
Introduction
Neonatal diabetes mellitus (NDM) is defined as diabe-tes with onset before 6–12 months of age and occurs in approximately 1 in 100,000 live births [1, 2]. Among indi-viduals diagnosed with NDM, nearly half are caused by heterozygous activating mutations in the ATP-dependent Potassium (KATP) channel genes: KCNJ11 or ABCC8 and can usually be treated successfully with oral sulfonylureas rather than insulin injections [3–7]. In addition to hyper-glycemia, affected individuals also exhibit divergent neu-rodevelopmental features which arise from the presence of altered KATP channels in the brain. Although many reports have suggested that sulfonylurea treatment may improve neurodevelopmental functioning, the degree to which improvement is possible, and the factors on which it may depend remain uncertain [8–12].
Several studies have shown that more severe neurologi-cal phenotypes in KATP-NDM are often related to specific mutations: DEND (developmental delay, epilepsy, and neonatal diabetes) with certain rare mutations, and iDEND (intermediate DEND) with the relatively common V59M mutation, for example. However, other less obvious features appear to be common even in those with mutations not as definitively associated with a neurological phenotype, such as learning disorders and attention-deficit/hyperactivity dis-order (ADHD) [13, 14]. Additional careful investigation by our group and others using validated neuropsycho-logical assessments has revealed that affected individuals frequently exhibit a wide range of neurodevelopmental difficulties including decreased social interactions and flex-ibility/adaptability, increased atypicality, and the presence of psychiatric disorders [15–17]. While several of these studies have noted concerns about social functioning on a variety of measures, it remains unclear how often individu-als with KCNJ11 mutations have impairment at a level seen in those with autism spectrum disorders (ASD), which is an additional co-morbid diagnosis among some within this population. Lastly, anxiety has rarely been directly assessed and to our knowledge grit (i.e. perseverance in settings of adversity) has not been measured, but both are important aspects of functioning within individuals with any type of chronic condition and/or neuroatypicality. Studies on anxi-ety in other chronic conditions such as type 1 diabetes sug-gest the importance of early identification and management to optimize long term well-being [18, 19].
In this study, we assessed self- and/or parent/caregiver-completed surveys on anxiety, grit, and social responsive-ness in participants with KCNJ11-NDM and their unaffected sibling controls. We hypothesized that participants with KCNJ11-NDM would score worse on measures of social responsiveness, report more anxiety, and report less grit than their unaffected siblings.
Methods
Compliance with ethical standards
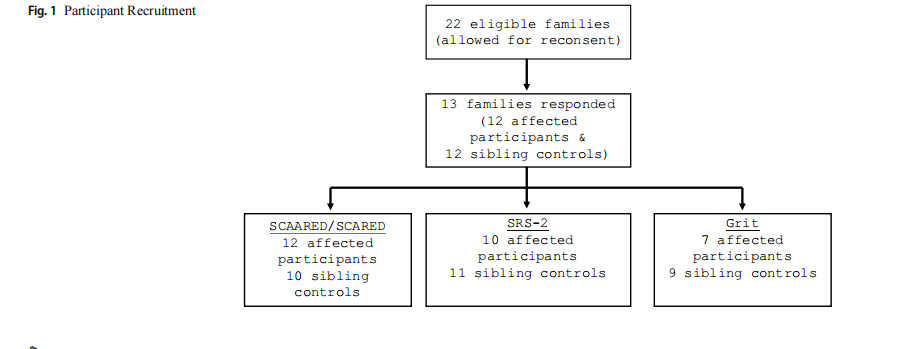
Participants with KCNJ11-NDM and their unaffected sib-lings were recruited and consented for this study through the University of Chicago Monogenic Diabetes Registry (http:// monogenicdiabetes.uchicago.edu/registry/). This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of University of Chicago (IRB 6858, 15617B, 16935B) (Fig. 1). The Registry gathers extensive longitudinal data about monogenic diabetes participants, such as diabetes diagno-sis and treatment data, other medical problems, diabetes genetic testing results, and family history information [20].
