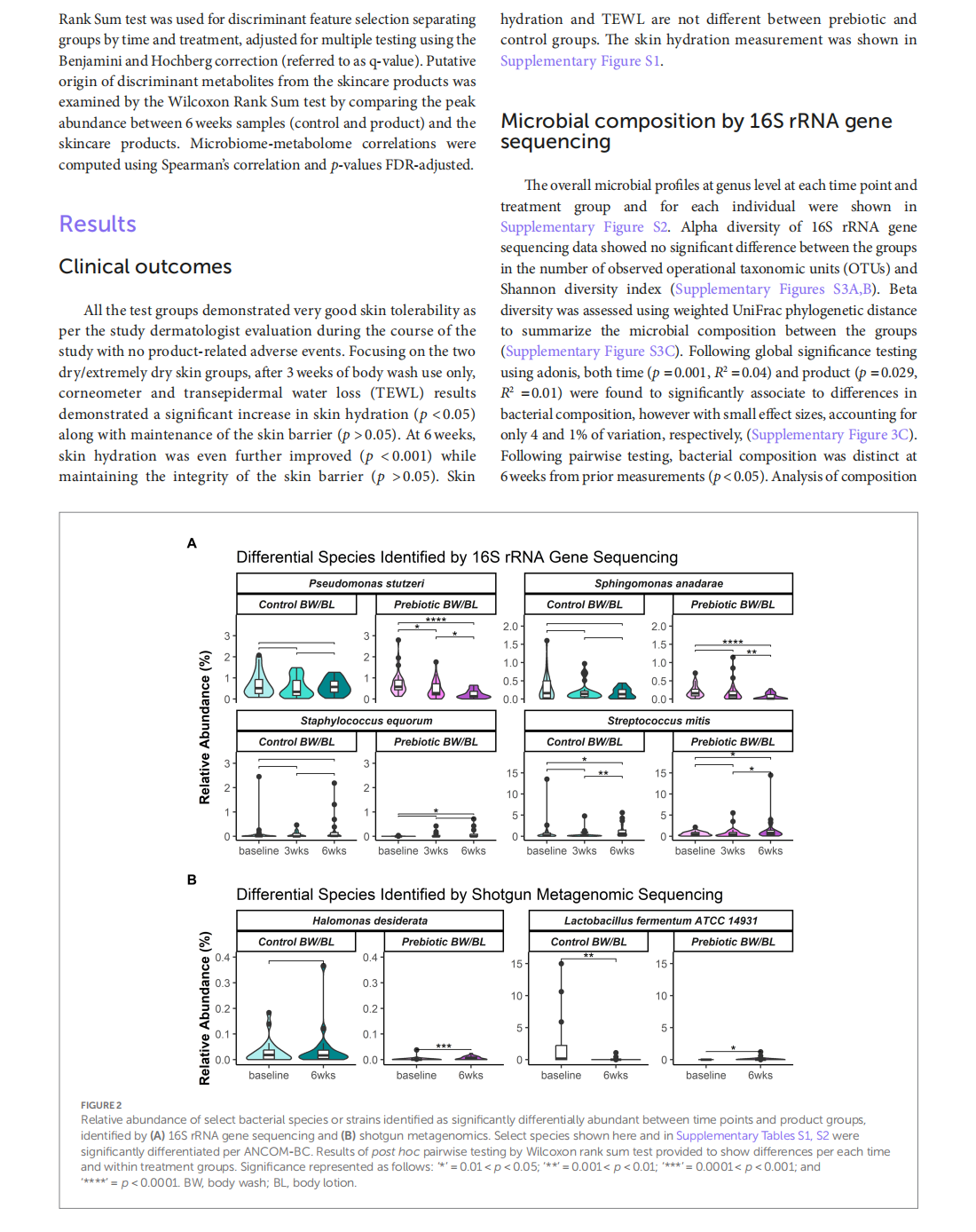
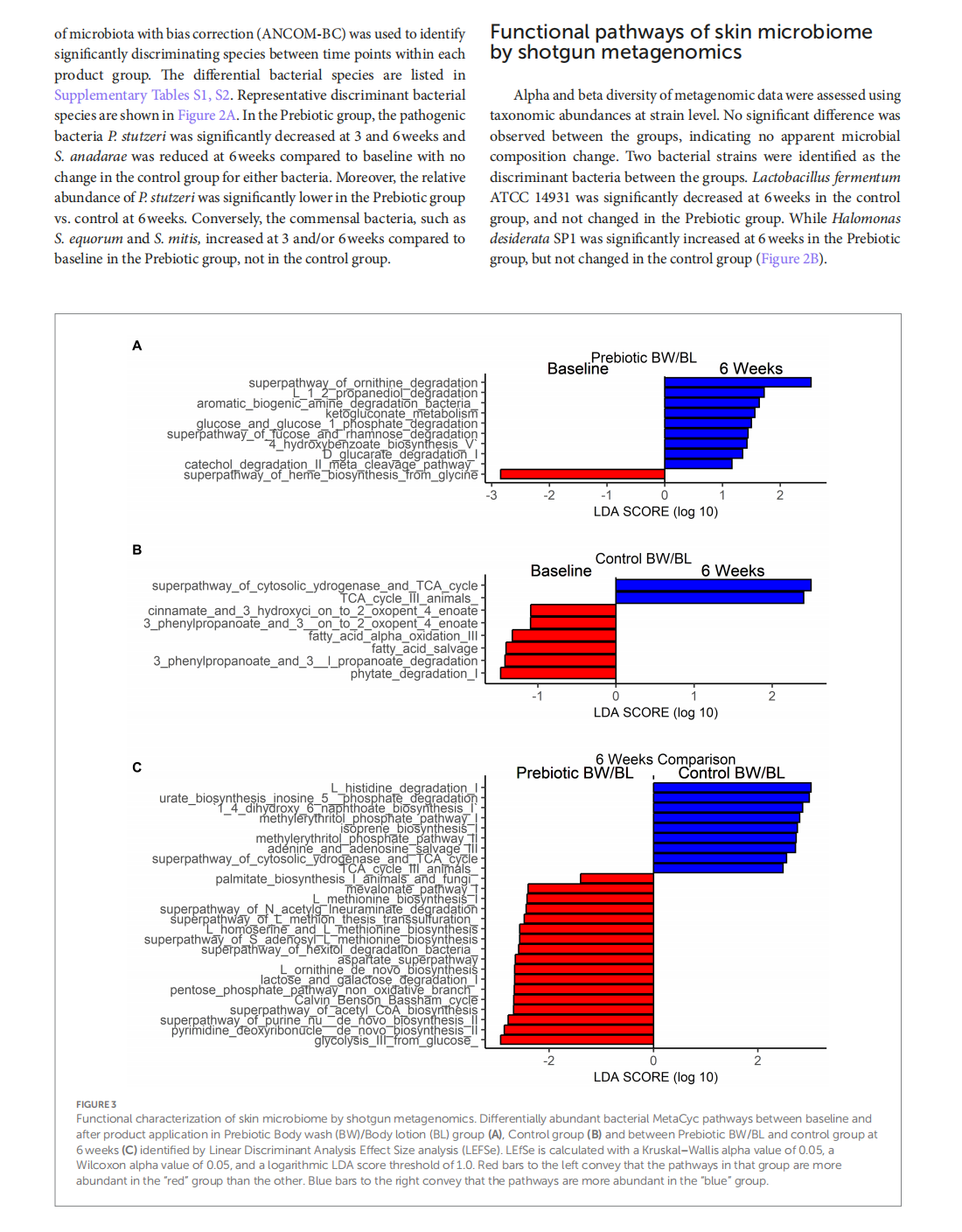

