
Introduction
In recent years, with improvements in living standards and a significant extension of life expectancy, the incidence of dia-betes mellitus (DM) has risen sharply, ranking eighth on the global burden of disease list [1]. It profoundly affects hun-dreds of millions of people worldwide and is often accompa-nied by various severe complications, posing a considerable challenge to the global health system. Among them, diabetic foot (DF) is a severe and chronic complication of diabetes, and its pathogenesis involves decreased protective func-tion of the lower extremities due to neuropathy, as well as microcirculatory disturbances caused by "macrovascular" and microvascular diseases. Early symptoms may include numbness, chills, and abnormal sensations, and may even lead to infection, osteomyelitis, and necrosis. It is predicted that by 2045, the number of people with diabetes worldwide will reach 700 million [2], of whom 19–34% may develop foot ulcers [3]. Among the over 60 million people with dia-betes in China, a quarter face the threat of kidney disease. Moreover, traditional treatments have limited effectiveness, leading to amputation in at least 30–40% of patients. This imposes a heavy burden on both patients and the healthcare system. The current research status of diabetic foot risk pre-diction models shows a significant trend towards diversi-fication and in-depth development. Currently, the research methods for diabetic foot risk prediction models include mainly statistical methods, machine learning methods, and deep learning methods. These methods collect and analyse various factors related to the risk of diabetic foot to con-struct prediction models, aiming to achieve accurate predic-tion of diabetic foot risk.
Statistical methods for diabetic foot risk prediction involve various statistical techniques and models to anal-yse and predict the risk of developing diabetic foot in dia-betic patients. These methods typically include steps such as descriptive statistics, univariate analysis, multivariate analysis, and prediction model construction. Descriptive statistics is the first step in data analysis. It is used to sum-marize and describe the basic characteristics of the data,such as age, gender, disease duration, blood glucose con-trol, and complications, thereby providing a foundation for subsequent analyses. Univariate analysis is used to explore the association between a single factor and the risk of dia-betic foot. Common methods include the chi-square test or t-test. Through this step, factors such as gender, age, disease duration, fasting blood glucose, and glycated hemoglobin that may be related to the risk of diabetic foot can be identi-fied. However, since the development of diabetic foot often involves the interaction of multiple factors, multivariate analysis is required, with logistic regression being the most commonly used method. The model is capable of handling binary or multicategory dependent variables, assessing the strength and direction of the impact of each independent variable on the dependent variable, thereby identifying the independent risk factors for diabetic foot. Finally, based on the identified independent risk factors, a predictive model is constructed to assess the risk of diabetic foot in patients. This process includes model training, validation, and evalu-ation, with the aim of ensuring the accuracy and reliability of the prediction results.
Machine learning (ML) and deep learning (DL) algo-rithms have been widely applied in the medical field. Artificial intelligence-based technologies are data driven, meaning that they make decisions on the basis of information in databases and have been used for diagnosing diabetes [4, 5]. Machine learning models such as Support Vector Machine (SVM), Random Forest (RF), and Logistic Regression (LR) can be used. These models are capable of handling various types of clinical data, including patients’ medical history, physiological indicators (such as blood glu-cose levels, blood pressure, etc.), and laboratory test results [6]. For example, Heald et al. (2019) successfully devel-oped a risk prediction model for diabetic foot ulcers using a univariate logistic regression model with predictors such as HbA1c, age, loss of monofilament sensation, creatinine levels, and history of stroke [7]. In terms of data sources, theapplication of machine learning models relies extensively on various types of information, among which electronic health records (EHR), medical imaging data, and biomarker test results are the most critical. These data sources provide the models with rich and comprehensive patient informa-tion. Some studies have delved deeply into and fully utilized patients’ medical history data, such as the duration of dia-betes, detailed records of whether foot ulcers have occurred in the past, and key physiological indicators, such as body mass index (BMI) and glycated hemoglobin (HbA1c) levels, as input features for constructing machine learning models. The selection of these features is aimed at improving the predictive accuracy and reliability of the models, thereby providing strong support for clinical decision-making. Deep learning algorithms are capable of directly extracting fea-tures from input data, thereby generating accurate predic-tions. Deep learning models, such as Convolutional Neural Networks (CNNs), can be used to analyze medical imaging data, such as foot X-rays and ultrasound images, to identify potential risks of diabetic foot ulcers [8]. For example, by analyzing images of the foot vasculature, CNNs can detect vascular lesions, thereby predicting the risk of diabetic foot ulcers [9].
It is crucial to identify patients at high risk of diabetic foot at an early stage and to take corresponding preventive and therapeutic measures. Diabetic foot risk prediction models serve as important tools for assessing patients’ risk of devel-oping diabetic foot. The technical methods can be divided into three main categories: statistical methods, machine learning methods, and deep learning methods. Statistical methods, such as logistic regression and Cox proportional hazards models, establish risk prediction models by analys-ing the statistical patterns in patient data. Machine learning algorithms, on the other hand, can automatically learn and extract features from large amounts of data to build more complex prediction models. The application of deep learn-ing technology in diabetic foot risk prediction can further improve prediction accuracy. Through model prediction, medical staff can identify high-risk patients for diabetic foot early and take corresponding preventive and therapeutic measures, thereby effectively reducing the incidence of dia-betic foot. Additionally, the model can provide a scientific basis for the personalized health management of patients, helping them better control their condition.