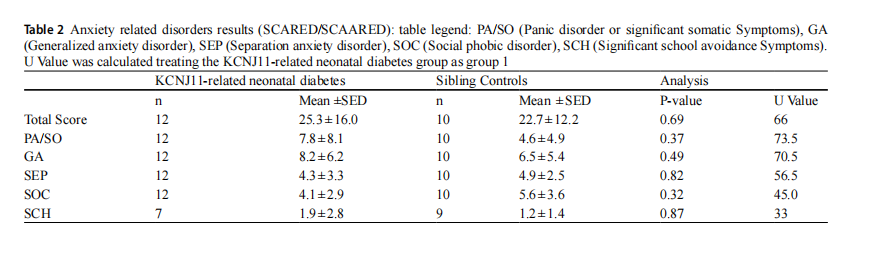
Three standardized behavioral and neuropsychological surveys were given to each participant and/or parent/care-giver: the Screen for Adult/Child Anxiety Related Disorder (SCAARED/SCARED) [21], the Social Responsiveness Scale, Second Edition (SRS-2) [22], and Grit Scale [23, 24]. SCAARED/SCARED generates a total score as well as scores for following subscores: Panic Disorder or Sig-nificant Somatic Symptoms (PA/SO), Generalized Anxi-ety Disorder (GAD), Separation Anxiety Disorder (SEP), Social Phobic Disorder (SOC), Significant School Avoid-ance Symptoms (SCH). The scores range from 0 to 62, with a score ≥25 indicating the presence of an Anxiety Disorder for child reports (child self-report or parent-report) and a score ≥23 indicating the presence of an Anxiety Disorder for adult self-report.
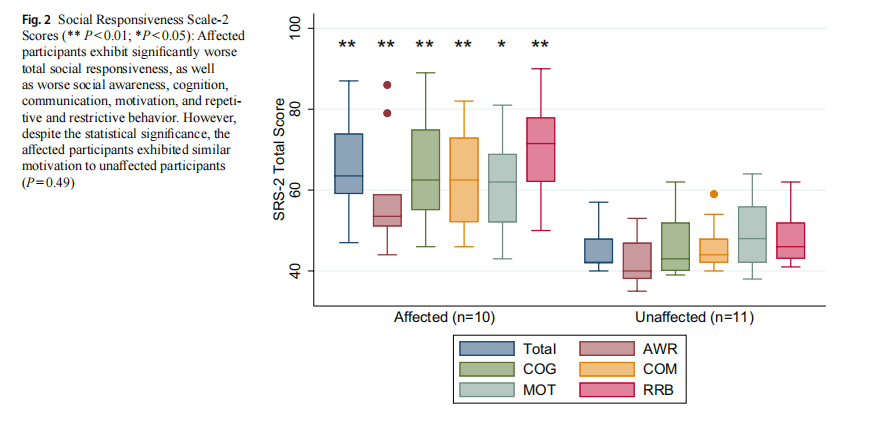
We chose the SRS-2 for describing a total social respon-siveness score, as well as five content areas of social func-tioning including Social Awareness (AWR), Cognition
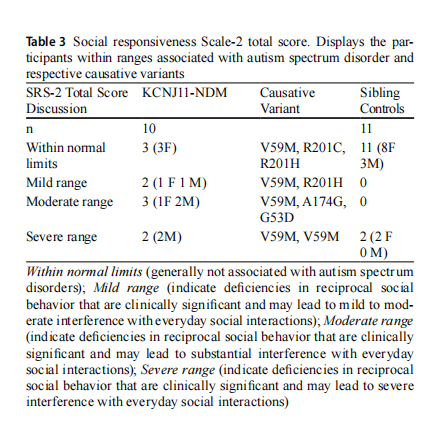
(COG), Communication (COM), Motivation (MOT), and Restricted Interests and Repetitive Behavior (RRB) for children, adolescents, and adults. The total score and other scores are reported as T-scores from a range of 0 to 90. A total T-score ≤59 is within normal limits, 60-65 is mild range, 66-75 is moderate range, and ≥76 is considered severe range.
The SRS-2 and SCAARED/SCARED generated scaled scores that could be analyzed despite differences in partici-pant age, enabling a greater cohort of participants. In situ-ations where both a self- and parent-reported form were completed, the self-report was used for analysis, unless oth-erwise indicated.
The Grit Scale measures the extent to which individuals can maintain focus and interest and persevere in obtaining long-term goals. A high grit score indicates that the individ-ual is resilient, persistent, and able to overcome obstacles to successfully achieve their goals [23]. Grit scores range from 1 to 5, with 5 being the maximum score and indicating the highest level of grit.
To compare the three measures, nonparametric analyses were performed using the Mann-Whitney U-test for group comparisons with Stata 19 (StataCorp LLC, College Sta-tion, TX) for statistical analysis. Results are expressed as mean±standard deviation (SD) unless indicated, and group differences were considered significant if P<0.05.