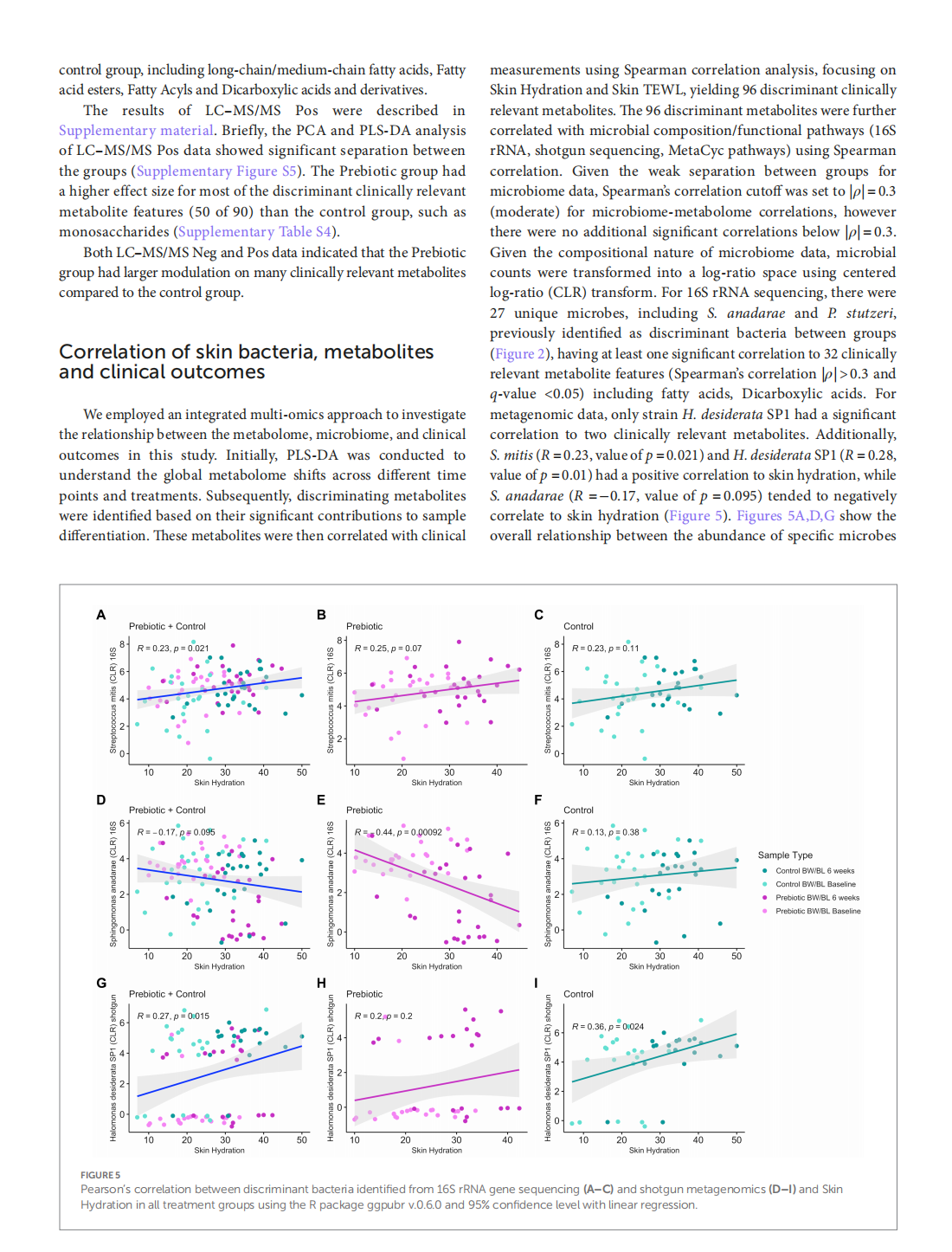
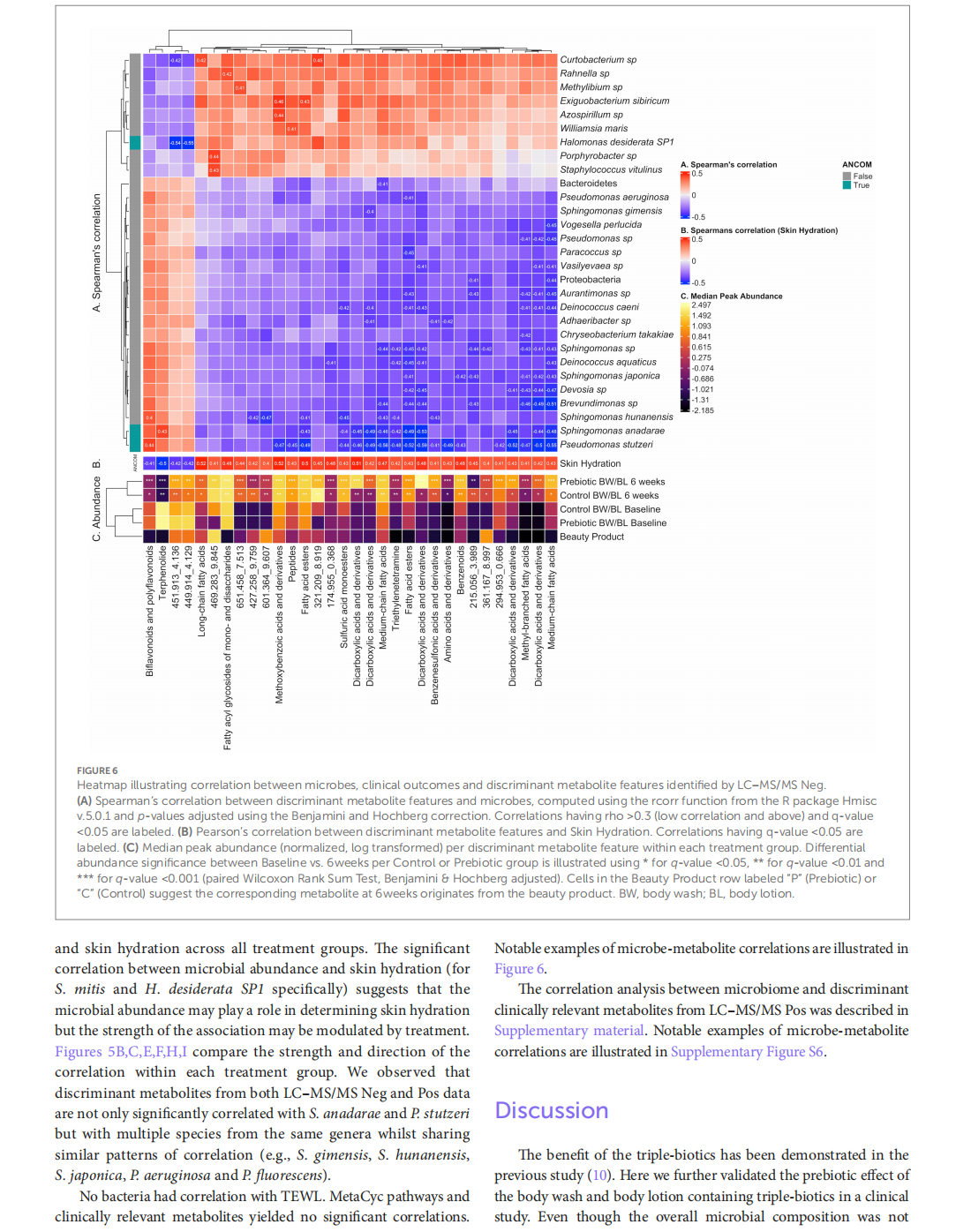


This article is excerpted