Methods
Search strategy
When searching for articles, we used the following Eng-lish search terms: “Diabetic Foot,” “Diabetic Foot Ulcer,” “Prediction Model,” “Risk Prediction Model,” “Risk Pre-diction,” “Risk Factors,” “Risk Assessment,” “Prognostic Model,” “Risk Score,” and “Prediction Tool.” We conducted computer-based searches in PubMed, the Cochrane Library, Embase, CNKI (China National Knowledge Infrastructure), VIP (China Science and Technology Journal Database), and Wanfang Data for relevant literature on diabetic foot risk prediction models. The searches combined subject terms with keywords. Additionally, we manually searched the ref-erences of the included articles. The search period was from December 12, 2019, to September 9, 2024, and the search language was limited to English.
Literature screening process and results
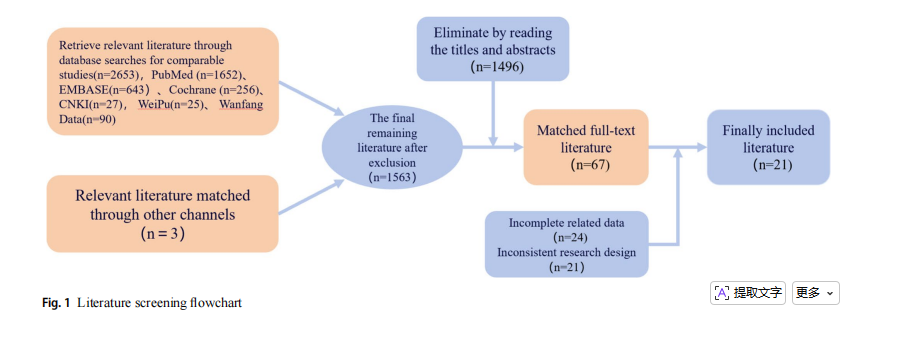
The literature screening process is shown in Fig. 1. A total of 2,653 relevant articles were retrieved from the PubMed, EMBASE, Cochrane, CNKI, VIP, and Wanfang databases. By focusing on whether the articles contained keywords or phrases such as “diabetic foot,” “risk prediction model,” “predictors,” “risk “assessment”,” etc., we quickly identi-fied articles related to diabetic foot risk prediction models. After excluding irrelevant articles, 1,563 articles remained. By reading the titles and abstracts of each article, we used the exclusion function to remove 1,496 articles, leaving 67 full-text articles. We then read the full texts of the candi-date articles one by one, paying attention to whether they described in detail the construction process of the diabetic foot risk prediction model, the selection of predictors, the validation and evaluation of the model, and other key infor-mation. On the basis of the research content, purpose, and conclusions of the articles, we assessed their relevance to the research topic and excluded 49 articles. After a com-bination of initial broad screening and subsequent detailed screening, a total of 21 articles were ultimately included.
Statistical methods
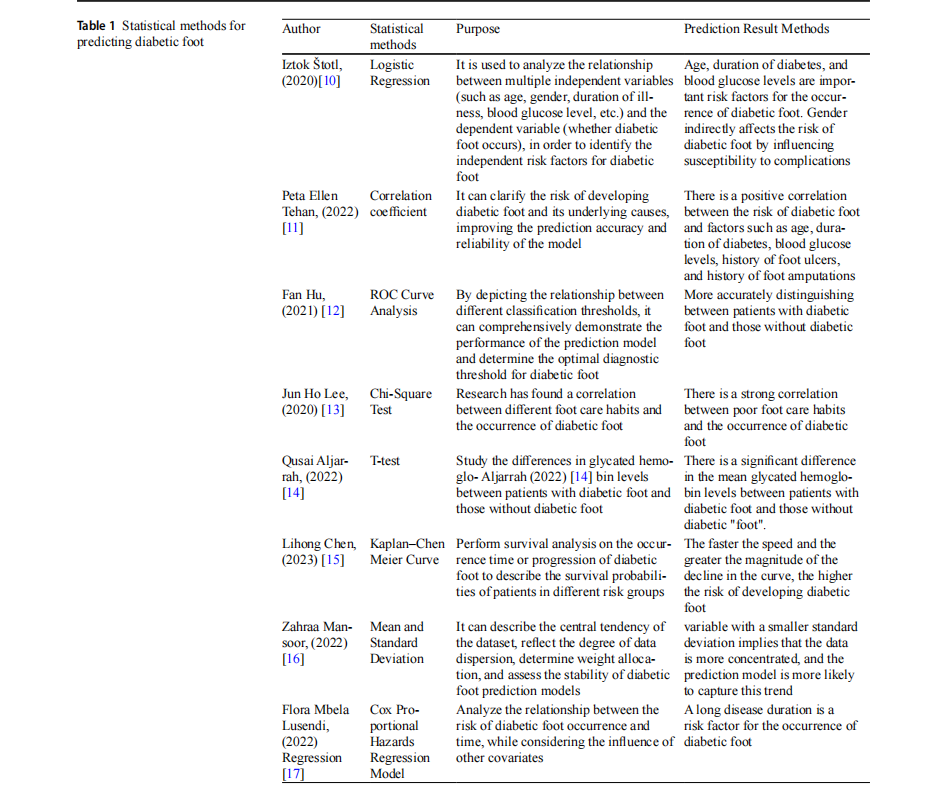
Statistical methods, as classic data analysis tools, continue to occupy an important position in predicting the risk of diabetic foot. By collecting patients’ clinical data, including age, sex, duration of disease, blood glucose levels, smok-ing habits, neurovascular disease status, and other factors, researchers have employed statistical methods such as logistic regression and the Cox proportional hazards model to analyse the associations between these factors and the risk of diabetic foot disease. On the basis of these analyses, they constructed prediction models. The common statisti-cal methods and their applications in predicting the risk of diabetic foot have been summarized in Table 1 for further research and application. These models can provide quanti-tative assessments of the risk of diabetic foot on the basis of individual patient characteristics.