Results
Participants
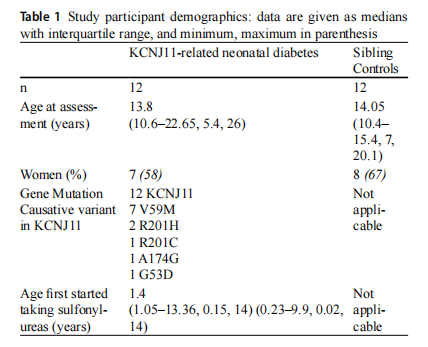
Twelve participants with KCNJ11-NDM and twelve unaf-fected sibling controls participated in this study. The median age at assessment was 13.8 years for KCNJ11-NDM par-ticipants and 14.1 years for sibling controls (Table 1). Com-parison of the mutations of affected participants in the study versus affected individuals not in the study did not reveal any distinct differences that may have preferentially influ-enced participation in the study. See Figures S1-S2 in the Supplementary Material for comprehensive demographic information as well as comparisons of mutations.
SCAARED/SCARED results
From the SCAARED/SCARED, the mean total anxiety score was 25.3 (±16.0) for KCNJ11-NDM participants and 22.7 (±12.2) for unaffected sibling controls. Statistical analyses revealed no significant differences in the mean total anxiety scores (P=0.69), as well as all subscores, in KCNJ11-NDM versus unaffected sibling participants (Table 2).
Despite there being no statistically significant differ-ences, it is important to note that according to SCAARED/ SCARED clinical categorization, seven out of twelve par--ticipants (58%) with KCNJ11-NDM and four out of ten sib-ling controls (40%) met criteria for an anxiety disorder by either self- or parent-report. Of note, one affected partici-pant met criteria for an anxiety disorder on the parent-report form but did not meet criteria for an anxiety disorder on the self-report form, and one sibling control met criteria for an anxiety disorder on the self-report form but did not meet criteria for anxiety on the parent-report form.
SRS-2 results
The mean total SRS-2 score was 66.2 (±13.1) for KCNJ11-NDM and 45.9 (±6.1) for unaffected siblings. KCNJ11- NDM participants displayed significantly worse SRS-2 mean scores than unaffected sibling controls (P< 0.001) as well as significantly worse subscores. The association appeared to be less strong for the Motivation subscore (P = 0.029) (Fig. 2).
Additional analysis of the clinical categorization revealed that 7 out of 10 KCNJ11-NDM participants (70%) had scores within a range consistent with mild (n = 2), moderate (n = 3), or severe (n = 2) associations with autism spectrum disorder while 0 out of 11 sibling controls (0%) had scores within a range consistent with autism spectrum disorders (Table 3). There was no clear association with mutation with the severity category
Grit results
Grit generates a single grit score, which was 3.3±0.5 for affected participants and 3.4±0.4 for unaffected partici-pants. Only 7 affected participants completed the Grit Scale. Statistical analysis revealed no significant differences in grit scores (P=0.46) (Table 4). The average grit scores reflect the mean on items for the whole group.
Discussion
In this study, we found that individuals with KCNJ11-NDM had significantly worse social responsiveness compared to their sibling controls, indicative of ASD. There was no group difference in assessment of anxiety or grit; however,

7 out of 12 with KCNJ11-NDM and 4 out of 10 unaffected siblings had scores indicative of an anxiety disorder by self-or parent-report.
Similar to previous studies by our group and others [16, 25, 26], showing a variety of struggles including social dys-function, individuals with KCNJ11-NDM exhibited signifi-cantly worse social responsiveness in both total scores, as well as on all five subscales including Social Awareness, Cognition, Communication, Motivation, and Restricted Interests and Repetitive Behavior. The association appeared to be less strong for the Motivation subscale. Out of the five subscales, Motivation is the only intrinsic measure, leading us to speculate that participants with KCNJ11-NDM may exhibit an internal sense of motivation, which can be con-nected to grit and self-resiliency.