from the《Frontiers in Medicine》by Wound World

- 星期二, 06 1月 2026
Genetic profiling and precision skin care: a review


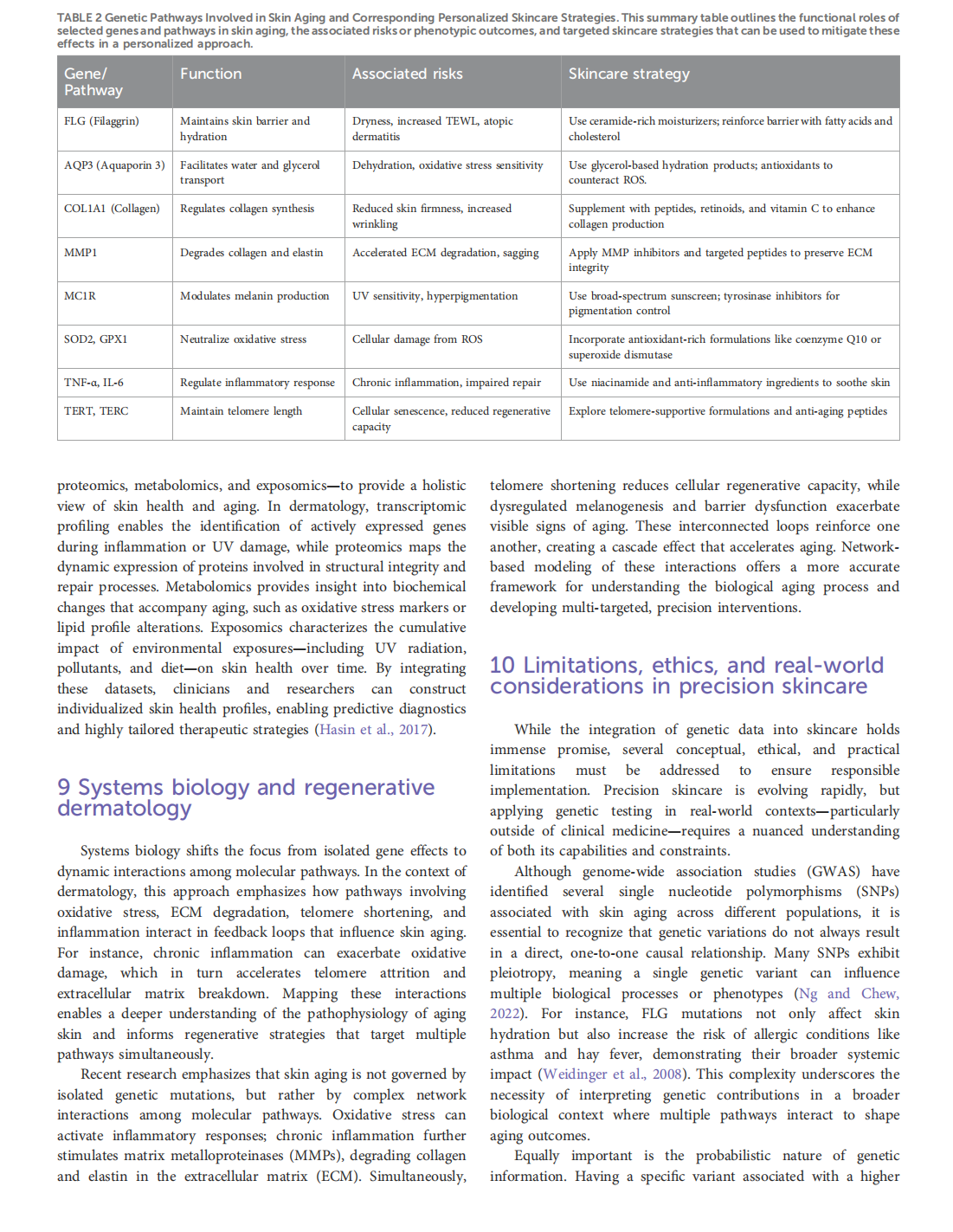


This article is excerpted from the《Frontiers in Genetics》by Wound World

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}