Statistical methods hold a pioneering position in the field of diabetic foot risk prediction, as they are the first to analyse the clinical data of diabetic patients in depth and identify multiple key factors closely associated with the risk of diabetic foot. On the basis of these core factors, predic-tion models have been constructed. Among them, a logistic regression model, as a classic representative, can effec-tively integrate variables such as the patient’s age, gender, duration of disease, blood glucose levels, smoking habits,
and neurovascular disease status to accurately assess the patient’s risk of developing diabetic foot. Notably, existing research has revealed a potential association between age and the recurrence of diabetic foot ulcers (DFUs), despite heterogeneity due to varying age stratification criteria [18,19]. Additionally, smoking, another critical risk factor, has been confirmed by multiple studies to significantly increase the recurrence rate of DFUs, with consistent conclusions [20, 21]. Gender differences in diabetes and its complica-tions have also been widely discussed. In general, the inci-dence of diabetes is greater in men than in women, especially among middle-aged men [22]. In addition, when diagnosed with type 2 diabetes, male patients tend to have an earlier onset age and a lower BMI [23]. However, female diabetic patients face a greater burden of risk factors at diagnosis, such as higher blood pressure and weight gain, a trend that is particularly prominent among white women and younger women [24, 25].
Diabetic peripheral neuropathy (DPN), a severe compli-cation of type 2 diabetes mellitus (T2DM), exacerbates the risk of ulcers, nontraumatic amputations, and foot infec-tions due to the neurological damage it causes. Moreover, it can lead to long-term disability, imposing heavy economic and psychological burdens on patients [26]. Additionally, research has revealed the intricate interconnections among lower extremity vascular disease, diabetic foot, and diabetic retinopathy, suggesting a trend towards mutual exacerbation among these complications [27]. Correlation coefficients, derived through statistical methods, provide an objective measure of the associations between various factors and the risk of diabetic foot, allowing for more precise identifica-tion of high-risk patients for diabetic foot. However, they are data dependent, and the presence of missing, incorrect, or biased data may affect the credibility of the prediction results. The ROC curve graphically displays the sensitiv-ity and specificity of a model at different threshold values, enabling an intuitive understanding of the model’s predic-tion performance. It can also be used to compare the pre-diction effects of different models or diagnostic methods. However, the accuracy of a ROC curve depends on the quality and quantity of the samples used. If the samples are biased or insufficient in number, the evaluation results of a ROC curve may be affected. The chi-square test has a broad scope of application and is suitable for various types of data analysis, especially for categorical variable data, such as age, gender, duration of diabetes, complica-tions, and their associations with the risk of diabetic foot. However, the chi-square test can determine only associa-tions and cannot establish causality. The t test is a classic statistical method used to determine whether the difference between the means of two samples is significant. It has high statistical power and can accurately judge whether there is a significant difference between two sets of data, with a wide range of applicability and clear results. However, the t test generally assumes that the data follow a normal distribu-tion or an approximately normal distribution. If the data dis-tribution deviates significantly from a normal distribution, the results of the t test may be affected. The Kaplan‒Meier method constructs survival curves entirely on the basis of empirical data without requiring assumptions about the dis-tribution of the data, making it applicable to various types of data. It visually presents survival rates over time in an easy-to-understand graphical format. However, it cannot directly control or adjust for the influence of confounding factors, which may lead to biased estimates of survival rates. The mean and standard deviation can reflect the central ten-dency and dispersion of data, providing a more intuitive representation of the data. However, they are susceptible to extreme values and units, which limits their application to a certain extent. The Cox proportional hazards regres-sion model is a semiparametric model that does not require strict assumptions about the distribution of survival times, making it more flexible and widely applicable in practical applications. However, although the Cox proportional haz-ards regression model is based on the proportional hazards assumption, this assumption may not hold in some cases. For example, when the interaction between the independent variables and time is significant, the hazard ratio may vary over time, leading to potential biases in the model’s results. Additionally, the model is sensitive to outliers and missing values when data are deleted.