Although the SRS-2 is not meant for diagnosis of ASD, our results support a strong association between KCNJ11- NDM and autism spectrum disorder [27]. This finding rein-forces the existing but limited data on the relation between these two conditions [26] and encourages providers to explore existing interventions in improving social compe-tencies in people with features of autism spectrum disorders [28]. We had a high participation rate of participants with V59M causative variant, but unexpectedly, they exhibited a range of scores associated with autism spectrum disor-der, including one without significant social concerns. This participant scored in the ‘normal’ range on their parent-completed SRS-2; there is no clear hypothesis as to why this participant would score better than other participants with V59M. One additional V59M participant scored in the 'mild' range. This participant was serendipitously exposed to sulfonylureas in utero, as has been described previously [29], which may explain why they scored better than other participants with V59M. Furthermore, a few individuals with mutations associated with a milder phenotype (such as R201H) had scores within a range concerning for autism spectrum disorder. This indicates that all affected individu-als should undergo comprehensive evaluation regardless of specific mutation. Although siblings had similar anxiety scores as affected participants, no siblings had SRS-2 scores suggestive of ASD, whereas 70% of the KCNJ11-NDM individuals had scores suggestive of ASD. This large dif-ference between affected participants and their unaffected siblings suggests that most of these families may not have a high background genetic risk for ASD, as may be the case in the general population [30], and the affected participants are likely to have “monogenic” ASD due to their KCNJ11 variant
Although individuals with KCNJ11-NDM did not exhibit significantly worse anxiety, both affected participants (7/12, 58%) and their sibling controls (4/10, 40%) scored in a range indicative of an anxiety disorder by self- or parent-report. These rates are higher than the overall lifetime prevalence of any anxiety disorder among adolescents in the US of 31.9% [31]. When one member of the family is impacted by a chronic disease such as T1DM, there can be increased psychological impact and anxiety on other unaffected mem-bers [32]. This notable finding highlights the importance of assessing anxiety levels not only with participants with KCNJ11-NDM, but also their siblings and other close fam-ily members.
Grit results were not significantly different when compar-ing individuals with KCNJ11-NDM to their sibling controls. The lack of significant differences of the Grit scores, which measure more intrinsic levels of personality, lead us to pos-tulate that participants with KCNJ11-NDM exhibit intrinsic grit
This study provides a greater understanding into the neu-rodevelopment difficulties individuals with KCNJ11-NDM may experience. These results can help improve patient clinical awareness: early screening for specific neurode-velopment difficulties such as social responsiveness can facilitate early intervention for individuals to help combat potential difficulties. To our knowledge, this is the first study investigating self- or parent/caregiver-reported grit in children and early adults with KCNJ11-NDM and to com-pare anxiety between them and their unaffected sibling con-trols. Additionally, our findings regarding heighted anxiety levels at the familial level encourage providers to advocate for greater support for families affected by KCNJ11-NDM.
We recognize that our sample size for this study is not very large, making it difficult to draw extensive conclusions about these neurodevelopment findings as representative of the KCNJ11-NDM community. However, even small sam-ples can be meaningful in rare disease research such as neo-natal diabetes. Additionally, questionnaires were completed by the participants and/or their family members instead of an external individual. This allows for potential personal biases or perceptions to affect the accuracy of the question-naire results.
Conclusions
In summary, individuals with KCNJ11-NDM have signifi-cantly worse social responsiveness than their sibling con-trols. Anxiety rates and grit are similar in individuals with KCNJ11-NDM compared to their sibling controls. Thus, it would be beneficial to monitor and check children with KCNJ11-NDM for social responsiveness challenges and anxiety challenges to obtain early support. Our findings sug-gest that unaffected siblings of individuals with KCNJ11-NDM may also benefit from an assessment for anxiety. Grit does not appear to be as different; individuals with KCNJ11-NDM exhibit self-resiliency and grit at rates simi-lar to sibling controls, which should support them achieving their individual goals in life.
Supplementary Information The online version contains supplementary material available at https://doi.org/10.1007/s00592-0 25-02598-w.
Acknowledgements The authors are very grateful to the patients and families who participated in this study through the UChicago Mono--genic Diabetes Registry (http://monogenicdiabetes.uchicago.edu).
Author contributions All authors contributed to the study conception and design. Data collection and analysis were performed by Jui Desai, Lisa Letourneau-Freiberg, Kristen Wroblewski, Megan Scott and Siri Greeley. All authors read and approved the final manuscript.
Funding This work was supported by the National Institute of Diabetes and Digestive and Kidney Disease R01DK104942 and P30DK020595, NIH CTSA UL1 TR000430 (REDCap support), and the Kovler Family
Data availability The datasets generated during the current study are available from the corresponding author on reasonable request.
Declarations
Conflict of Interest The authors declare that they have no conflict of
Ethics approval This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of University of Chicago (IRB 6858, 15617B, 16935B).
Consent to participate Informed consent was obtained from all par-ticipants (and/or legal guardians, in the case of minor participants) included in the study.
Open Access
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.o rg/licenses/by/4.0/.
This article is excerpted from the 《Acta Diabetologica》 by Wound World.