Machine learning methods
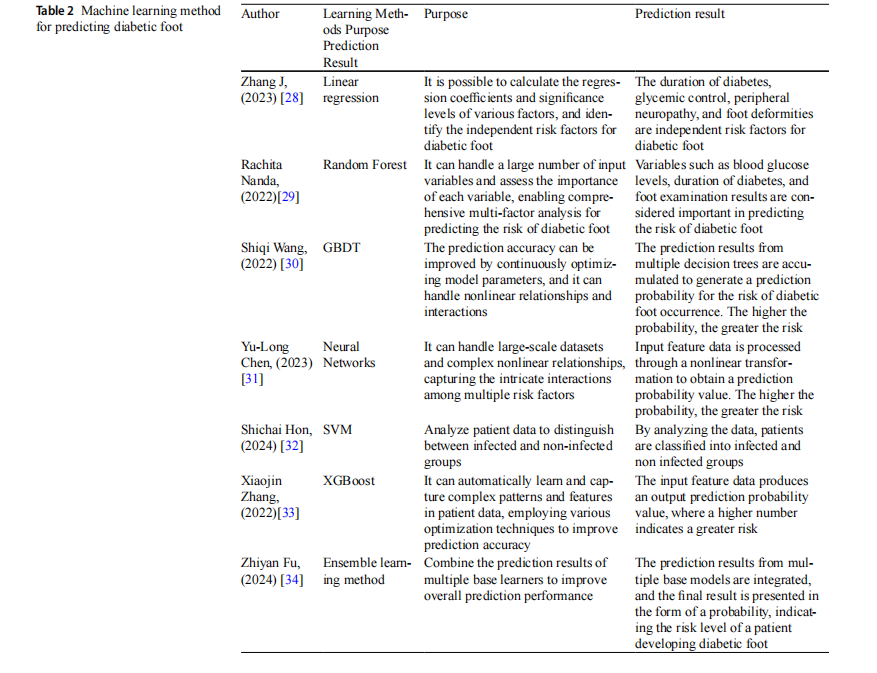
Compared with statistical methods, machine learning methods can handle more complex data relationships and uncover hidden risk factors. Common machine learning methods include decision trees, random forests, support vec-tor machines, and gradient boosting trees. These methods automatically learn the nonlinear relationships between risk factors and diabetic foot through training on large amounts of data and constructing efficient prediction models. The common machine learning methods and their applications in diabetic foot risk prediction are summarized in Table 2 for further research and application.
With the rapid development of big data and artificial intelligence technologies, machine learning (ML) has been increasingly applied in the field of diabetic foot ulcer (DFU) risk prediction. Advanced algorithms such as support vector machines (SVMs), random forests, and gradient boosting decision trees (GBDTs) have demonstrated unprecedented potential in DFU risk prediction because of their exceptional data processing and prediction capabilities. For example, researchers have successfully utilized SVMs and backprop-agation neural networks (BPNNs) to construct predictive models for the recurrence risk of DFUs. Through compari-sons of algorithm performance, it has been confirmed that machine learning models outperform traditional statistical methods in terms of prediction accuracy. However, SVMs have limited processing capabilities for high-dimensional data, and neural networks typically require a large amount of training data to avoid overfitting, with the training process potentially being very time-consuming. Schäfer et al. [10] further utilized machine learning to predict the risk of DFU and amputation in patients with high-risk factors, consid-ering their socioeconomic background and medical history information. A study by Goyal et al. [11] demonstrated the accuracy of machine learning in identifying signs of isch-aemia and infection in DFU images. Furthermore, machine learning has been innovatively applied to the analysis of foot thermograms in smartphone applications, enabling early detection of DFU [12]. Thermography technology allows noninvasive, convenient, and easily repeatable foot temperature measurements in diabetic patients [35], facili-tating early detection and regular monitoring programs and thereby limiting the incidence of disability-related condi-tions associated with diabetic foot disease.
Random forest predicts by integrating multiple decision trees, which can significantly improve the prediction accu-racy and handle datasets with many features well. However,
when the number of decision trees included in the experi-ment is excessive, the space and time costs required for the training process of the random forest algorithm also increase.
XGBoost, as an efficient machine learning algorithm, excels in processing both structured and unstructured data, achieving higher accuracy than other algorithms do. It can also handle data issues such as missing values and outli-ers. However, XGBoost has many parameters that need to be tuned, requiring considerable time and effort to find the optimal parameter combination. Additionally, it is suscep-tible to the influence of outliers or noisy data. Ensemble learning can improve prediction accuracy by combining the predictions of multiple learners, and it has a certain degree of tolerance for errors and outliers from individual learners.
However, in practical applications, it requires training mul-tiple learners, resulting in higher computational complexity. Notably, machine learning is not a blind computation process but rather a process of intelligently extracting reasonable answers on the basis of specific inputs. In sum-mary, ML algorithms create a mathematical model that maps “features” (i.e., observational variables) to “labels” (i.e., outcome variables) [13]. In this process, precise definitions of complex features and labels are crucial. This model not only facilitates early identification of complications such as severe infections but also provides a solid foundation for improving the clinical outcomes and prognosis of patients with diabetic foot ulcers (DFUs).
Deep learning methods
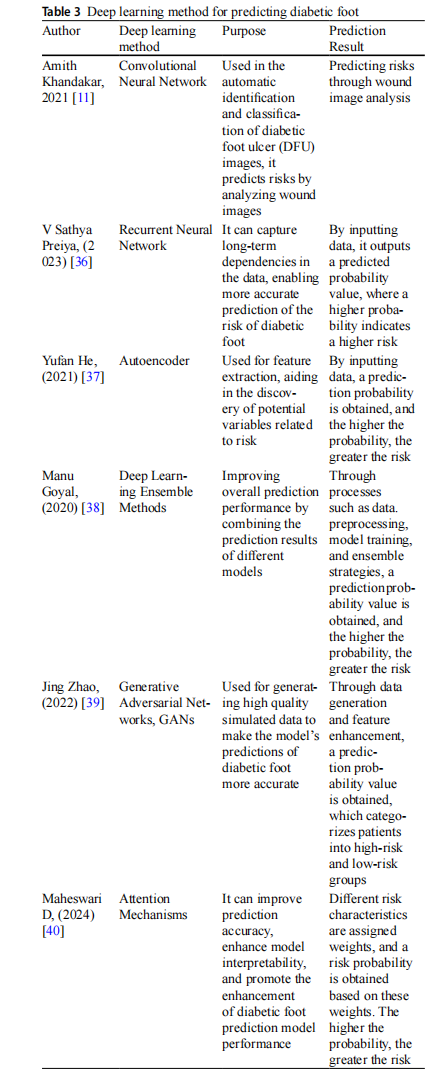
The deep learning method, as a cutting-edge branch of machine learning, has also demonstrated great potential in predicting the risk of diabetic foot disease. Deep learning is capable of automatically extracting high-level feature representations from raw data, thereby more accurately capturing the complex relationships between risk factors and diabetic foot. Common deep learning methods include convolutional neural networks (CNNs) and recurrent neural networks (RNNs). These methods have unique advantages in processing time series data, image data, and other types of information, providing new insights for predicting the risk of diabetic foot. A summary of common deep learn-ing methods and their applications in predicting the risk of diabetic foot is presented in Table 3 for further research and application [11, 36–40].
Deep learning is an important branch of machine learn-ing that uses artificial neural networks and large datasets to solve computationally complex problems. By mimick-ing the structure and function of the human brain’s neural networks, it achieves automatic learning and feature extrac-tion from complex data. In the diagnosis of diabetic foot, deep learning models can automatically extract valuable features from images, signals, and other data related to diabetic foot, thereby enabling accurate classification and prediction. This study provides new ideas and methods for the diagnosis and staging of diabetic foot disease. By con-structing deep learning models based on images and PPG signals, early screening and accurate staging of the diabetic foot can be achieved, providing timely and effective treat-ment recommendations for patients. Research has shown that the use of convolutional neural network (CNN) mod-els is more effective in identifying ischaemia and infection. Compared with manual machine learning algorithms, the integrated CNN deep learning algorithm performs better in both classification tasks, with an accuracy rate of 90% for ischaemia classification and 73% for infection classification [11]. However, CNNs have high requirements for data qual-ity and consume significant computational resources, which can be a challenge for resource-constrained environments.The integration of attention mechanisms and deep learn-ing methods can improve model performance and enhance model interpretability. However, in practical applications, they have high computational complexity and complex parameter tuning, requiring longer training times and more computational resources.
Generative adversarial networks (GANs) possess pow-erful data generation capabilities and flexible model struc-tures, which can improve model accuracy when applied. However, their drawbacks include the difficulty of training and high computational resource requirements. Autoencod-ers can extract features highly related to the risk of diabetic foot from complex medical data, improving the accuracy and efficiency of predictions. They can also detect anoma-lies in the input data. However, autoencoders tend to per-form poorly when testing data.
Richness of predictive factors
The predictive factors of the diabetes foot risk prediction model cover multiple aspects, including patients’ basic information (such as age, sex, BMI, etc.), duration of dia-betes and complications (such as retinopathy, peripheral neuropathy, etc.), foot examinations (such as dorsalis pedis artery pulsation, abnormal changes in foot skin, etc.), bio-mechanical parameters (such as plantar pressure, plantar soft tissue stiffness, etc.), and laboratory tests (such as gly-cated haemoglobin, ankle‒brachial index, etc.). The com-prehensive application of these predictive factors enables the model to assess patients’ risk of developing diabetic foot more comprehensively.
Factors related to underlying diseases
Duration of diabetes: The longer the duration of diabetes is, the greater the risk of developing diabetic foot [41]. With a longer duration of diabetes, the likelihood of distal lower limb vascular pathology increases, and conditions such as atherosclerosis in the lower limb blood vessels can lead to inadequate blood supply to the lower limbs. Long-termdiabetes may also affect the dilation and contraction func-tions of blood vessels, increasing the susceptibility of lower limb blood vessels to damage when subjected to external pressure. A prolonged duration of the disease can also exac-erbate distal lower limb neuropathy, reducing or even elimi-nating patients’ sensitivity to sensations such as pain and temperature. Motor neuropathy may lead to issues such as atrophy of foot muscles and decreased muscle strength, fur-ther affecting patients’ ability to walk and stand and increas-ing the risk of developing diabetic foot.
Blood glucose control status: Patients with poor blood glucose control, such as those with elevated fasting plasma glucose (FPG) levels and glycated haemoglobin (HbA1c) levels [42], are more prone to neuropathy and angiopathy, thereby increasing the risk of diabetic foot. When diabetic patients have poor blood glucose control, hyperglycaemia for an extended period can cause damage to blood vessels and nerves. This damage can lead to lower limb vascular and neuropathic complications, thereby increasing the risk of developing diabetic foot. Hyperglycaemia also provides favourable conditions for bacterial growth, increasing the risk of foot infections.
Factors related to vascular pathology
Peripheral Arterial Disease: Peripheral arterial disease is an important risk factor for diabetic foot, with a hazard ratio as high as 3.43 [43]. Vascular pathology leads to impaired blood circulation in the lower limbs, affecting wound
healing. Macrovascular disease can cause insufficient blood supply to the lower limbs, triggering ischaemic pain in the limbs. In severe cases, it can lead to intermittent claudica-tion, resting pain, and even limb necrosis. Vascular stenosis and occlusion not only affect the blood supply to the feet but also increase the risk of lower limb infections, ulcers, and gangrene.
Factors related to neuropathy
Peripheral neuropathy: Peripheral neuropathy is another important risk factor for diabetic foot, with a hazard ratio of 2.09 [44]. Neuropathy leads to a decrease or loss of sensa-tion in the feet, making patients susceptible to foot injuries from trauma, burns, etc. When the feet are injured, patients may be unable to detect it in a timely manner, leading to delayed treatment, an increased risk of infection, and ulti-mately triggering diabetic foot. The autonomic nerves are responsible for regulating skin temperature, humidity, and sweat secretion. When the autonomic nerves are damaged, these functions become abnormal, leading to issues such as dry and cracked skin, which further increases the risk of foot
Factors related to other complications
Retinopathy: Retinopathy is associated with diabetic foot, with a hazard ratio as high as 6.42 [45]. Retinopathy may reflect the status of systemic microvascular pathology and increase the risk of diabetic foot. The occurrence of reti-nopathy indicates the presence of microvascular pathology in the patient’s body, which may also affect the blood ves-sels in the lower limbs.
Nephropathy: Conditions such as microalbuminuria are also among the risk factors for diabetic foot. Patients with kidney disease often have systemic vascular pathology and metabolic disturbances, which increase the risk of foot com-plications [43]. These patients typically experience vascular pathology that leads to poor blood circulation in the lower limbs. The occurrence of diabetic foot is closely related to impaired blood circulation in the lower limbs; thus, patients with kidney disease are more prone to developing diabetic foot. Kidney disease can also exacerbate neuropathy in dia-betic patients, especially neuropathy in the lower limbs. Neuropathy reduces or eliminates patients’ sensitivity to sensations such as pain and temperature, thereby increasing the risk of foot injuries and infections and affecting the heal-ing of the diabetic foot.
Lifestyle habits and environmental factors
Smoking: Smoking is an independent risk factor for dia-betic foot, and smokers have a significantly increased risk of developing diabetic foot [46]. Smoking exacerbates vascu-lar and neuropathic complications, affecting the blood sup-ply and nerve sensation in the lower limbs and increasing the susceptibility of the feet to injury and infection. Improper foot care: Improper foot care, such as wearing unsuitable footwear and socks and improper nail trimming [47], can lead to foot injuries and infections. Improper foot care can also accelerate the progression of diabetic foot pathology, exacerbate existing symptoms, and accelerate the process of diabetic foot deterioration.
Rigorousness of model evaluation and validation
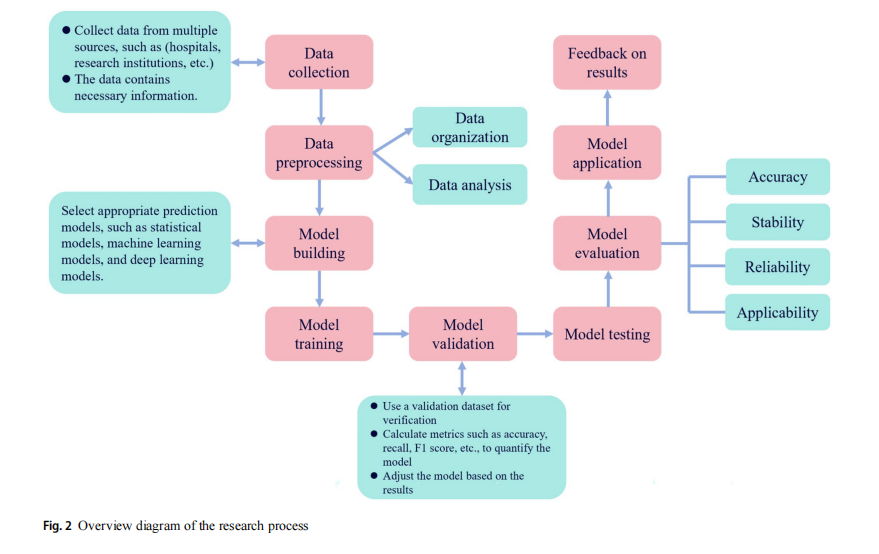
The overall construction of a risk prediction model for dia-betic foot disease is a complex and systematic process aimed at assessing the risk of diabetic patients developing diabetic foot disease through statistical analysis and machine learn-ing techniques. The specific process is shown in Fig. 2. The process begins with data collection from various sources,such as hospitals and medical institutions, ensuring that the collected data contain all of the necessary information. Next, the data are organized and analysed. On the basis of these data, an appropriate prediction model (statistical model, machine learning model, or deep learning model) is selected. The selected algorithm is then trained on the training dataset to obtain a preliminary prediction model. This model is further validated via a validation dataset, with metrics such as accuracy and recall being calculated to quantify the model’s performance. Adjustments are made to the model on the basis of these results. Model testing and evaluation are subsequently conducted to assess the model’s accuracy, stability, reliability, and applicability. Finally, the model is applied in practical settings (such as communities and hospitals), and feedback is obtained on the basis of the
Selection and processing of predictive factors
The selection of predictive factors should be based on sci-entific research and clinical experience, covering multiple aspects of the occurrence and development of diabetic foot, such as underlying diseases, vascular pathology, neuropathy, lifestyle habits, and environmental factors. The processing of continuous and categorical variables needs to be scientific and reasonable, maintaining the continuity and authenticity of the data to avoid distortion or oversimplification.
Selection of modelling methods
Comprehensive data related to the risk of diabetic foot,including but not limited to the patient’s age, sex, duration of diabetes, blood glucose control status, foot examination results, lifestyle habits (such as smoking and alcohol con-sumption), and complications (such as kidney disease and retinopathy), were collected. Data preprocessing, which includes handling missing values, detecting outliers, data normalization, etc., is necessary before modelling to ensure the quality and consistency of the data. During the model-ling process, it is necessary to screen out features closely related to the risk of diabetic foot to improve the prediction accuracy and efficiency of the model. Choosing the right model is crucial for successful modelling. Each model has its own characteristics and applicable scenarios, and the choice should be based on the characteristics of the data and prediction requirements.
Evaluation metrics for model performance
The area under the receiver operating characteristic (ROC) curve (AUC) [48] was used as the primary metric to evalu-ate the predictive performance of the model. The closer the AUC value is to 1, the better the predictive performance of the model. Additionally, other evaluation metrics, such as sensitivity, specificity, positive predictive value, and nega-tive predictive value, can also be considered to comprehen-sively assess the model’s predictive performance.
Rigorousness of model validation
(1) Internal Validation: Internal validation of the model is conducted through data splitting methods (such as the bootstrap method) [49] or cross-validation methods (such as K-fold cross-validation) [50] to assess the sta-bility and reliability of the model on the training dataset. Internal validation helps to identify potential overfitting or underfitting issues in the model during the training process and allows corresponding adjustments and opti-mizations to be made.
(2) External Validation: External validation of the model is conducted via a new dataset that is independent of the training dataset to assess the model’s prediction accuracy and generalizability to unknown data. Exter-nal validation is a crucial step in assessing the practi-cal application value of the model, as it ensures that the model maintains a stable predictive performance across different populations and environments.
(3) Sensitivity Analysis and Robustness Testing: Sensitiv-ity analysis is conducted on the key predictive factors in the model to assess their degree of influence on the model’s prediction results. Robustness testing is per-formed to evaluate the stability and reliability of the model under different conditions, such as missing data and outlier handling.
Results
Statistical methods
A logistic regression model, as a classic method, can inte-grate information from multiple variables (up to more than10), providing personalized risk assessments for patients with a prediction accuracy rate of over 80%. Key risk fac-tors, such as age (especially for patients over 60 years old) and smoking, have been extensively studied and confirmed to be closely associated with the risk of diabetic foot ulcer-ation (DFU). Smoking can increase the recurrence rate of DFU by approximately 50%. Furthermore, sex differences are also significant for diabetes and its complications, with a higher incidence rate among males than females. However, females face more risk factors when they are diagnosed.
Machine learning methods
The ability of machine learning to predict the risk of diabetic foot ulcers (DFUs) is becoming increasingly widespread, and its powerful data processing capabilities enable us to uncover more complex and hidden risk factors. Compared with traditional statistical methods, machine learning algo-rithms such as decision trees, random forests, support vec-tor machines (SVMs), and gradient boosting decision trees (GBDTs) can automatically learn the nonlinear relation-ships between risk factors and diabetic foot ulcers (DFUs) through extensive data training, enabling the construction of efficient prediction models.
Deep learning methods
Deep learning has tremendous potential in predicting the risk of diabetic foot ulcers (DFUs). By simulating the neural networks of the human brain, it extracts high-level features from data, accurately capturing the connections between risk factors and DFUs. Common methods such as convolutional neural networks (CNNs) and recurrent neu-ral networks (RNNs) have advantages in processing spe-cific data, enabling automatic feature extraction and precise predictions, which aid in diagnosis and staging. Deep learn-ing models based on images and PPG signals can perform early screening and accurate staging of diabetic foot ulcers (DFUs). Convolutional neural networks (CNNs) excel in identifying ischaemia and infection, but they have high requirements for data quality and computational resources.
Discussion
In this systematic review and meta-analysis, we conducted a thorough examination and integration of a vast array of literature, deeply exploring the key factors influencing the development of diabetic foot ulcers (DFUs) as well as the effectiveness of preventive intervention measures. Using statistical methods, we identified the significant roles of variables such as age, gender, duration of disease, blood glucose levels, smoking habits, and neurovascular pathol-ogy in the occurrence and progression of DFU. These find-ings not only provide a scientific basis for our understanding of the pathogenesis of DFU but also offer important refer-ences for formulating targeted prevention and treatment strategies. Furthermore, we have also attempted to apply machine learning methods in predicting and assessing the risk of DFU. By training machine learning models, we suc-cessfully identified DFU patients with high-risk factors and validated the accuracy of machine learning in recognizing signs of ischaemia and infection in DFU images. The deep learning model integrates patients’ historical data, images, and textual information to accurately identify the risk of foot complications, enabling early screening of diabetic foot ulcers. These discoveries not only expand the application scope of machine learning and deep learning in the medical field, but also provide new technological means for the early diagnosis and treatment of DFU. However, when exploring the effectiveness of comprehensive care in reducing the risk of DFU, we encountered the challenge of low certainty evi-dence. This suggests that in future work, we need to integrate data from multiple studies through systematic reviews and meta-analyses, expand the sample size to enhance the cer-tainty of evidence; design rigorous randomized controlled trials to ensure comparability between the intervention and control groups, effectively reducing bias; conduct long-term follow-ups to assess the sustained effects of comprehensive nursing; and simultaneously incorporate real-world data to address the limitations of clinical trials, comprehensively validating the effectiveness of comprehensive nursing. Deep learning models are capable of efficiently processing com-plex clinical data and have demonstrated excellent perfor-mance in early screening for diseases such as diabetic foot ulcers, assisting doctors in identifying risks earlier. How-ever, their limited interpretability and lack of transparency in the decision-making process make it difficult for doctors to understand the reasoning logic of the models, which may affect their trust in the results. In future work, a comprehen-sive evaluation of the models should be conducted through a combination of external validation and clinical validation. Specifically, the generalization ability of the models should be tested on independent datasets to ensure their reliability across different populations and scenarios, and the model predictions should be compared with clinicians’ diagnoses to assess consistency and accuracy. Additionally, interpret-ability techniques can be leveraged to reveal the decision-making basis of the models and help doctors understand the key features. In the initial stages, the models can be used as auxiliary tools, with doctors retaining the final decision-making authority, to gradually build trust. Doctors should critically assess the model results in combination with clini-cal experience, while actively exploring efficient modes of collaboration to improve the overall quality of medical decision-making
Conclusions
In summary, this systematic review and analysis not only uncovered the key factors influencing the development of DFU but also explored the potential application of machine learning in predicting DFU risk and the effectiveness of comprehensive care in reducing DFU risk. Although we have made significant progress in some areas, there are still issues and challenges that need to be addressed. In the future, the development of diabetic foot ulcer (DFU) risk prediction models will focus more on model optimization and personalization. By continuously collecting and ana-lysing new clinical data, we anticipate the emergence of more accurate and personalized prediction models, which will assist doctors in formulating more precise prevention and treatment plans, thereby increasing the effectiveness of DFU prevention and treatment success rates. Moreover, research on DFU prevention intervention measures, espe-cially comprehensive care methods for high-risk popula-tions and interventions specifically targeting populations with low to moderate ulcer risk, is needed. By designing and conducting high-quality randomized controlled trials, we can provide a more solid scientific basis and technical support for the prevention and treatment of DFU. Finally, we call on the medical community and all sectors of soci-ety to work together, strengthen their emphasis and support for DFU prevention and control efforts, and jointly promote progress in diabetic foot prevention and treatment.
Author contributions HX Q and T Z: methodology, data analysis,writing-original draft, and review and editing. LJ H, Q L, and RP H conceptualization and writing the original draft. LH M: proofreading and reviewing and editing the final draft of the manuscript. All authors contributed to the article and approved the submitted version.
Funding This research is granted from the National Natural Science Foundation of China (No. 72264022), Lanzhou Science and Technol-ogy Planning Project (2023-ZD-95), the First Hospital of Lanzhou University (ldyyyn2022-97), and the Gansu Provincial Natural Sci-ence Foundation (25JRRA559).
Declarations
Conflict of interest The authors declare that they have no known com-peting financial interests or personal relationships that could have ap-peared to influence the work reported in this paper.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.o rg/licenses/by/4.0/.

This article is excerpted from the 《Acta Diabetologica》 by Wound World.
